
Abstract
Background and Aims:
Non-resolving pneumonia (NRP) refers to pneumonia that resolves slowly or incompletely despite appropriate treatment in populations with delayed or disproportionate initiation of therapy, NRP can lead to drug resistance, increased morbidity and ultimately mortality. While the majority of patients respond well to initial antimicrobial therapy, a subset exhibits poor response, resulting in NRP or death. The objective of this study was to identify the underlying causes of NRP by utilising fiberoptic bronchoscopy (FOB) as a diagnostic method.
Materials and Methods:
This prospective study was conducted in the Department of Pulmonary Medicine at Andhra Medical College, Visakhapatnam and included 50 patients diagnosed with NRP. All patients underwent FOB, during which clinical, radiological and bronchoscopic findings were recorded. Diagnostic techniques such as bronchoalveolar lavage (BAL), brush cytology and transbronchial lung biopsy (TBLB) were employed.
Results:
A definitive diagnosis was achieved in 94% (n = 47) of the patients, with most being males over the age of 50. The right lower lobe was most commonly affected. Gross bronchoscopic examination revealed inflamed mucosa with mucopurulent discharge in a large number of cases. Infectious causes accounted for 50% (n-25) of cases, with Gram-negative bacterial infections being most common (32%), followed by tuberculosis (14%) and fungal infections such as mucormycosis (4%). Pseudomonas was the predominant bacterial pathogen, followed by Klebsiella. Malignancies constituted 28% (n = 14) of cases, with adenocarcinoma being the predominant histological subtype, followed by squamous cell carcinoma. Malignancy was identified in 14%of cases by BAL cytology and in 14% by brush cytology. TBLB was able to diagnose the aetiology in 8,461% (22 out of 28) of the cases where it was performed.
Conclusion:
Fibreoptic bronchoscopy is a safe and valuable diagnostic tool in the evaluation of NRP, offering high diagnostic yield, especially in detecting infections and malignancies.
Keywords
Introduction
Pneumonia is characterised as an inflammatory condition of the lung parenchyma caused by infectious organisms and remains one of the most prevalent clinical conditions. Despite significant advancements in diagnostic and therapeutic strategies, the mortality rate associated with pneumonia continues to range between 5% and 15%.[1,2] In a substantial portion of the population, delayed or inappropriate treatment contributes to the development of drug resistance, increased morbidity and ultimately, mortality. The persistence or incomplete resolution of pneumonia can be attributed to multiple factors, including the underlying aetiology, host immune response, diagnostic inaccuracies and the emergence of complications following the initial infection. Additionally, various non-infectious conditions may clinically and radiologically mimic pneumonia. Notably, nearly one-fifth of non-resolving pneumonia (NRP) cases arise from non-infectious etiologies. Nonetheless, there remains a scarcity of research dedicated exclusively to NRP.
Non-resolving Pneumonia (NRP)
NRP, characterised by a delayed or incomplete resolution of pneumonia despite appropriate treatment, is a common clinical problem, accounting for about 15% of inpatient pulmonary referrals and 8% of cases undergoing bronchoscopy.
Definition Challenges
Universally accepted definition of NRP remains elusive, with existing literature offering varied criteria.
Lung India, 2013: Non-resolving pneumonia is defined by persistent clinical symptoms and radiographic findings that fail to improve by at least 50% within 2 weeks or completely within 4 weeks, even after at least 10 days of antibiotic treatment and two negative acid-fast bacilli (AFB) smear results.[3]
BMJ, 2016: Slowly resolving pneumonia is characterised by the persistence of radiographic infiltrates for over 4 weeks in clinically improving patients, with less than 50% resolution during this period.[4]
According to the 2007 IDSA/ATS guidelines, non-resolving or slowly resolving pneumonia is characterised by pulmonary infiltrates that continue for over 30 days following the onset of pneumonia symptoms.
Given the limited literature specifically addressing NRP, especially in cases where chest CT findings are inconclusive, this study seeks to assess the usefulness of bronchoscopy in determining the underlying cause in these patients.
Materials and Methods
Study Design
This was a prospective observational study.
Study Setting
The study was carried out in the Department of Pulmonary Medicine at Andhra Medical College, Visakhapatnam.
Study Duration
Participants meeting the inclusion criteria were enrolled and observed between August 2023 and June 2024.
Study Population
The study enrolled patients aged 12 years and above with NRP who were admitted to the Department of Pulmonary Medicine, Andhra Medical College, Visakhapatnam.
Inclusion Criteria
Patients who met the criteria for NRP as outlined in Lung India.[3]
Patients presenting with a clinical profile suggestive of pneumonia whose chest radiograph failed to show ≥50% resolution within 2 weeks or no significant radiological improvement after approximately 4 weeks and who demonstrated no radiographic response following 10 days of antibiotic therapy.
Exclusion Criteria
Patients unwilling to provide consent.
Patients with a confirmed diagnosis of neoplastic disease.
Patients who were smear-positive for tuberculosis or had active TB.
Patients with a recent history of myocardial infarction.
Patients reactive for HIV.
Patients with hemodynamic instability, poor general condition or those who were uncooperative.
Methodology
Following approval from the institutional ethics committee, a total of 50 patients who met the study’s inclusion criteria were enrolled. Based on the definition of NRP from Lung India, participants were enrolled.
Demographic data, including name, age, sex and occupation, were collected.
A comprehensive clinical history was taken, covering the duration of illness, any previous use of anti-tubercular therapy and comorbid conditions such as diabetes mellitus, hypertension, coronary artery disease, chronic kidney disease (CKD) and chronic liver disease.
Details regarding smoking habits and alcohol intake were also noted.
Baseline laboratory investigations included complete blood picture, random blood sugar, renal function tests, liver function tests, prothrombin time with INR, activated partial thromboplastin time and serum electrolytes.
All patients underwent screening for HIV, hepatitis B and hepatitis C before the procedure.
Sputum analysis was carried out for AFB, Gram staining and culture, fungal staining and culture, along with cytological examination for malignant cells.
Imaging studies such as chest X-ray and CT chest were advised for all participants.
Additional diagnostic modalities, including ultrasonography of the chest, cardiac evaluation and relevant serological tests, were carried out when indicated.
Before undergoing the procedure, all patients received empirical antimicrobial therapy for approximately 10 days in accordance with standard guidelines. The purpose, advantages and possible complications of bronchoscopy were explained to them. Consent was obtained in the patients’ native language, both orally and in written form. Baseline vital parameters were documented before initiating the procedure.
During the study, an Olympus broncho videoscope BF Type PI-150 was utilised. The system has a 120° field of view, depth of field ranging from 3 mm to 100 mm, outer diameter of 5.3 mm, angulation capacity of 180°, total length of 870 mm with a working length of 600 mm and an inner diameter of 2.0 mm. It is also fully compatible with electrocautery and Nd: YAG or 810 diode laser applications.
For transbronchial lung biopsy (TBLB), Olympus FB-231 D standard oval biopsy forceps were used, equipped with a 5 mm cup opening and a working length of 115 cm. Cytological specimens were collected using a bronchial brush (Olympus BC-202D-3010) with a protective sheath; the brush measured 10 mm in length, had an outer diameter of 3 mm and bristles with a diameter of 0.064 mm.
The procedure involved sequential steps: Examination of the upper airways, evaluation of vocal cord function, inspection of the trachea and systematic assessment of the bronchial tree, followed by bronchoscopic sampling techniques. Patient vitals were continuously monitored and all procedures were conducted under standard protocols with appropriate safety precautions.
The collected samples were immediately sent to the laboratory. Bronchoalveolar lavage (BAL) fluid was centrifuged at 1500 rpm for 5 minutes and smears were prepared for cytology, total and differential cell counts using H and E staining. BAL specimens were also tested for AFB, GeneXpert, Gram stain and culture, as well as fungal stain and culture. Cytological evaluation was carried out on bronchial brushing samples, while TBLB specimens were preserved in formalin and forwarded for histopathological examination.
Following the procedure, patients were monitored for at least 1 hour to detect any complications such as severe haemoptysis or hypoxia. A chest X-ray was performed afterwards to rule out procedure-related complications, including pneumothorax.
Results
The study included 50 patients (N = 50). All were admitted via the emergency department, remained clinically stable and did not require either mechanical ventilation or tracheostomy. Among them, 74% (n = 37) were male and 26% (n = 13) were female.
The age distribution was as follows: 6% (n = 3) were 20–30 years, 16% (n = 8) were 31–40 years, 18% (n = 9) were 41–50 years, 30% (n = 15) were 51–60 years and 24% (n = 12) were 61–70 years. The majority of patients belonged to the 41–70 years age group.
Since the study was carried out in a tertiary care hospital, all patients were referred from peripheral centres. The initial sputum culture and sensitivity results for the study group were non-conclusive.
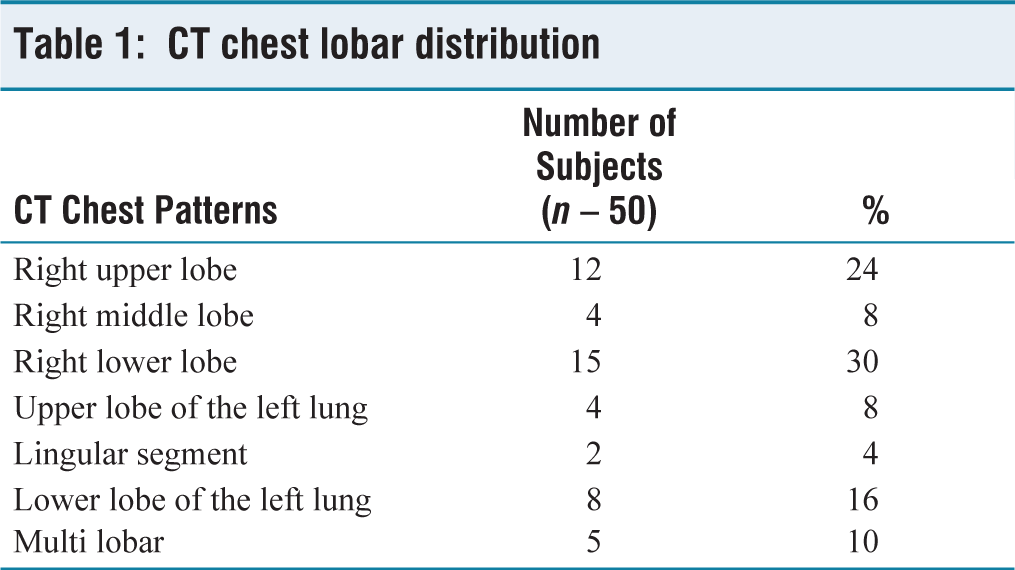
X-ray and CT chest involvement: CT chest of all subjects had presented with random presentations; results are revised in the table below [Table 1].
CT chest lobar distribution
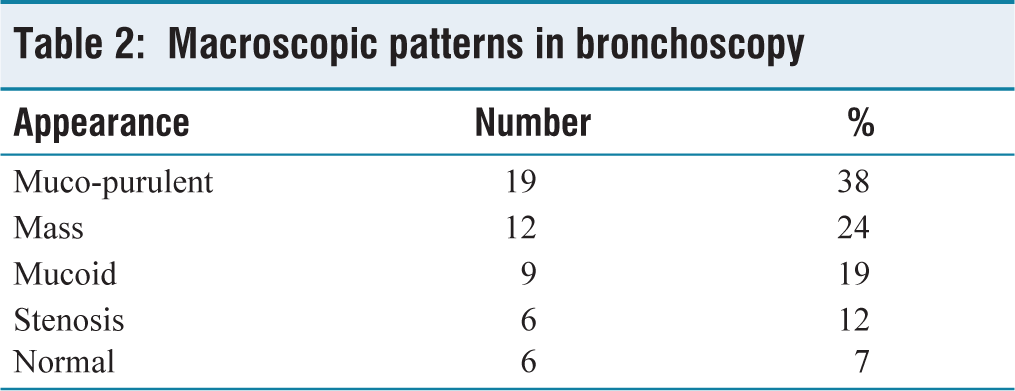
Bronchoscopy Macroscopic Observations
The changes observed during bronchoscopy are revised in the table below [Table 2].
Macroscopic patterns in bronchoscopy
Diagnostic Accuracy
Altogether, the accuracy of fiberoptic bronchoscopy (FOB) in my study was 94% (n47). In 6% no diagnosis was made.
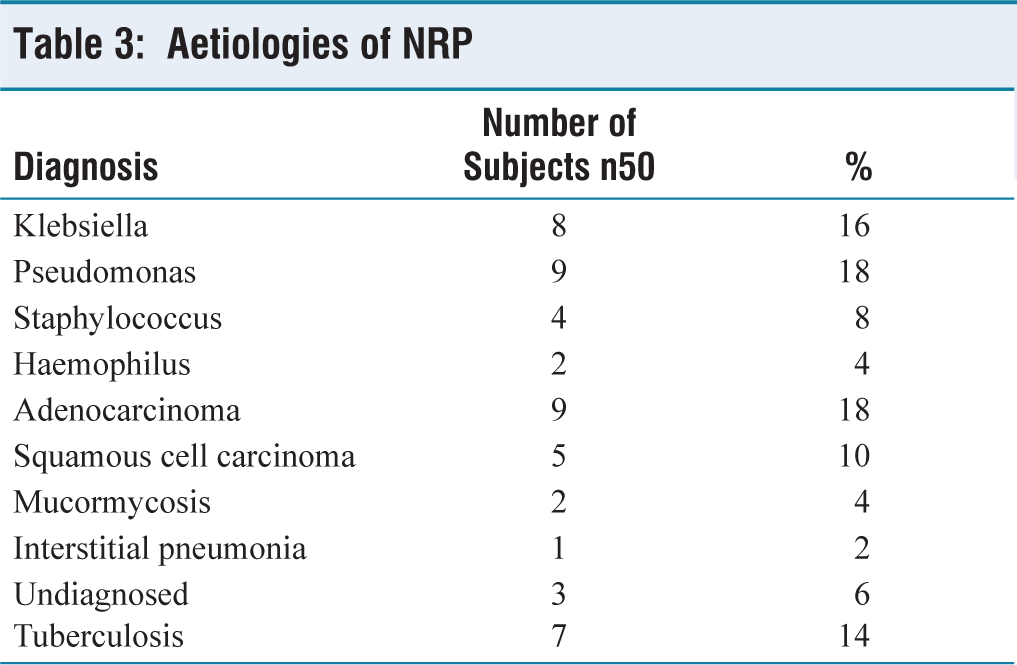
Aetiology in my study: Most of the patients were diagnosed with an infective aetiology, followed by a neoplastic aetiology. Infections were the aetiology in 50% (n25), malignancy was diagnosed in 28% (n14), tuberculosis was diagnosed in 14% (n7), interstitial pneumonias were diagnosed in 2% and lastly, indeterminate aetiology in 6%. The different aetiologies are elaborated in the table below [Table 3].
Aetiologies of NRP
BAL Cytology
In cytology, malignancy was identified in 14% (n7) and the remaining 86% (n43) showed inflammatory changes.
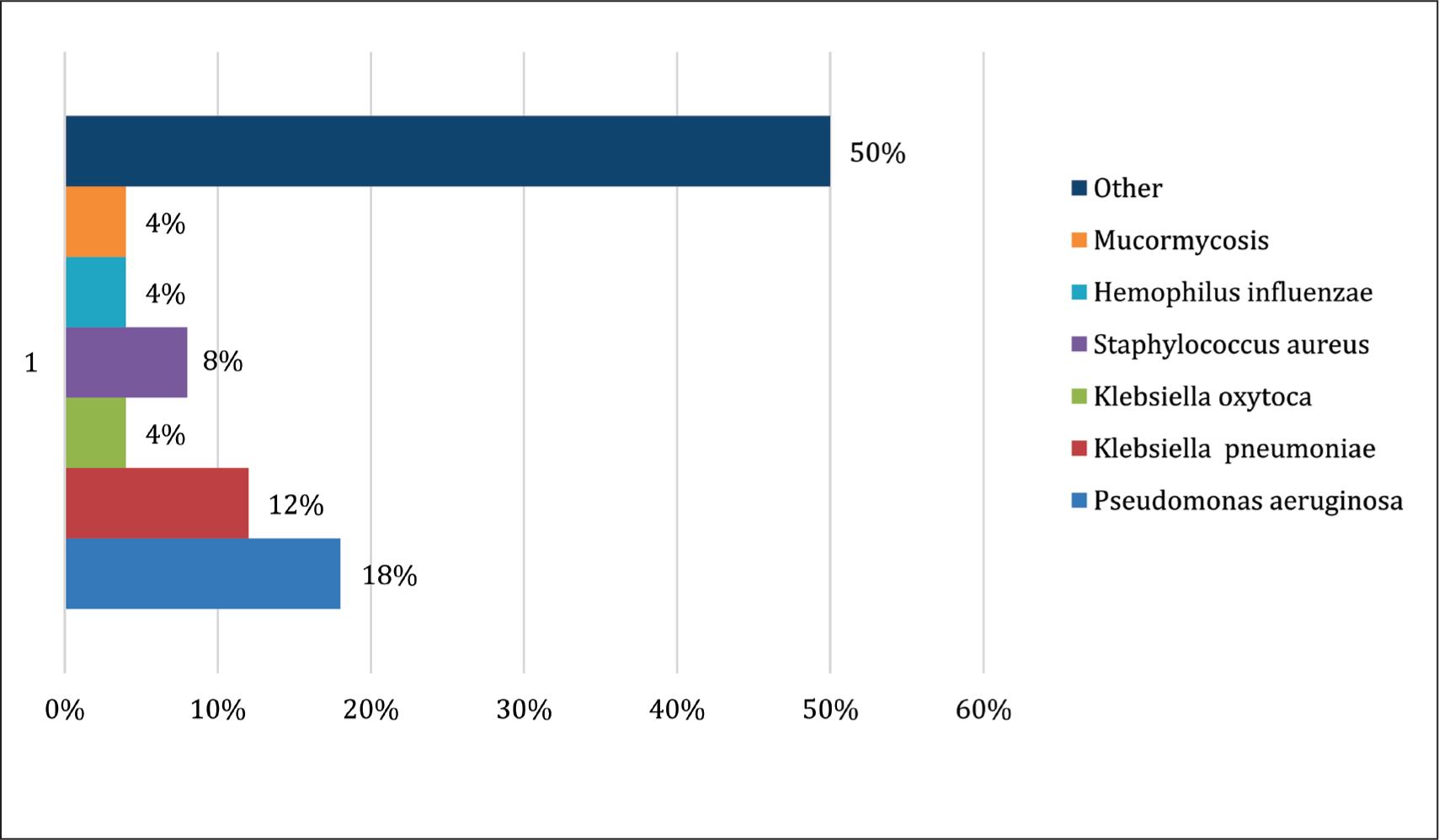
Microbiological
Out of 50 patients, 50% were infected. Out of all, the predominant bacteria isolated in culture were Pseudomonas aeruginosa, followed by Klebsiella pneumonia. The percentage and different organisms isolated in the study are elaborated in the figure below [Figure 1].
BAL culture patterns
Mycobacterium tuberculosis (MTB) was diagnosed in 14% (n7), Out of them, 3 patients were positive for AFB smear and in the remaining 4, MTB was detected in BAL using a cartridge-based nucleic acid amplification test (CBNAAT).
Transbronchial Lung Biopsy (TBLB)
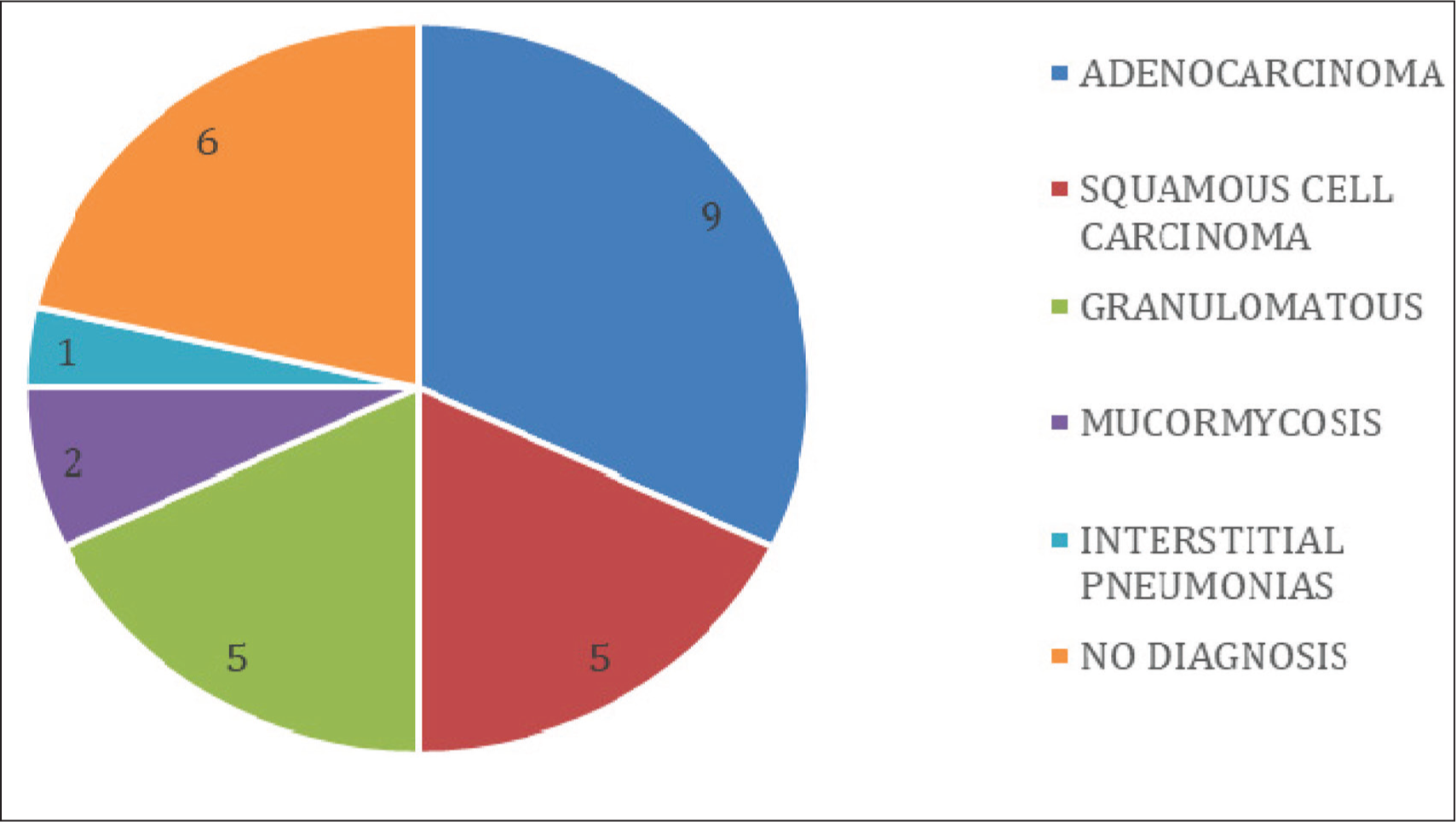
Among 50 subjects, TBLB has been performed in 28 patients and the results have been elaborated in the figure below [Figure 2].
TBLB patterns
Comorbidities
Among the 50 patients in the study, 66% (n = 33) were smokers and 36% were diabetic. Diabetes showed a stronger association with infectious etiologies. Additional comorbid conditions included CKD in 1 patient and chronic liver disease in 3 patients.
Complications
Post-bronchoscopy, a chest X-ray was performed for all patients and none developed pneumothorax. Only minor complications were observed, such as transient fever, mild bleeding and temporary desaturation during the procedure. No major adverse events, including massive haemoptysis, were encountered.
Discussion
This study was conducted on 50 patients diagnosed with NRP, all of whom underwent bronchoscopy. A definitive aetiology was established in 47 cases, while in 3 patients, image-guided FNAC was performed. The obtained tissue samples were examined using CBNAAT, Gram stain and culture, fungal culture and NTM testing; however, no conclusive diagnosis could be made in these cases. Repeat image-guided FNAC also failed to provide definitive results. Histopathology demonstrated only non-specific inflammation. These patients were subsequently referred to a higher centre with facilities for EBUS and cryobiopsy for further evaluation. On follow-up, 1 case was diagnosed as adenocarcinoma, whereas the remaining 2 cases continued to remain inconclusive and were advised further follow-up.
Comparison between initial pneumonia pathogens and organisms isolated during the course of NRP could not be made, as most of the patients were referrals from peripheral centres, where microbiological data from the initial stage of illness were not available at the time of presentation to our tertiary care hospital.
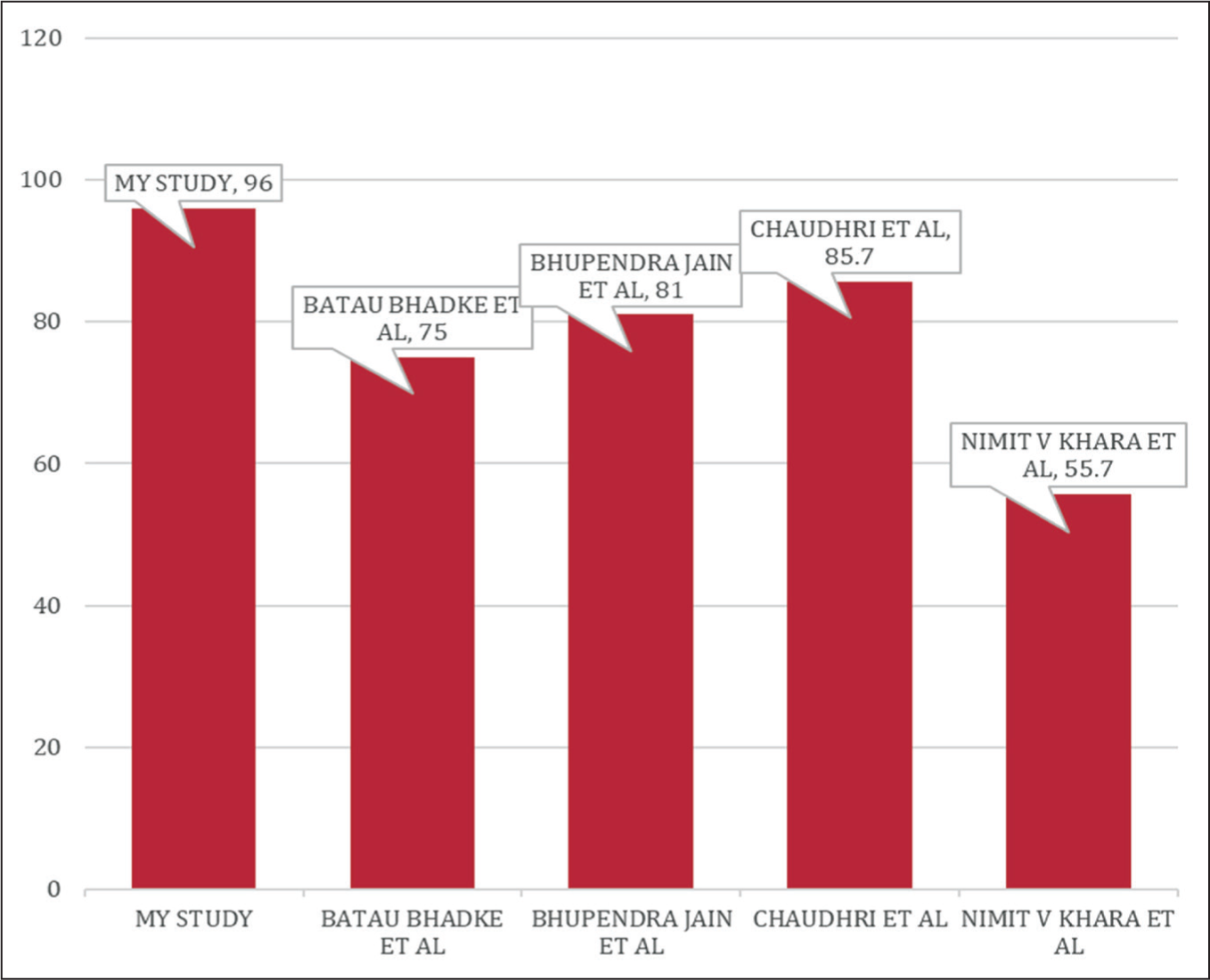
In this study, FOB identified the cause of NRP in 96% of cases (n = 47), a rate that exceeds those documented in earlier studies. Badke et al.[5] reported a diagnostic yield of 75%, Jain et al.[6] found 81% and Chaudhuri et al.[7] observed 85.7%.
In the present study and literature review, the majority of cases were found in males. In females, infections accounted for the majority of pneumonia cases compared to malignancy, while in males, infections were likewise the most common cause, but the incidence of malignant conditions was higher, likely due to the greater prevalence of smoking. Smoking-related impairment of mucociliary clearance further increases the risk of developing infectious pneumonia.
Most patients in this review were above 50 years of age, which can be attributed to decreased immunity and the presence of comorbid conditions, making them more susceptible compared to the younger population.
Radiological findings revealed that the right lung was more commonly affected than the left. In contrast, Chaudhuri et al.,[7] Jain et al.[6] and El-Shabrawy et al.[8] observed that the right upper lobe was the most commonly affected site.
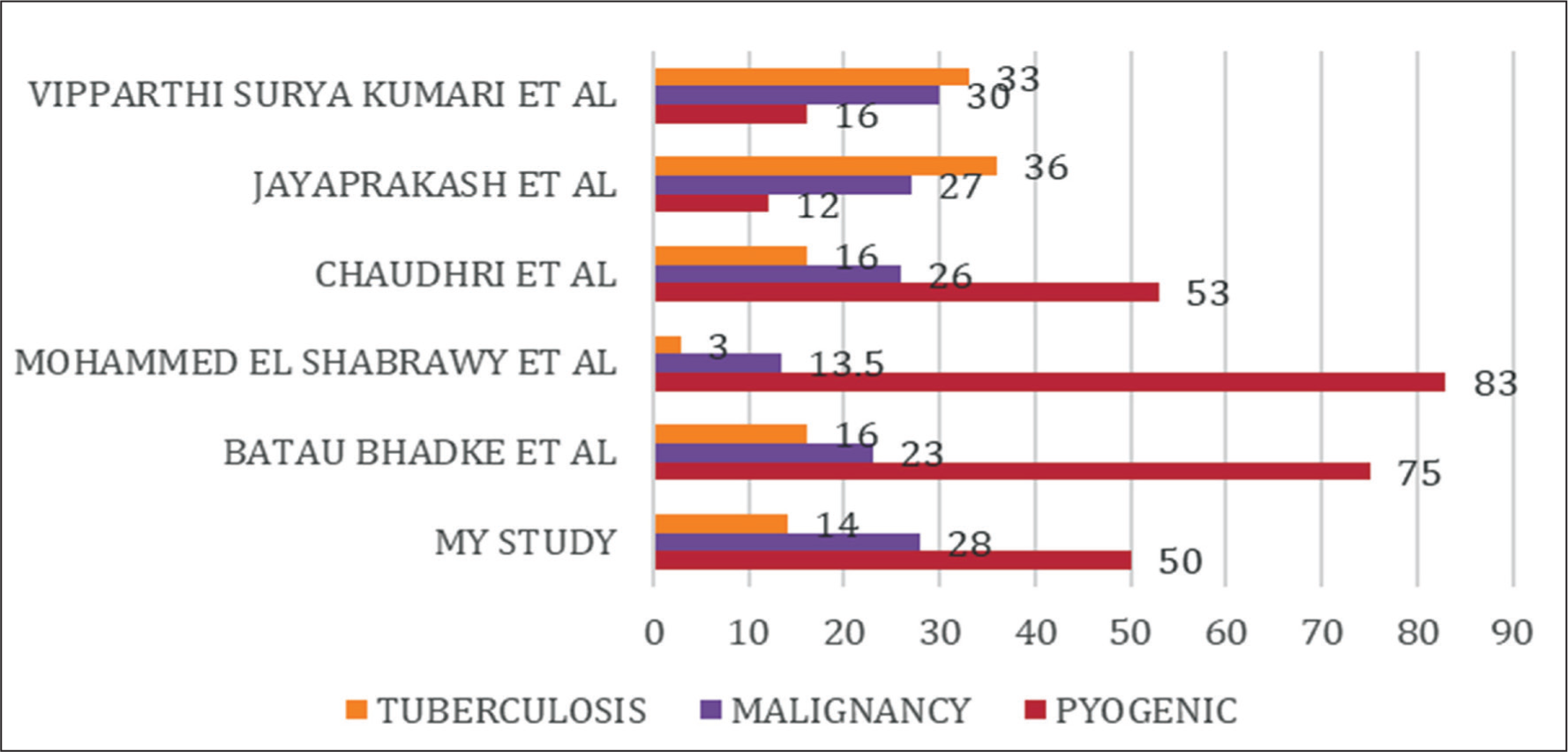
On gross inspection of the tracheobronchial tree, mucopurulent secretions were commonly noted. In this study, pyogenic bacterial infection accounted for the majority of NRP (50%), followed by neoplastic lesions (28%) and tuberculosis (14%). These results align with earlier reports by El-Shabrawy et al.,[8] Badke et al.,[5] and Chaudhuri et al.[7] and Jasari et al.[9] all of which highlighted bacterial infection as the predominant cause, with malignancy and tuberculosis as subsequent contributors.
Aetiology in Various Studies
El-Shabrawy et al.[8] studied 135 patients with NRP. The leading cause was pyogenic infection, seen in 113 patients (83.7%), followed by malignancy in 18 (13.5%) and tuberculosis in 4 (2.9%). Among infectious agents, Klebsiella pneumoniae was the most common isolate; next most frequent pathogens were Pseudomonas (19.65%) and Streptococcus pneumoniae (19.65%).
Jain et al.[6] and Chaudhuri et al.[7] evaluated the role of FOB and CT-guided FNAC in diagnosing NRP. In Jain’s study of 65 patients, pyogenic bacterial infections were the leading cause (37%), followed by tuberculosis (29.2%) and bronchogenic carcinoma (23%). Similarly, Chaudhuri’s study of 60 patients found pyogenic infection to be the predominant aetiology (53.3%), with bronchogenic carcinoma (26%) and tuberculosis (16.7%) as other major causes. Streptococcus pneumoniae was the most frequent pathogen in Jain’s cohort, whereas Klebsiella and Pseudomonas were more common in Chaudhuri’s. Both studies noted the right upper lobe as the most commonly affected site (25%). Regarding malignancy, Jain reported 15 cases of bronchogenic carcinoma without specifying subtypes, while Chaudhuri documented 16 cases, with squamous cell carcinoma being the most frequent (10 cases), followed by adenocarcinoma (5 cases). The diagnostic yield of FOB was high in both studies, with Chaudhuri et al. achieving 85.7% by FOB alone and 98.3% when combined with CT-guided FNAC.
Jayaprakash et al.[10] carried out a study in a tertiary care hospital in Kerala[9] assessed the causes and clinical outcomes of NRP. Among 821 patients admitted with pneumonia, 70 cases were identified as NRP. Tuberculosis emerged as the leading aetiology in 25 cases (35.7%), followed by malignancy in 19 cases (27.1%), drug-resistant bacterial infections in 10 (14.3%), Pneumocystis infection in 7.1% and bronchiolitis obliterans pneumonia in 5.7%. Among cancers, adenocarcinoma was the predominant subtype (42.1%). Among infections, Klebsiella species (60%) was the most frequent isolate. Smoking (60%) was the strongest risk factor associated with NRP, while diabetes mellitus, COPD and hypertension were other significant comorbidities.
Badke et al.[5] (2010) studied 120 patients who met the inclusion criteria and underwent FOB.[10] FOB yielded a definitive diagnosis in 90 patients (75%). The underlying etiologies were bacterial pneumonia in 32 cases (26.6%), malignancy in 28 (23.3%), pulmonary tuberculosis (PTB) in 20 (16.6%) and fungal pneumonia in 6 (5%). Among the bacterial infections, Streptococcus pneumoniae was the most frequent (16 patients, 50%), followed by Staphylococcus (10, 31.25%) and Klebsiella (6, 18.75%).
Kumari et al.[11] studied 32 patients with NRP who underwent FOB, lung FNAC and CT chest. Tuberculosis was the most common diagnosis, seen in 33.3% of patients, followed by malignancy (30.3%) and infections (16.6%). Diabetes mellitus was the leading comorbidity (23.3%), followed by COPD (20%) and hypertension (16.6%).
Similarly, Khara et al.[12] assessed the diagnostic value of FOB in 289 patients, reporting an overall diagnostic yield of 55.7%. The yield was 37.7% for PTB, 48.7% for pneumonia and highest at 68.5% for lung cancer.
Jasari et al.[9] investigated the role of FOB in diagnosing NRP among 34 patients. The majority of cases were attributed to bacterial infections, identified in 19 patients (55.88%), while bronchogenic carcinoma accounted for 8 cases (23.5%) and PTB for 6 cases (17.6%). Streptococcus pneumoniae emerged as the most common bacterial isolate, found in 8 patients (42.1%). Among the malignancies, adenocarcinoma was the predominant histological type (50%), followed by squamous cell carcinoma (25%), small cell carcinoma (12.5%) and large cell carcinoma.
Nikbakhsh et al.[13] conducted a study in Iran involving 290 patients with sputum smear-negative tuberculosis from 2006 to 2012.[14] All participants underwent FOB with BAL smear and culture. BAL smear was positive for TB bacilli in 110 patients, while in those with negative BAL smears, BAL culture detected TB bacilli in 64 cases (35.5%). The authors concluded that FOB-guided BAL serves as a rapid and reliable method for confirming the diagnosis of sputum smear-negative TB.
Brownback et al.[14] studied 133 individuals, including those on immunosuppressive therapy, HIV-positive patients, neutropenic individuals and recipients of haematopoietic stem cell or organ transplants. The diagnostic yield of FOB was 52.7%. Viral infections were the most common cause, detected in 38 (48.1%) patients, followed by bacterial infections in 9 (11%), invasive aspergillosis in 14 (17.7%) and Pneumocystis jiroveci in 6 (7.6%) cases. The study also found that BAL performed in the lower lobes provided a higher diagnostic yield.
The diagnostic yield and aetiology of different studies are summarised in charts (Figures 3 and 4).
Diagnostic yield of different studies
Aetiology of NRP in different studies
Conclusion
Bronchoscopy serves as a highly reliable tool in establishing the underlying cause of NRP, with a diagnostic yield of 94%. Infections remain the leading aetiology, with tuberculosis responsible for nearly half of the cases. TBLB is advised in about 85% of such patients to effectively rule out malignancy.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
REG.NO: 213/IEC AMC/AUG 2024.
Informed consent
Informed consent was taken from all the participants.
Credit author statement
D.V. Pratapa Reddy: Conceptualisation, methodology, investigation and writing.
V. Vijayakumari: Validation and supervision.
Neha Tarannum: Data curation, writing and visualisation.
R. Sunil Kumar: Supervision and project administration.
CH.R.N. Bhushana Rao: Supervision and project administration.
K. Premchand: Validation and supervision.
Data availability
Non-digital data curated at the Department of Pulmonary Medicine, Andhra Medical College, Visakhapatnam.
Use of artificial intelligence
N/A.