
Abstract
Introduction:
Chronic obstructive pulmonary disease (COPD) is a leading cause of global morbidity and mortality, frequently complicated by acute exacerbation of COPD (AECOPD) that may result in cardiovascular stress. Emerging evidence suggests that cardiac injury, as indicated by elevated cardiac troponin I, may be associated with the severity and prognosis of AECOPD.
Objective:
This study aimed to evaluate cardiac troponin I levels in patients presenting with AECOPD and to investigate their correlation with disease severity, ventilatory requirements, length of hospital stays and mortality.
Methods:
A hospital-based cross-sectional study was conducted at the Department of Medicine, including 106 patients diagnosed with AECOPD. Serum cardiac troponin I levels were measured at admission. COPD severity was graded using Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria. Associations between cardiac troponin I levels and clinical outcomes were statistically analysed.
Results:
Elevated cardiac troponin I levels were observed in 55.7% of patients. A significant correlation was found between elevated cardiac troponin I levels and COPD severity (P < .01), increased need for ventilator support (74.6% vs. 36.2%; P < .01) and prolonged hospitalisation (7.47 vs. 5.75 days; P < .01). All mortality cases (3.8%) occurred in the cardiac troponin I-positive group, although this finding was not statistically significant (P = .128).
Conclusion:
Elevated cardiac troponin I levels are prevalent among AECOPD patients and significantly correlate with exacerbation severity, ventilatory support requirements and length of hospitalisation. While the association with mortality requires further exploration, cardiac troponin I may serve as a valuable prognostic biomarker for identifying high-risk patients and guiding clinical management during COPD exacerbations.
Introduction
According to Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023, ‘COPD is a heterogeneous pulmonary disorder marked by chronic respiratory symptoms, including dyspnoea, cough, sputum production, and/or exacerbations, resulting from airway abnormalities (bronchitis, bronchiolitis) and/or alveolar damage (emphysema), leading to persistent and progressive worsening airflow limitation’.[1]
Diagnosis of COPD
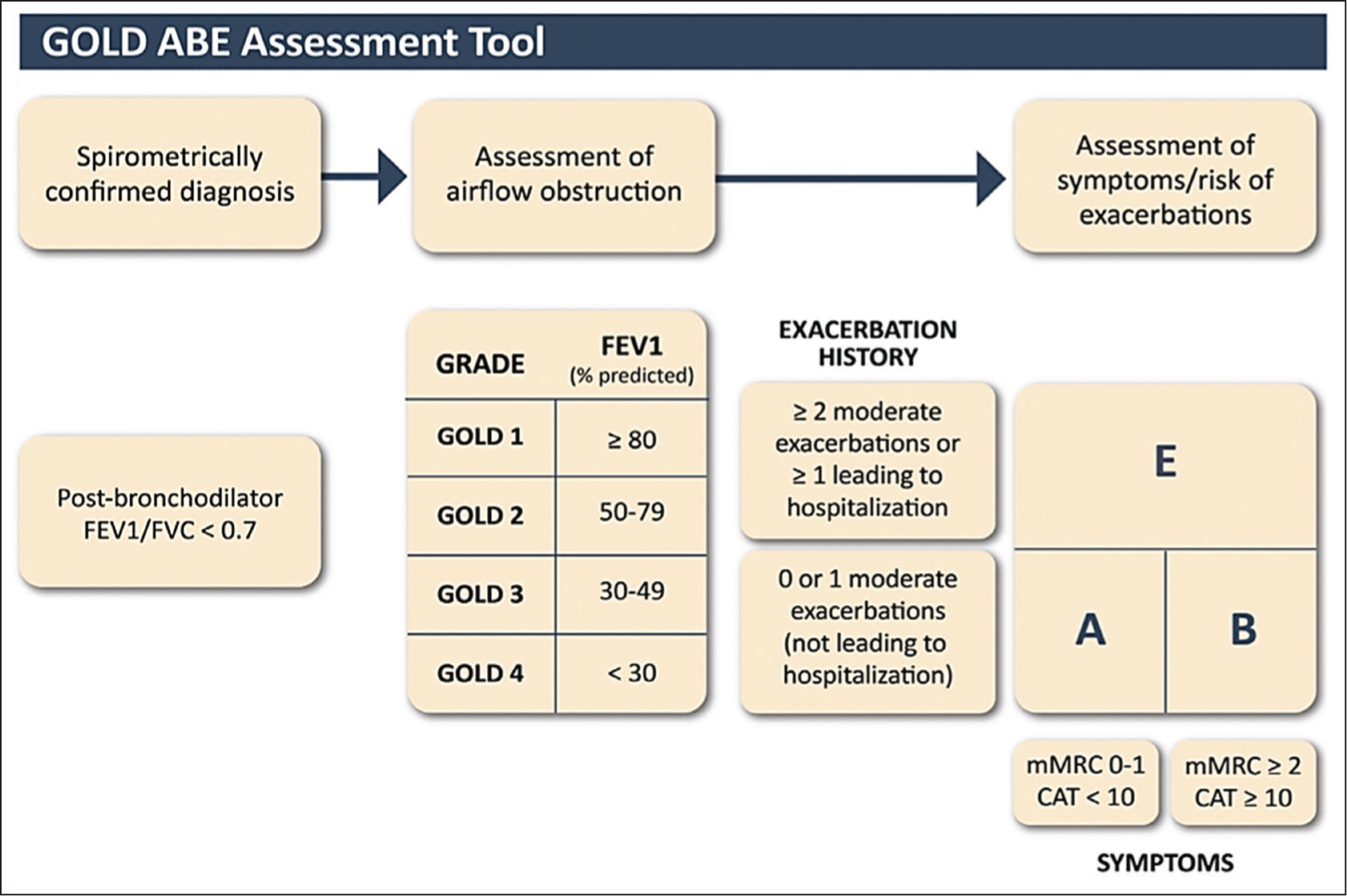
‘COPD should be considered in patients who present with symptoms such as shortness of breath, persistent cough or sputum production, particularly if they have a history of exposure to known risk factors. Confirming the diagnosis requires spirometry; a post-bronchodilator forced expiratory volume in 1 second/forced vital capacity (FEV1/FVC) ratio of less than 0.70 confirms the existence of persistent airflow limitation, indicating COPD’.[1]
A comprehensive assessment approach evaluates disease severity by considering symptom levels (using Modified Medical Research Counsil [mMRC] or COPD Assessment Test [CAT]), the degree of airflow limitation (classified from GOLD 1 to 4) and the history of past exacerbations as shown in Figure 1.[2–4]
GOLD classification of severity of COPD
COPD Exacerbations
Acute exacerbations of COPD (AECOPDs) are characterised by an exacerbation of patient symptoms that surpasses typical daily fluctuations, potentially necessitating an adjustment in the standard treatment regimen for those with underlying COPD.[4]
AECOPDs are empirically managed with antibiotics, despite substantial evidence indicating that ‘fewer than 50% of these episodes are linked to bacterial infections, and with prednisone, even though approximately 30% of the episodes do not correlate with lung or systemic inflammation’; this data indicates likely there is excessive use of antibiotics and steroids in the community.[5]
Cardiac Troponin I and AECOPD
Elevated troponin levels are observed in COPD patients, in the absence of acute coronary syndrome (ACS), complicating accurate diagnosis. Consequently, the identification of ST Elevation Myocardial Infarction (STEMI) is often postponed in COPD patients. Elevated cardiac troponin I levels in patients of AECOPD serve as an independent mortality risk factor, even in the absence of ACS, and may arise from several aetiologies.
The pathophysiology of increased troponins observed during an AECOPD may be related to the development of supply–demand mismatch to the myocardium due to tachycardia or coexisting left ventricular hypertrophy. Hypoxaemia and hypercapnia arising from an AECOPD can be pro-arrhythmogenic, leading to arrhythmias that may precipitate heart failure decompensation.[6] Troponin levels may rise due to elevated pulmonary pressures and hypoxia, resulting in right ventricular ischaemia and microinfarcts during an exacerbation.
Materials and Methods
Study Population
The study was approved by the Ethics Committee. In this study, 106 individuals were enrolled; after screening the subjects according to the inclusion and exclusion criteria.
Study Methodology
COPD and AECOPD were diagnosed according to the GOLD 2023.[1] A comprehensive medical history was taken; complete clinical examination and workup including chest X-ray, electrocardiogram (ECG), echocardiography and laboratory investigations were done. Cardiac troponin I samples were taken on admission and estimation was done by Getein cardiac troponin I fast test kit (immunofluorescence assay). The minimum detection level was 0.01 ng/mL. Pulmonary function testing was performed using a COSMED MicroQuark USB-PC-based spirometer to measure forced expiratory volume in first second (FEV₁) for assessing disease severity.
Outcome variables included need for intensive care unit (ICU) care, need for assisted ventilation (non-invasive/ invasive), length of hospitalisation and survival/ death.
Statistical Analysis
The quantitative data were expressed as the mean ± standard deviation (SD). Categorical and nominal data were represented as percentages. The t-test was employed for the analysis of quantitative data, while non-parametric data was assessed using the Mann–Whitney U test, and categorical data was evaluated with the chi-squared test. The Pearson correlation coefficient was utilised to calculate the correlation between quantitative variables. The significance level for the P value was established at <.05. All analyses were conducted utilising SPSS software version 21.
Result
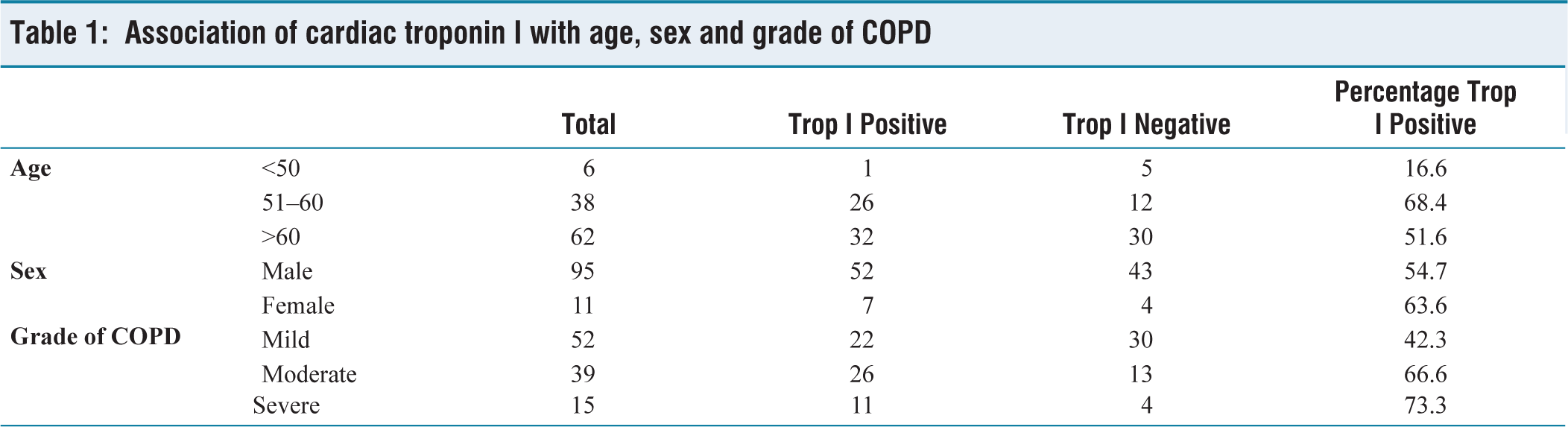
The mean age of the study participants was 61.58 years, with more than half of the cases (58.5%) belonging to the old age category (over 60 years). The study group had a male predominance, including 89.6% men and 10.4% females, resulting in a male-to-female ratio of 8.63:1. Elevated cardiac troponin I levels were observed in 55.7% of cases upon admission, whereas negative levels were noted in 44.3% of cases.
Out of the total 106 cases, 49.1% had mild symptoms, 36.8% had moderate symptoms and 14.2% had severe symptoms. Among the mild cases 42.3% had raised cardiac troponin I, 66.6% of the moderate cases had raised cardiac troponin I and 73.3% of the severe cases had raised cardiac troponin I, as shown in Figure 2 and Table 1.
Graph showing association of cardiac troponin I with age, sex and gender
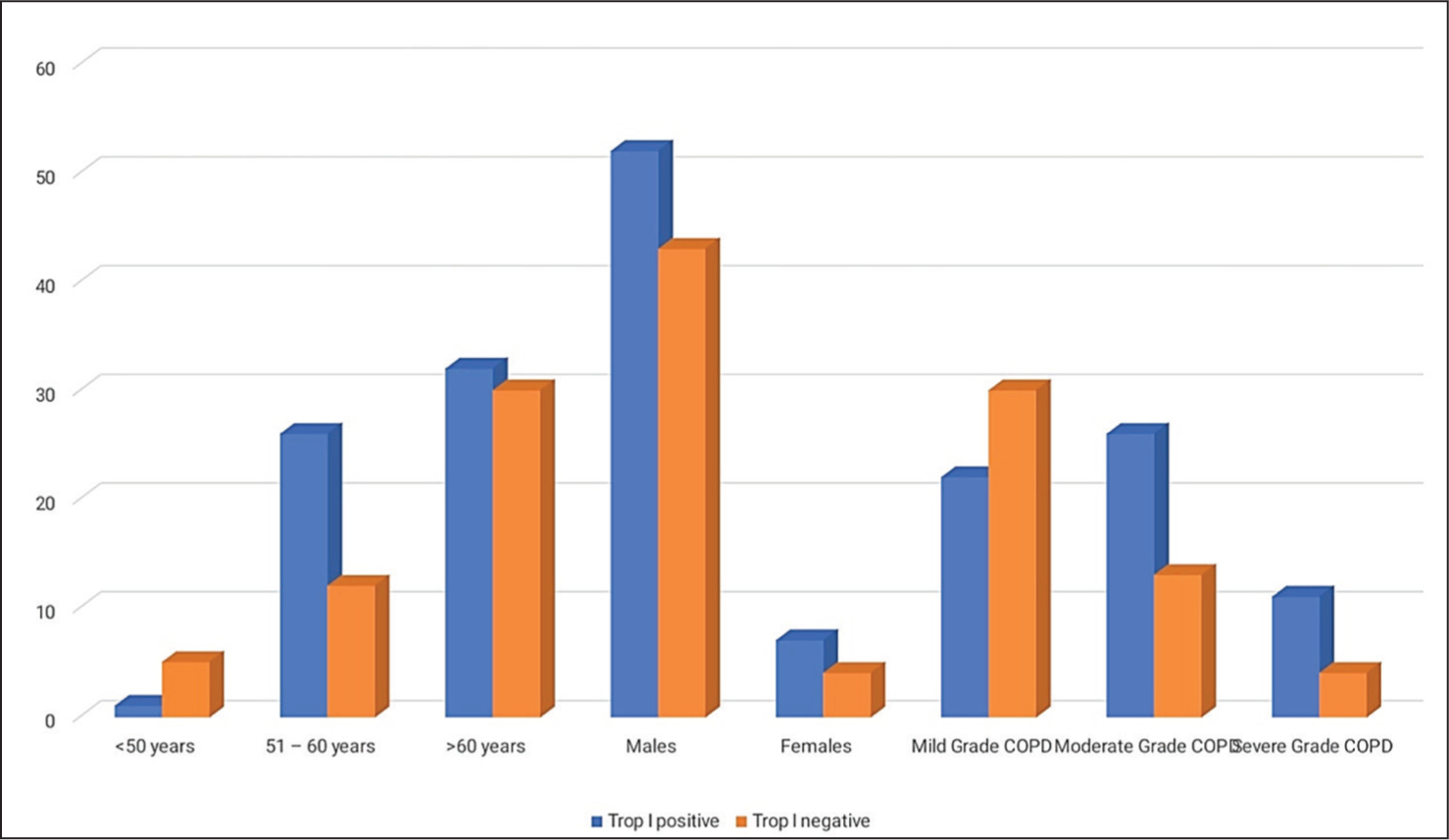
Association of cardiac troponin I with age, sex and grade of COPD
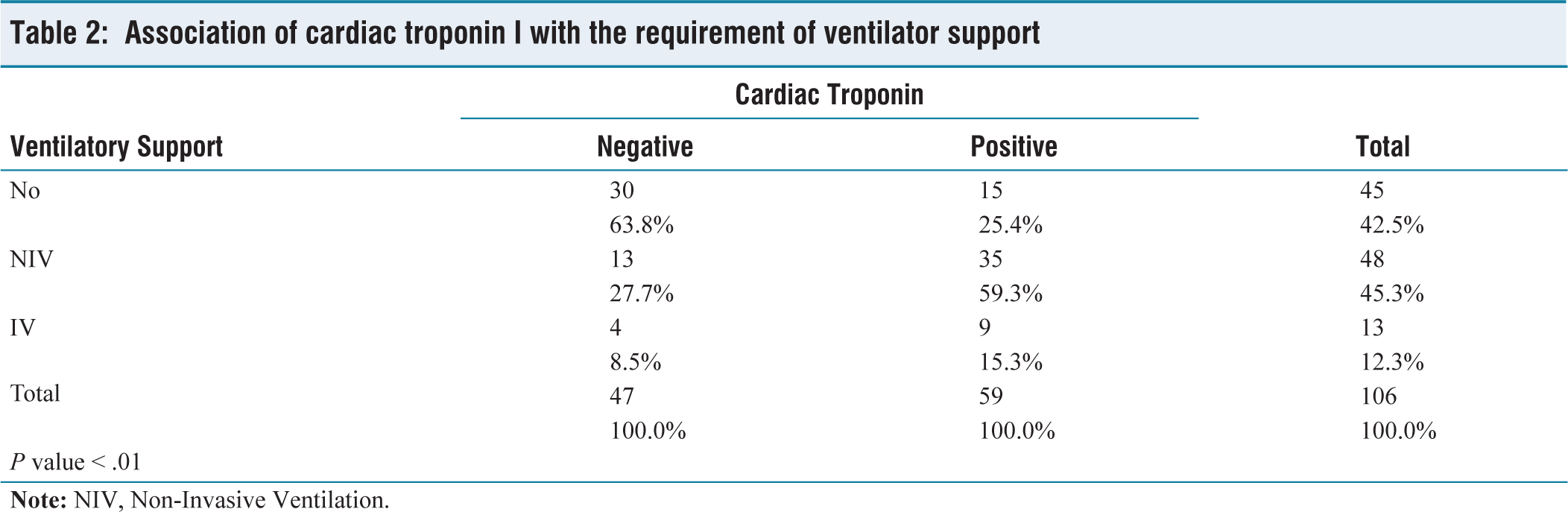
Forty five out of 106 (42.5%) patients did not require any form of ventilator support. A total of 48 patients (45.3%) were supported by non-invasive ventilation and 13 patients (12.3%) required invasive ventilator support. Ventilator support was required in 74.6% cases with positive cardiac troponin levels as compared to only 36.2% cases with negative cardiac troponin levels (P < .01) as shown in Figure 3 and Table 2.
Graph showing association of need for ventilatory support in study participants
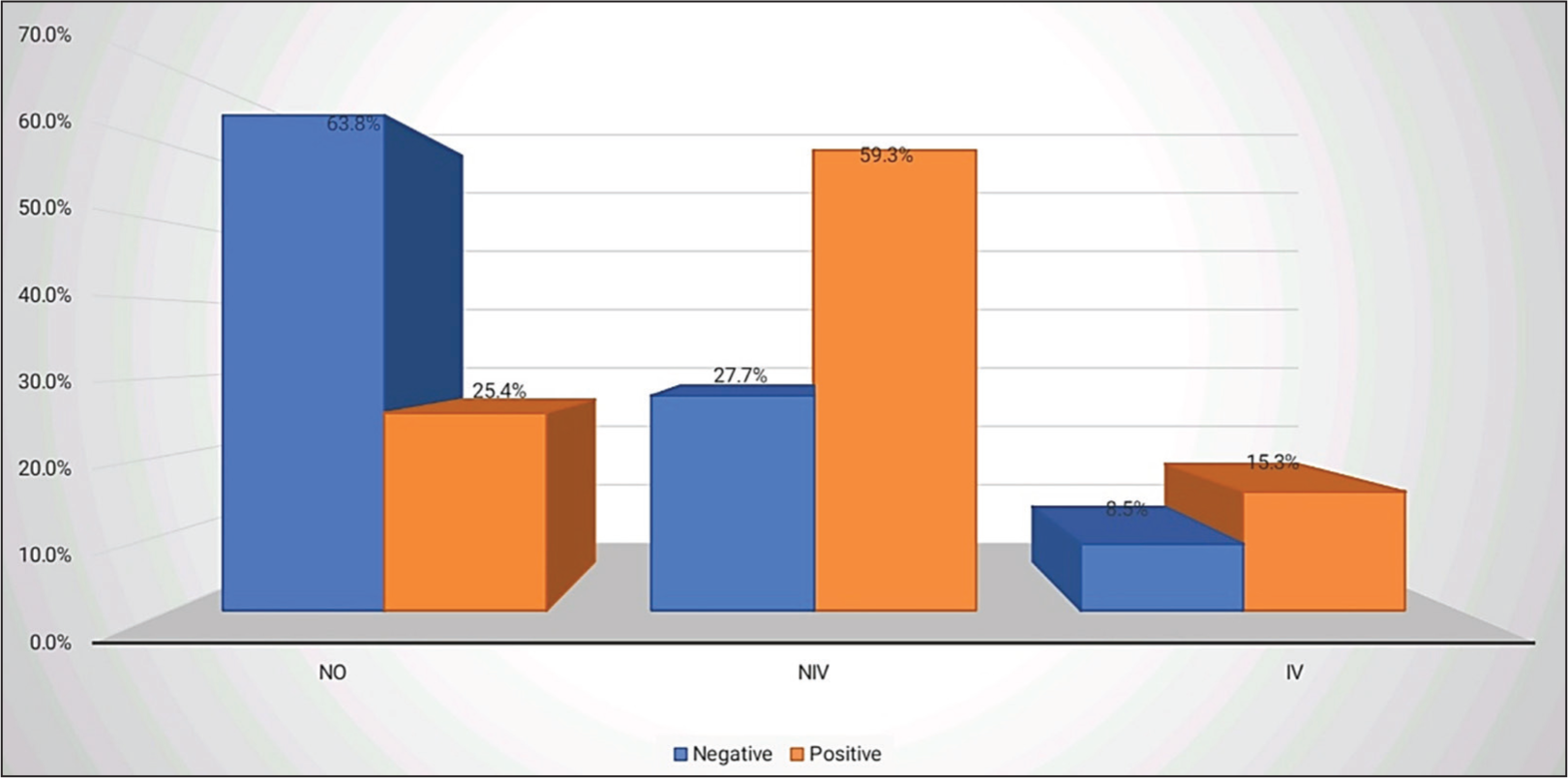
Association of cardiac troponin I with the requirement of ventilator support
Mean duration of hospitalisation was significantly more in cases with positive cardiac troponin levels as compared to cases with negative cardiac troponin levels (7.47 vs 5.75; P < .01) as shown in Figure 4 and Table 3.
Graph showing mean duration of hospitalisation of the study participants
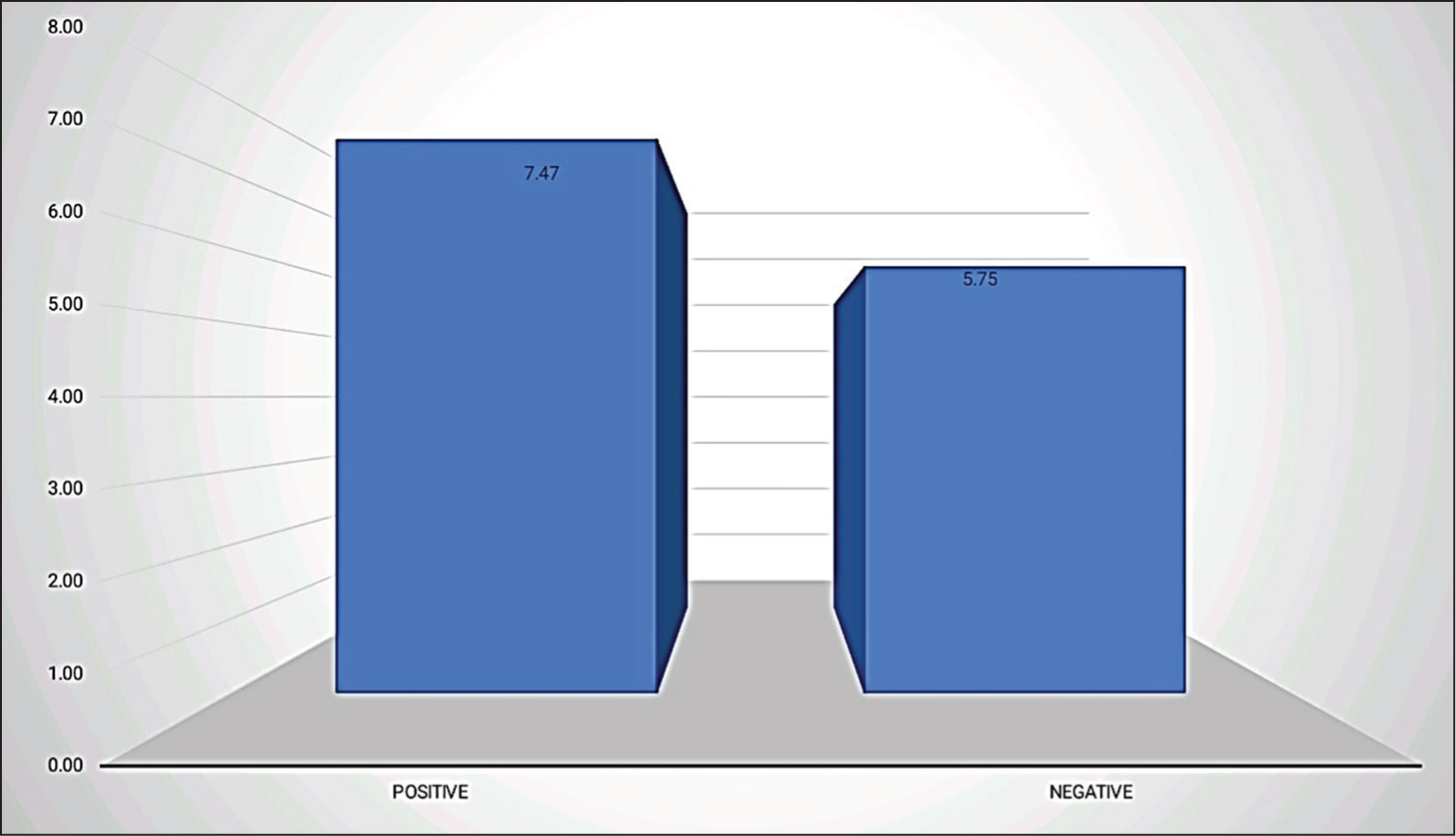
Association of cardiac troponin I with mean duration of hospitalisation

A significant majority of the patients, 102 out of 106 (96.2%), survived their treatment. Only four patients (3.8%) experienced mortality. Overall mortality rate was 3.8%, with all the four cases having raised cardiac troponin levels. Thus, mortality rate in cases with positive cardiac troponin levels was 6.8% as compared to none in cases with negative cardiac troponin levels, although the result was statistically not significant (P = .128).
Discussion
A significant association was identified between elevated cTnI levels and the severity of AECOPD (P < .05). Raised troponin levels were detected in 42.3% of mild cases, 66.6% of moderate cases and 73.3% of severe cases.
The mean duration of hospitalisation was significantly longer in patients with elevated cardiac troponin I compared to those with normal (7.47 vs. 5.75 days; P < .01). The requirement for ventilator support was also notably higher in patients with elevated cardiac troponin I (74.6%) compared to those with normal levels (36.2%) (P < .01).
Harvey et al. observed that ‘patients with elevated troponins had significantly prolonged hospital stays (5 vs. 3 days; P = .001)’.[7] Martins et al. similarly reported that ‘elevated baseline and peak cardiac troponin I levels were associated with increased need for non-invasive ventilation and extended hospitalisation’.[8] Søyseth et al. identified ‘a significant association between elevated cTn levels and increasing COPD severity (P = .039)’.[9] Youssef et al. noted that cardiac troponin I positivity was more common among patients requiring mechanical ventilation and that hospital stays were longer for cardiac troponin I-positive patients.[10] Noorain et al. also reported ‘a strong correlation between cardiac troponin I elevation and the need for ICU admission and ventilator support’. These findings reinforce the prognostic significance of elevated cardiac troponin I levels in AECOPD.[11]
Conclusion
This research reveals that patients exhibiting elevated troponin levels not only experienced a greater need for mechanical ventilation but also had longer hospital stays, affirming the implication that monitoring troponin levels could provide valuable prognostic information. Additionally, the observed mortality rate highlights the potential risk associated with increased troponin levels, linking them to adverse outcomes. These insights underscore the importance of routine cardiac biomarker screening in the clinical management of COPD exacerbations.
Limitation
The study involved a specific cohort of patients within a single hospital setting, which may limit the generalisability of the findings to broader populations or different healthcare settings.
The reliance on a single cardiac troponin I measurement may not capture the dynamic changes in cardiac injury that can occur in response to treatment or disease progression. Repeated measurements could offer a clearer picture of the relationship between COPD exacerbations and cardiac function.
Moreover, confounding factors also may impact both cardiac troponin levels and COPD severity, hence influencing the interpretation of the observed correlations.
Footnotes
Data availability statement
Data will be available on request from corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Approval for the study was obtained from the Institutional Ethics Committee (IEC), SN Medical College Agra. Letter number: SNMC/IEC/DHR/2025/51 Dated 08 March 2025.
Informed consent
Written informed consent was taken from all the patients included in the study.
Credit author statement
Nimish Gupta was involved in conceptualisation, methodology, investigation, writing-original draft, writing-review and editing and project administration.
Mridul Chaturvedi helped in conceptualisation, methodology, investigation, validation, writing-review and editing, formal analysis, and project administration and super-vision.
Nikhil Pursnani and Raj Kumar Verma contributed to methodology, writing-review and editing and formal analysis.
Gajendra Vikram Singh helped in writing-review and editing and resources.
Kirubhakar K was involved in formal analysis, writing-review and editing and resources.
Henbi Lendo and Saurabh Tripathi helped in formal analysis, writing-review and editing and project administration.
Use of artificial intelligence
N/A