
Abstract
Background:
Compressive myelopathy is a common disease. Compressive myelopathy encompasses many pathological conditions that cause damage to the spinal cord or dysfunction of the spinal cord by compression either within the spinal cord or from the outside of the cord. Many of these spinal cord diseases have the potential to be reversible if recognised early and treated appropriately. Hence, the prognosis of this condition depends on a timely and accurate diagnosis. Magnetic resonance imaging (MRI) is essential when dealing with a multifactorial disorder, such as compressive myelopathy, which is considered one of the serious neurological emergencies. We attempted to evaluate the various causes of compressive myelopathy and to characterise them.
Materials and Methods:
This is a retrospective study conducted at a tertiary care hospital in Chennai from January 2024 to June 2024. We retrospectively examined a total of 48 cases from our department with the reports of compressive myelopathy on MRI spine studies.
Results:
We found that degenerative myelopathy (37.5%) was found to be the most common cause, followed by trauma (22.9%) and infection (18.8%), malignancy, including metastasis (16.7%), and Hirayama(4.2%). The cervical spine compression (54.2%) and the extradural compartment (89.6%) were more frequently involved.
Conclusion:
The study recommends MRI for individuals with suspected compressive myelopathy, as it accurately identifies the underlying cause and related characteristics. Providing precise information about the patient’s long-term prognosis is beneficial.
Keywords
Introduction
Diseases causing cord compression can be classified into acute causes, such as traumatic causes, infection with abscess formation and chronic conditions like degenerative changes of the spine, tumoural compression of the cord and Hirayama.[1] Magnetic resonance imaging (MRI) is the most accurate way to assess soft tissue damage, particularly in the spinal cord and ligaments. MRI can reveal fractured/subluxated vertebral bodies, causing stenosis of the spinal canal, and is also useful in assessing the posterior ligamentous injury. The signal abnormality inside the cord can be recognised and aid in determining the severity of trauma. MRI is an effective tool for imaging tumours affecting the spinal canal and spinal cord in cases of suspected cord compression caused by neoplasms. Early detection and treatment are crucial for reversing many spinal cord illnesses. Hence, the prognosis of this condition depends on a timely and accurate diagnosis.[2] The purpose of MRI is to identify compressive from non-compressive myelopathy.
Materials and Methods
This is a retrospective study conducted in a tertiary care hospital in Chennai over six months, from January 2024 to June 2024. We have a total of 48 cases retrospectively searched in our department for reports of compressive myelopathy in MRI spine studies. The patients with clinical suspicious and imaging findings of compressive myelopathy at all age groups were included in this study. Patients with non-compressive causes of myelopathy like demyelination, ischaemia and with motion artefacts, metallic implants that rendered MRI technically infeasible were excluded from our study. The Institutional Ethics Committee accepted the study (Approval Number: AMH-C-S-063/07-24). Canal stenosis was classified according to the T2-weighted sagittal images into the following grades: grade 0, absence of canal stenosis; grade 1, subarachnoid space obliteration exceeding 50%; grade 2, spinal cord deformity; and grade 3, spinal cord signal change.[3] MR classification system of intramedullary T2 hyperintensity signal intensity was divided into four categories, type 0 = normal signal intensity of spinal cord without any intramedullary T2 hyperintensity, type 1 = diffuse pattern of intramedullary T2 hyperintensity occupying more than two-thirds of axial dimension of spinal cord with an obscure and faint border, and types 2 and 3 = focal patterns of intramedullary T2 hyperintensity occupying less than two-thirds of axial dimension of spinal cord. Type 2 indicates focal intramedullary T2 hyperintensity with an obscure and faint border, whereas type 3 has a well-defined and distinct margin.[4]
Study Protocol
All patients fulfilling the inclusion criteria were subjected to the study. MRI of the spine was performed on a 3.0-T (PHILIPS, INGENIA) using sixteen phased-array coils for the spine. The sequences were axial, sagittal section of T1- and T2-weighted scans, coronal section of short tau inversion recovery (STIR), and depending on clinical details, sagittal section of diffusion-weighted imaging (DWI) and apparent diffusion coefficient (ADC) will be done.
Statistical Analysis
Descriptive statistics were presented with frequency (percentage). Chi-square/Fisher’s exact test was used to determine the association between two independent categorical factors. P value < .05 is considered as statistical significance. All the statistical analysis was done by using SPSS (IBM, 28.0)
Results
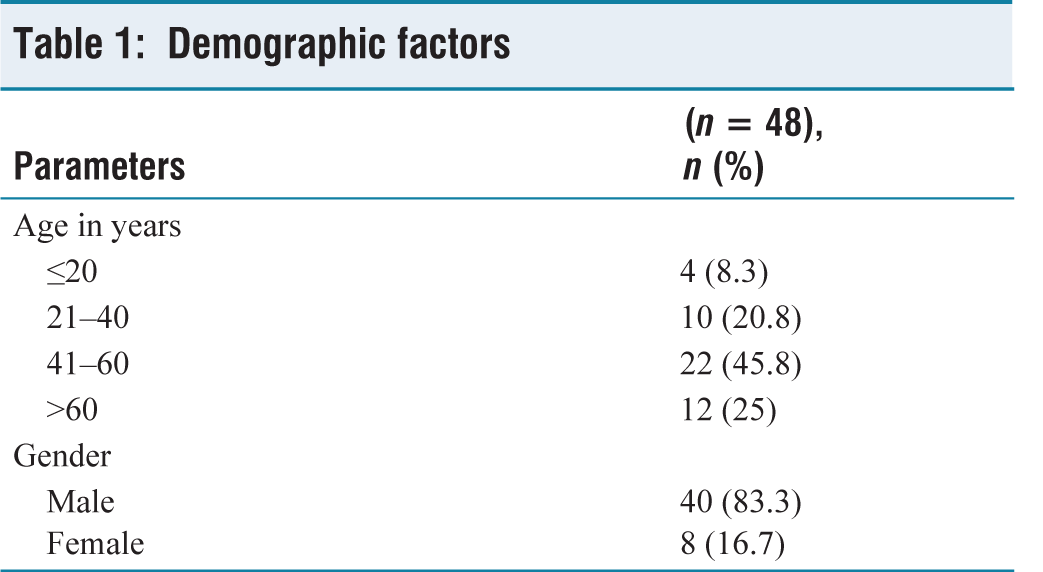
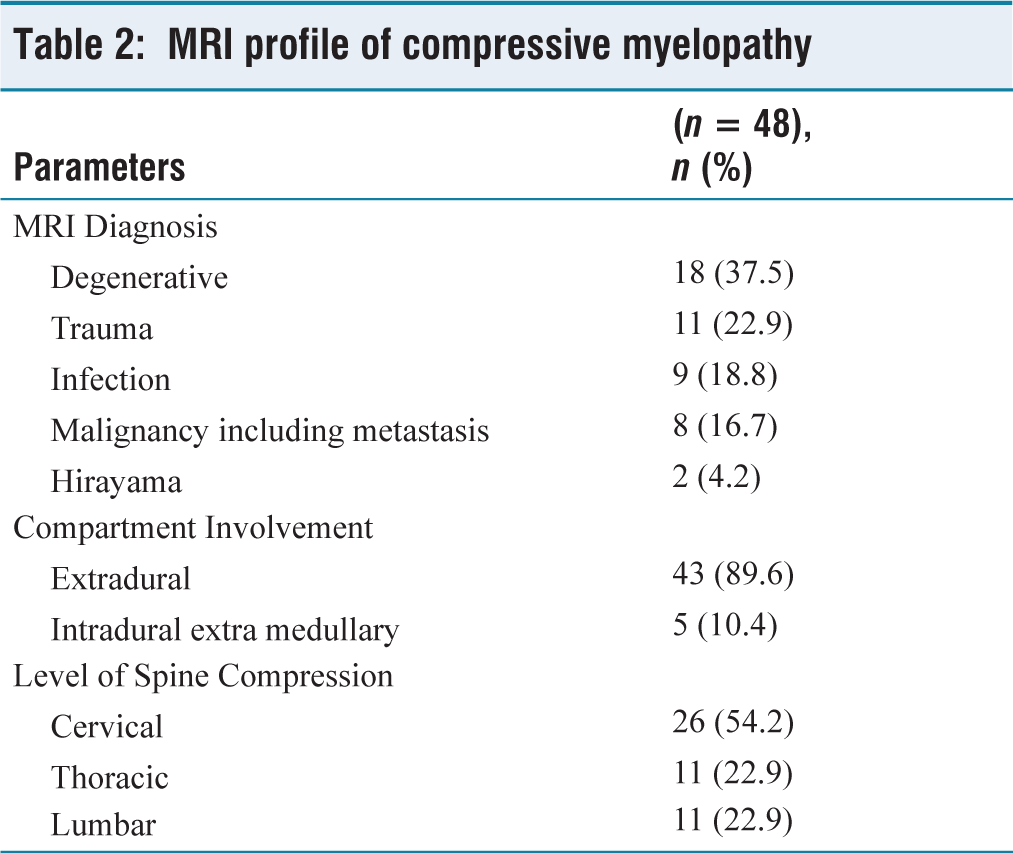
The majority of cases were seen between the age group of 41 and 60 years (45.8%) [Table 1], with a male predominance of 40 patients (83.3%) [Table 1]. The most common cause of compressive myelopathy was degenerative disease seen in 18 patients (37.5%) followed by trauma seen in 11 patients (22.9%), infection with or without abscess formation seen in 9 patients (18.8%), malignancy including metastasis seen in 8 patients (16.7%) and Hirayama seen in 2 patients (4.2%) [Table 2].
Demographic factors
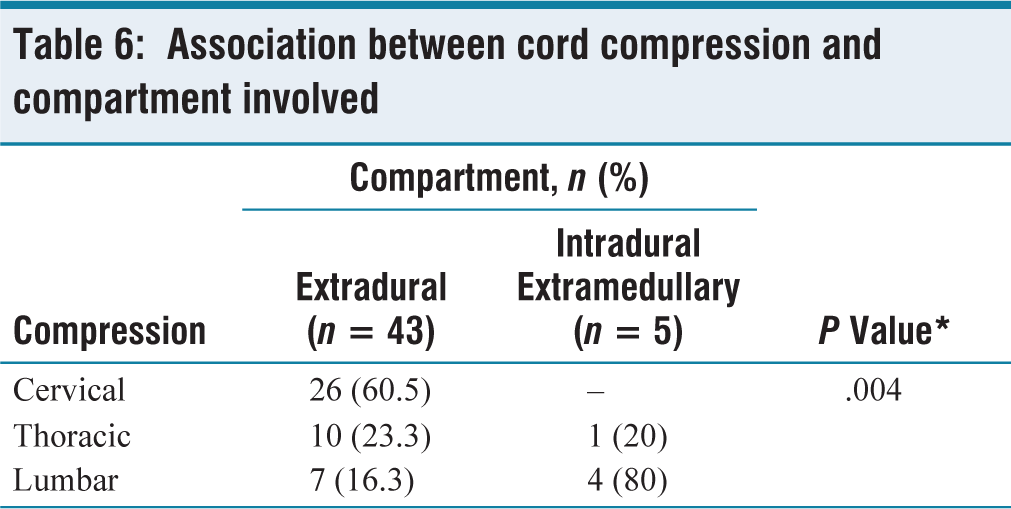
Extradural compression is most commonly seen in 43 patients (89.6%). Intradural extramedullary compression was seen in 5 patients (10.4%) [Table 2]. The cervical spine is most commonly involved in 26 patients (54.2%), followed by the thoracic spine seen in 11 patients (22.9%) and lumbar spine seen in 11 patients (22.9%) involvement [Table 2]. The association between the extradural and intradural extramedullary compartment lesion with the spinal cord compression at cervical, thoracic and lumbar regions was found to be significant with a P value of .004 [Table 6].
MRI profile of compressive myelopathy
Degenerative
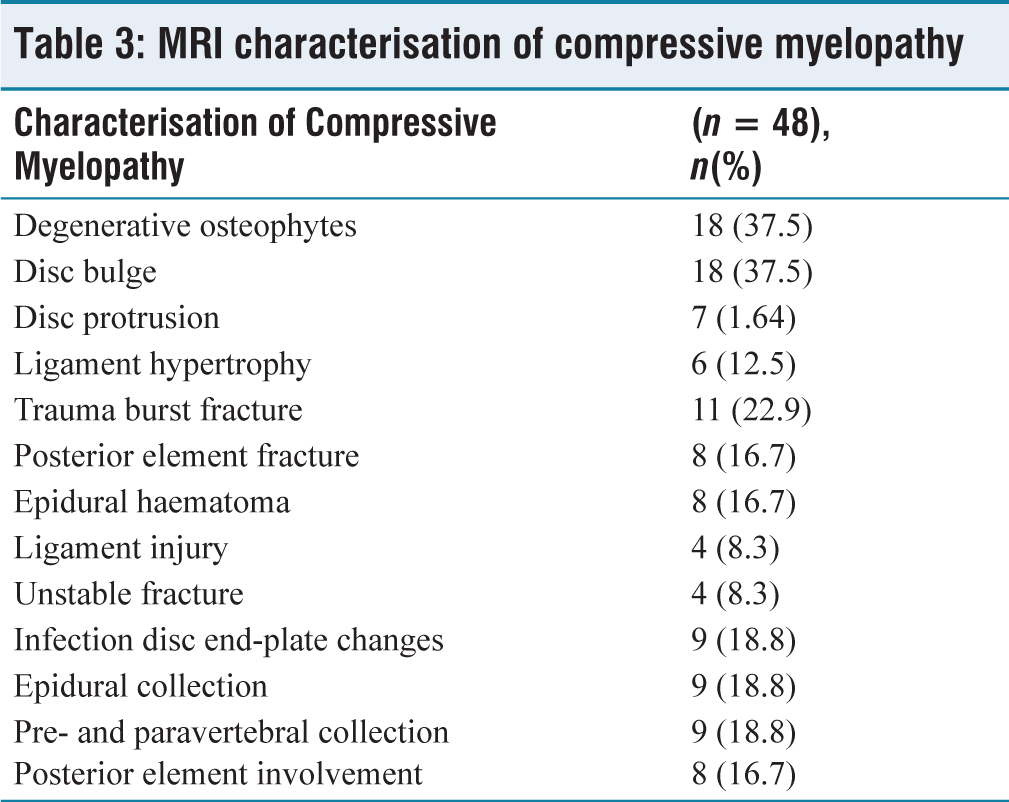
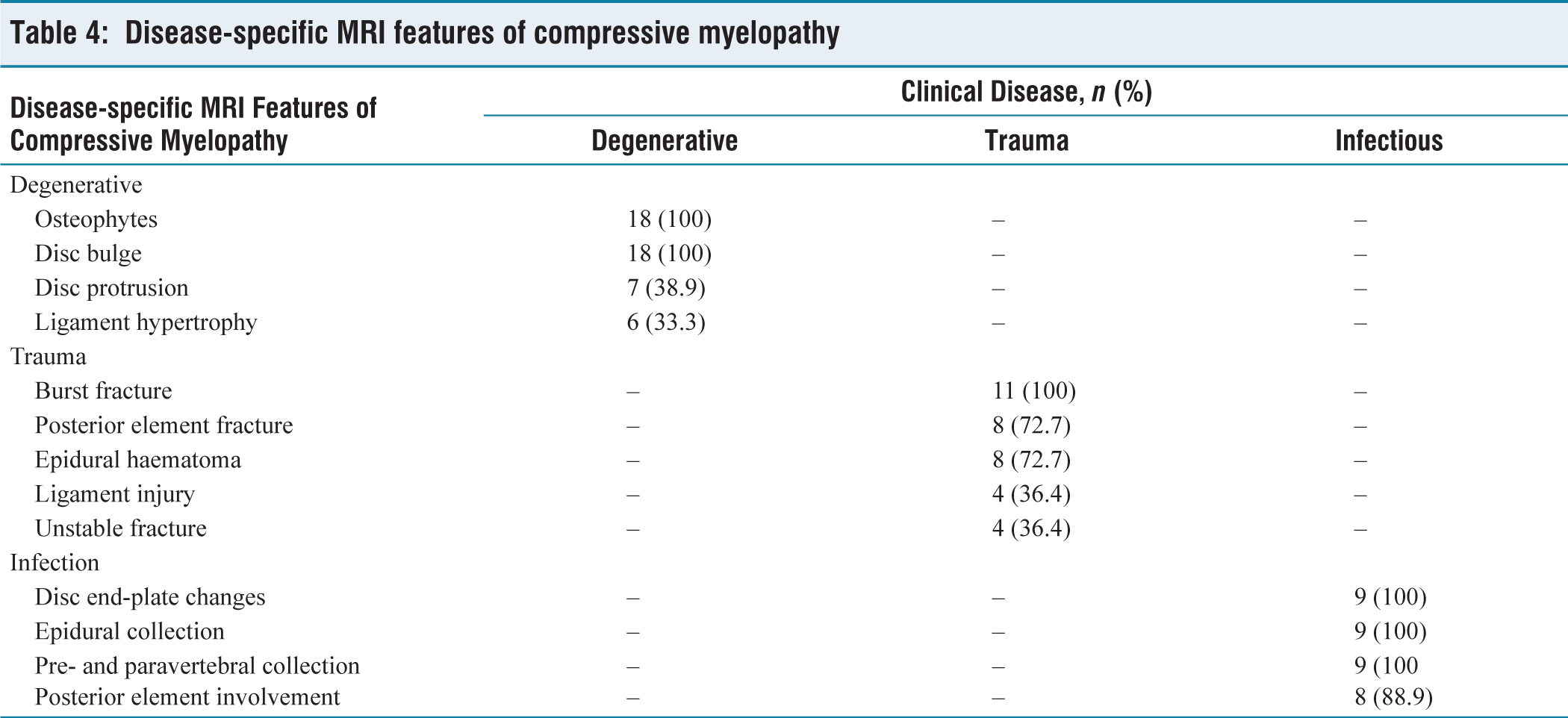
Causes of compressive myelopathy characterised by osteophytes and disc bulges were seen in 18 patients (100%), followed by disc protrusion seen in 7 patients (38.9%), and thickening of the posterior longitudinal ligament in 6 patients (33.3%) [Tables 3 and 4]. All of them show grade 3 canal stenosis, 13 patients showed type 1 T2 signal intensity and 3 individuals showed type 2 T2 signal intensity and rest of the remaining 2 show type 3 T2 signal intensity within the cord.
MRI characterisation of compressive myelopathy
Disease-specific MRI features of compressive myelopathy
Trauma
Causes of compressive myelopathy characterised by burst fractures seen in 11 patients (100%), posterior element fracture and epidural haematoma were seen in 8 patients (72.7%), followed by ligament injury and unstable fractures in 4 patients (36.4%) [Tables 3 and 4]. All of them show grade 3 canal stenosis, 8 patients showed type 1 T2 signal intensity and one individual shows type 2 T2 signal intensity and the rest of the 2 showed type 3 T2 signal intensity within the cord.
Infection
Causes of compressive myelopathy disc end-plate changes, epidural, pre- and paravertebral collection were seen in 9 patients (100%), and posterior elements involvement was seen in 8 patients (88.9%) [Tables 3 and 4]. All of them show grade 3 canal stenosis and type 1 T2 signal intensity changes within the cord.
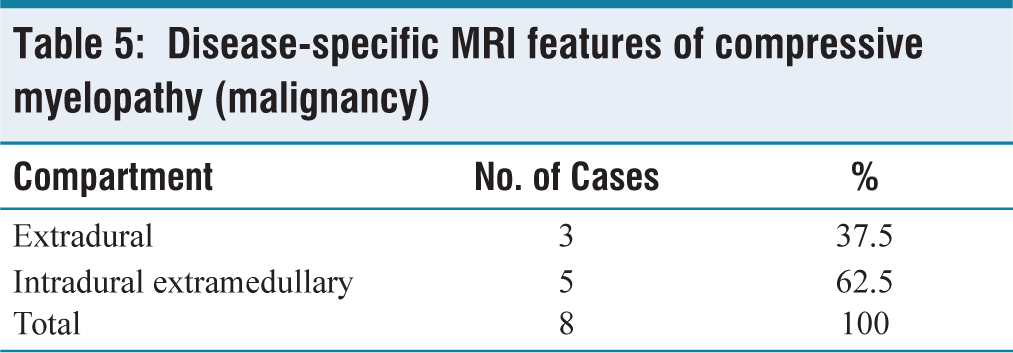
Malignancy
Both primary and metastasis total of 8 cases. Five patients (62.5%) had intradural extramedullary components, and three patients (37.5%) had extradural components [Table 5]. All of them show grade 3 canal stenosis and type 1 T2 signal intensity changes within the cord.
Disease-specific MRI features of compressive myelopathy (malignancy)
The association between the extradural and intradural extramedullary compartment lesion with the spinal cord compression at cervical, thoracic and lumbar regions was found to be significant with a P value of .004 [Table 6]. In degenerative myelopathy and traumatic spinal injury, the cervical spine is most commonly involved. The most common region involved in infective spondylitis is the lumbar region
Association between cord compression and compartment involved
Discussion

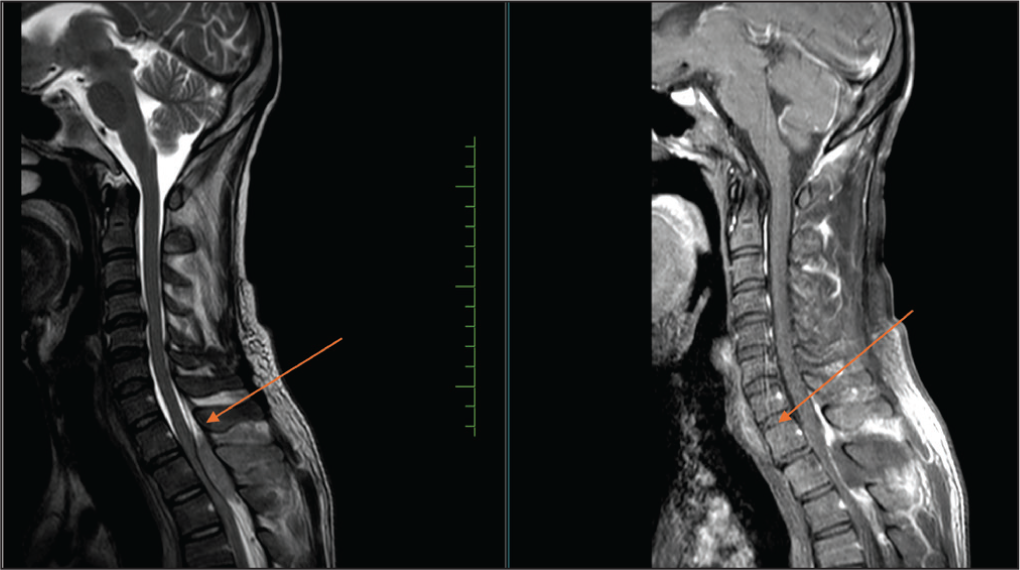
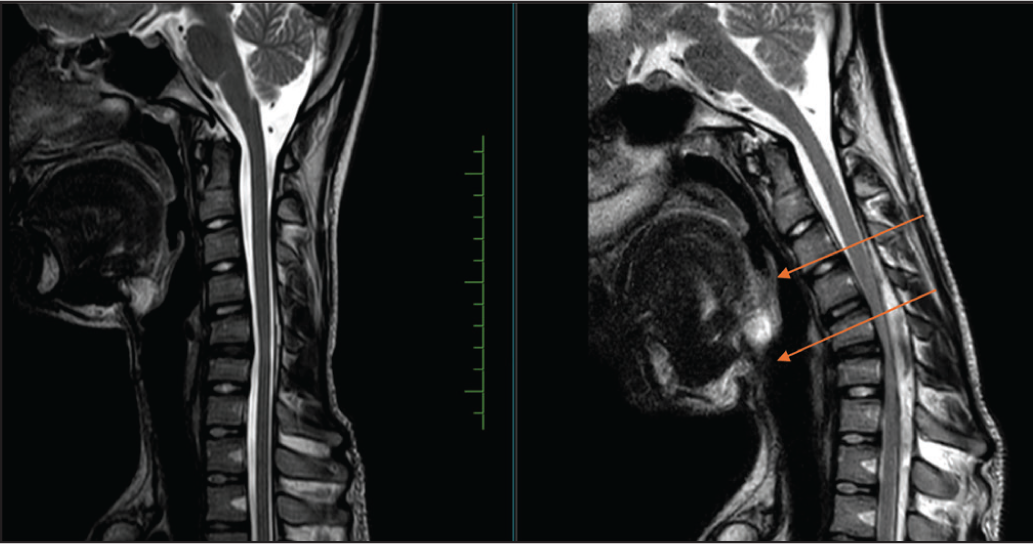
Hirayama T2 sagittal neutral and flexion sequence of MRI cervicodorsal spine shows anterior displacement of the posterior dura mater at the C4 to C7 level, compressing the spinal cord against the vertebral column. Focal cord atrophy changes are seen at the C5-C6 level.
Conclusion
MRI is the definitive modality for examining soft tissues of the spine and spinal cord abnormalities, including cord oedema/contusion and intervertebral discs and ligaments. Due to its high sensitivity, MRI is the preferred imaging method for detecting and characterising spinal tumours and infections. Finally, MRI is a highly definite, accurate, cost-effective, non-invasive, radiation-free method for evaluating compressive myelopathy.
Footnotes
Acknowledgements
We are thankful to the Research Department—Shivashankari, Research Assistant and Logesh—Biostatistician, Apollo Hospital, Chennai and to the Department of Radiology for providing access to imaging data and technical support. We thank the hospital administration for their institutional backing and infrastructure. We also acknowledge the contributions of our colleagues in the neurology and neurosurgery departments for their clinical insights. Lastly, we express our appreciation to all patients involved in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval was obtained from the Institutional Ethics Committee of Apollo Hospitals, Chennai. Approval Number: AMH-C-S-063/07-24.
Informed consent
Informed consent has been obtained from all the patients who met the eligibility criteria.
Credit author statement
MAL participated in data acquisition, literature search, investigations, data analysis and manuscript preparation.
AB participated in conceptualisation, investigation, supervision, data analysis and manuscript editing.
Both authors have reviewed and approved the manuscript.
Patient consent
Not obtained.
Data availability
Data presenting the study’s findings are available from the corresponding author.
Use of artificial intelligence
The authors affirm that no generative artificial intelligence or AI-assisted tools were used in the writing, data analysis, or image generation for this manuscript.