
Abstract
Background:
Tuberculosis (TB) remains a leading cause of morbidity and mortality worldwide, with extrapulmonary manifestations posing significant diagnostic challenges. Postpartum women are particularly vulnerable due to immune modulation, which may unmask latent TB or precipitate disseminated disease.
Case Presentation:
We report the case of a 29-year-old postpartum female who presented with fever, headache, and altered sensorium. Neuroimaging revealed parieto-occipital cortical hyperintensities and an internal capsule infarct, while cerebrospinal fluid analysis confirmed tuberculous meningitis (TBM) by GeneXpert MTB/RIF assay. High-resolution CT of the chest demonstrated bronchocentric nodular infiltrates and right lower lobe consolidation suggestive of pulmonary TB with aspiration. The clinical course was complicated by acute respiratory distress, with chest radiographs revealing diffuse bilateral pulmonary infiltrates and echocardiography showing diastolic dysfunction—consistent with flash pulmonary oedema (FPE). The patient responded well to antitubercular therapy, intravenous corticosteroids, and diuretics, with resolution of neurological and respiratory symptoms.
Conclusion:
This case highlights the complexity of multisystem TB in the postpartum period, presenting simultaneously with central nervous system involvement, pulmonary disease, and life-threatening hemodynamic complications such as FPE. Early multidisciplinary evaluation, integration of imaging, and the use of molecular diagnostics are critical for timely diagnosis and management in such atypical and high-risk presentations.
Keywords
Introduction
Tuberculosis (TB) remains a major global public health challenge, accounting for significant morbidity and mortality worldwide, with India contributing nearly 28% of the global TB burden according to the WHO Global Tuberculosis Report 2023.[1] While pulmonary TB constitutes the majority of cases, extrapulmonary TB accounts for approximately 15%–20% in immunocompetent individuals and up to 50% in immunocompromised states.[2] Among extrapulmonary forms, tuberculous meningitis (TBM) is the most severe, associated with high mortality and neurological sequelae, yet often underdiagnosed due to its insidious onset and nonspecific clinical features.[3]
The postpartum period is a unique immunological state characterised by immune reconstitution following pregnancy-induced immunosuppression. This shift can unmask latent infections or precipitate the progression of subclinical TB to disseminated disease.[4] The incidence of TBM in postpartum women is not well documented in large-scale studies; however, smaller series and regional data suggest that postpartum women account for 4%–6% of TBM cases in high-burden settings, with increased susceptibility within the first 6 months after delivery.[5,6]
The clinical diagnosis of TBM in postpartum women is particularly challenging because its presentation often overlaps with obstetric and neurological complications such as preeclampsia/eclampsia, posterior reversible encephalopathy syndrome (PRES), cerebral venous thrombosis (CVT), and reversible cerebral vasoconstriction syndrome (RCVS).[7] Neuroimaging plays a critical role in differentiating these conditions, and cerebrospinal fluid (CSF) molecular diagnostics—particularly the GeneXpert MTB/RIF assay—have markedly improved the diagnostic yield, especially in resource-limited settings.[8,9]
Cardiopulmonary complications in TBM are rare but can be life-threatening. Flash pulmonary oedema (FPE)—either neurogenic or cardiogenic—has been reported in association with acute CNS insults but remains exceptionally uncommon in TBM, particularly in postpartum women.[10] Understanding such multisystem involvement is essential for timely recognition and management.
In this report, we present a unique case of postpartum disseminated TB involving the CNS and lungs, complicated by recurrent FPE, and discuss its diagnostic challenges, management strategies, and relevance to clinical practice
Case Presentation
A 29-year-old right-handed woman, two months postpartum following an uncomplicated lower-segment caesarean section (LSCS), presented with a 10-day history of intermittent fever and a month-long worsening holocranial headache. Twenty-four hours before admission, she developed acute altered sensorium, preceded by transient blurring of vision lasting approximately 15 minutes. She denied seizures, focal weakness, or constitutional symptoms prior to this episode.
On arrival to our emergency department, she was drowsy with a Glasgow coma scale (GCS) score of E2V1M4, necessitating immediate intubation for airway protection. There was no pallor, icterus, lymphadenopathy, or pedal oedema. BMI was 18.6 kg/m². Neurological examination revealed meningeal signs, bilateral reactive pupils, normal extraocular movements, and preserved brainstem reflexes. Plantar responses were asymmetric—extensor on the right and flexor on the left—consistent with a left pyramidal tract lesion. No motor weakness was noted at presentation; however, over the next 48 hours, mild right upper limb pronator drift was observed, which resolved before discharge.
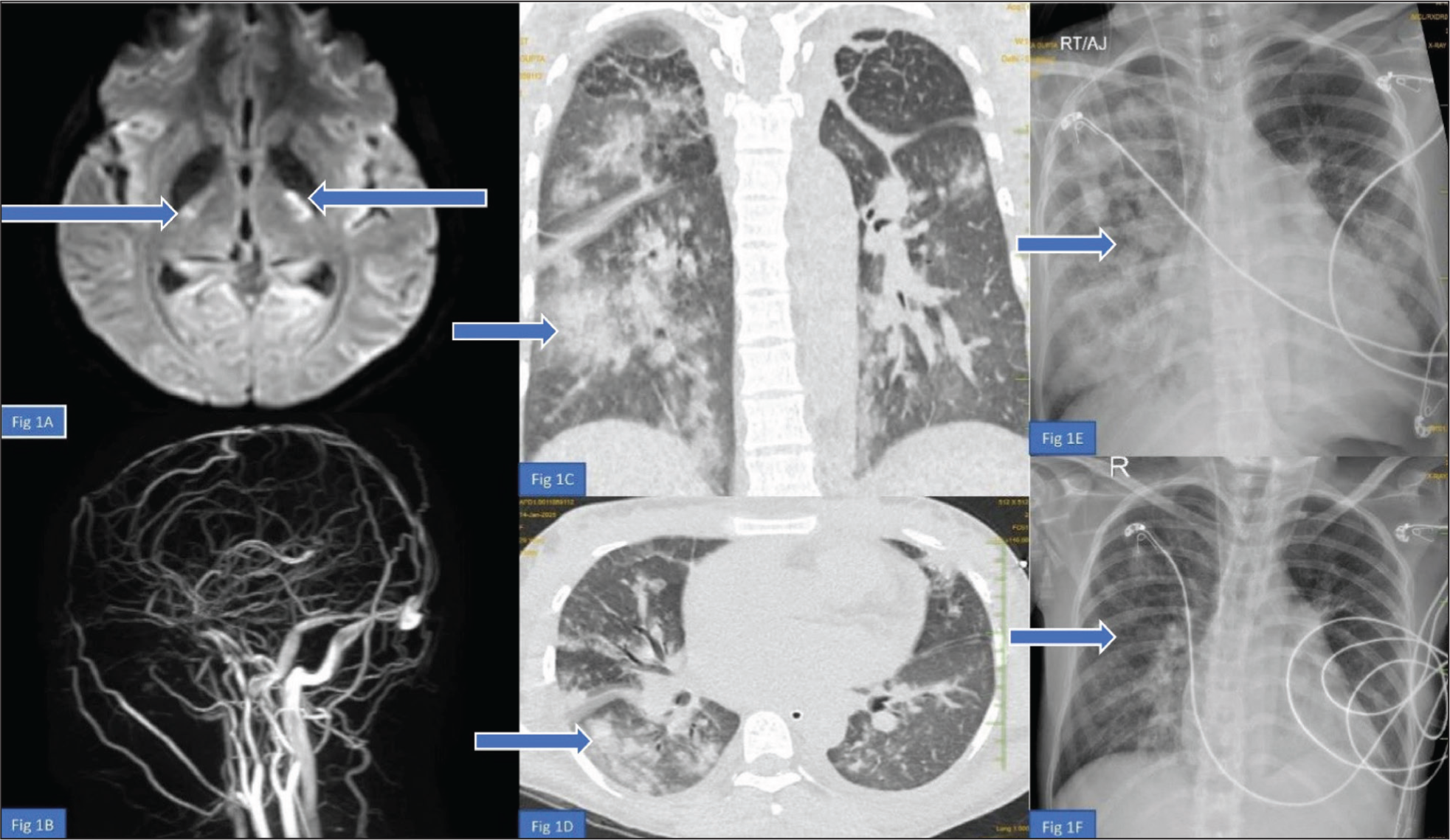
Neuroimaging with MRI brain and MR angiography/venography demonstrated acute ischaemic changes in the left internal capsule [Figure 1A], subcortical and cortical T2/FLAIR hyperintensities in the bilateral parieto-occipital lobes [Figure 1A], and absent flow in cortical venous sinuses [Figure 1B], raising suspicion for cortical vein thrombosis (CVT), PRES, or tuberculous vasculopathy. The deep venous system was patent. Although MRV suggested absent cortical venous flow, the absence of venous infarcts, lack of deep venous system involvement, and overlapping vasculitic features made the diagnosis of CVT uncertain. Anticoagulation was therefore deferred to avoid potential haemorrhagic risk in the setting of CNS infection, and high-dose corticosteroids were initiated for suspected TB vasculitis.
(A) MRI brain (Axial FLAIR), focal acute area of ischaemia involving the body of the left internal capsule. Findings are consistent with tubercular vasculitis. (B) MR venography (MRV) shows the absence of flow in cortical venous sinuses, raising suspicion of cerebral venous thrombosis (CVT) in the setting of tuberculous meningitis. (C & D) Chest HRCT (coronal and axial views), discrete and confluent bronchocentric nodular infiltrates involving both lungs, consistent with infective respiratory bronchiolitis. A large right lower lobe consolidation is also noted, suggestive of aspiration pneumonia. (E) Chest X-ray (CXR) post-extubation diffuse airspace opacities over bilateral lung fields (right > left), with mild left-sided pleural effusion. Radiological features are suggestive of flash pulmonary oedema. (F) CXR Post IV Diuretics and Steroid Therapy: Confluent airspace opacities in both lung fields, with mild left-sided pleural effusion seen after initiation of diuretics and corticosteroid therapy, showing partial radiological resolution of pulmonary oedema
CSF analysis revealed no organisms on Gram, fungal, or Ziehl–Neelsen staining, and cultures were sterile. GeneXpert MTB/RIF assay on CSF was positive for Mycobacterium tuberculosis (trace detected), confirming TBM [Figure 2]. Given the subacute presentation, neuroimaging findings suggestive of vasculitis, and the high morbidity of treatment delay, antitubercular therapy (ATT) was initiated empirically before culture confirmation and HIV test results. Aspirin (150 mg/day) was added following MRI confirmation of ischaemic infarct, as there was no haemorrhagic contraindication.
Respiratory examination revealed bilateral crepitus (right > left). Arterial blood gas showed primary respiratory acidosis (pH 7.29, pCO2 61.8 mmHg, HCO3 – 30.2 mmol/L). Chest HRCT demonstrated discrete and confluent bronchocentric nodular infiltrates bilaterally, with a large right lower lobe consolidation suggestive of aspiration pneumonia [Figure 1C and 1D]. BAL GeneXpert MTB/RIF was also positive (trace detected), confirming pulmonary TB.
On Day 3, shortly after extubation, she developed acute respiratory distress. Chest X-ray revealed diffuse bilateral interstitial opacities, mild cardiomegaly, and upper lobe venous diversion [Figure 1E]. Echocardiography showed mild left atrial dilation, concentric LV hypertrophy, elevated LV end-diastolic pressure, preserved systolic function (EF 55%), and minimal pericardial effusion. NT-proBNP was markedly elevated (32,457 pg/mL), and hs-TnI was 52.2 pg/mL—consistent with FPE. She showed rapid improvement following intravenous furosemide and methylprednisolone [Figure 1F].
On Day 7, a second episode of acute respiratory distress occurred, with worsening bilateral airspace opacities and pleural effusions. Repeat echocardiography confirmed persistent diastolic dysfunction with minimal pericardial effusion. Given the temporal association with CNS insult, neurogenic mechanisms were considered contributory. Both episodes resolved completely with diuretics and corticosteroids.
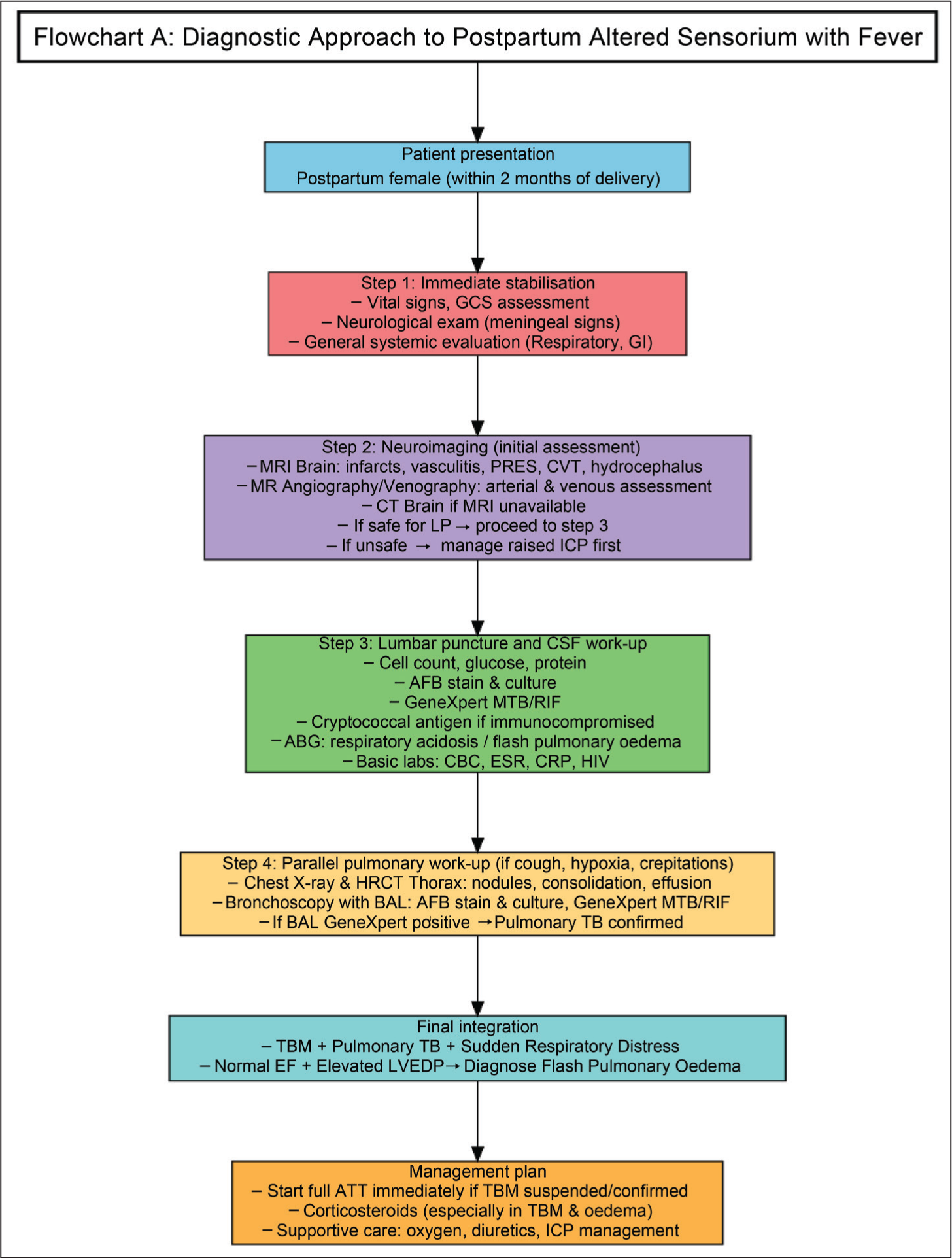
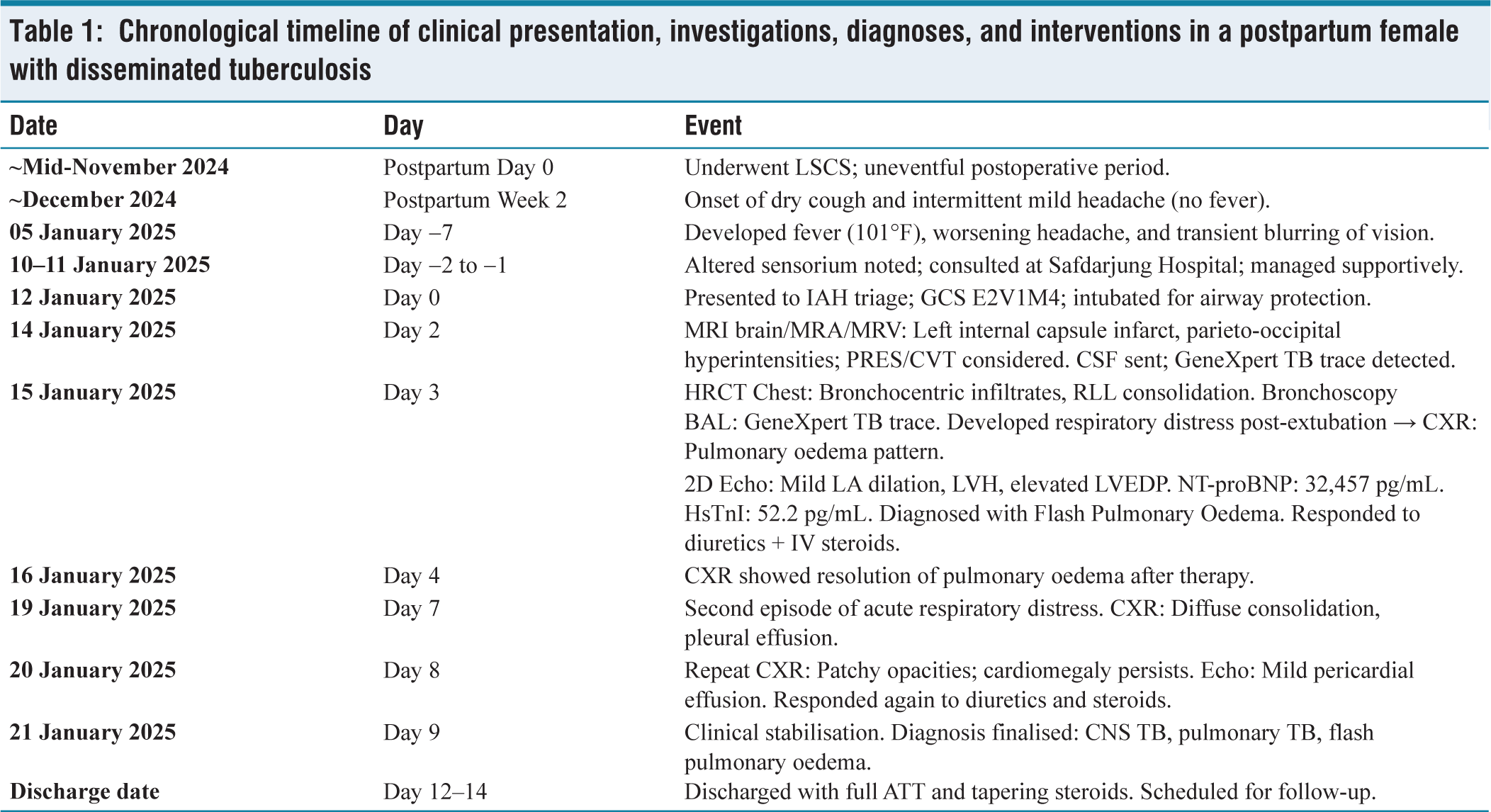
By Day 9, she was neurologically stable, with no residual focal deficits. She was discharged on full ATT, tapering corticosteroids, and aspirin, with scheduled follow-up. The final diagnosis included TBM, pulmonary TB with aspiration, and recurrent FPE due to probable neurogenic and diastolic dysfunction mechanisms. A chronological summary of the patient’s clinical course, investigations, and key interventions is outlined in Table 1. A stepwise diagnostic approach integrating neuroimaging, CSF molecular testing, pulmonary evaluation, and cardiac assessment [Figure 2] was essential in confirming postpartum disseminated TB with TBM, pulmonary TB, ischaemic infarct due to TB vasculitis, and recurrent FPE.
Chronological timeline of clinical presentation, investigations, diagnoses, and interventions in a postpartum female with disseminated tuberculosis
Discussion
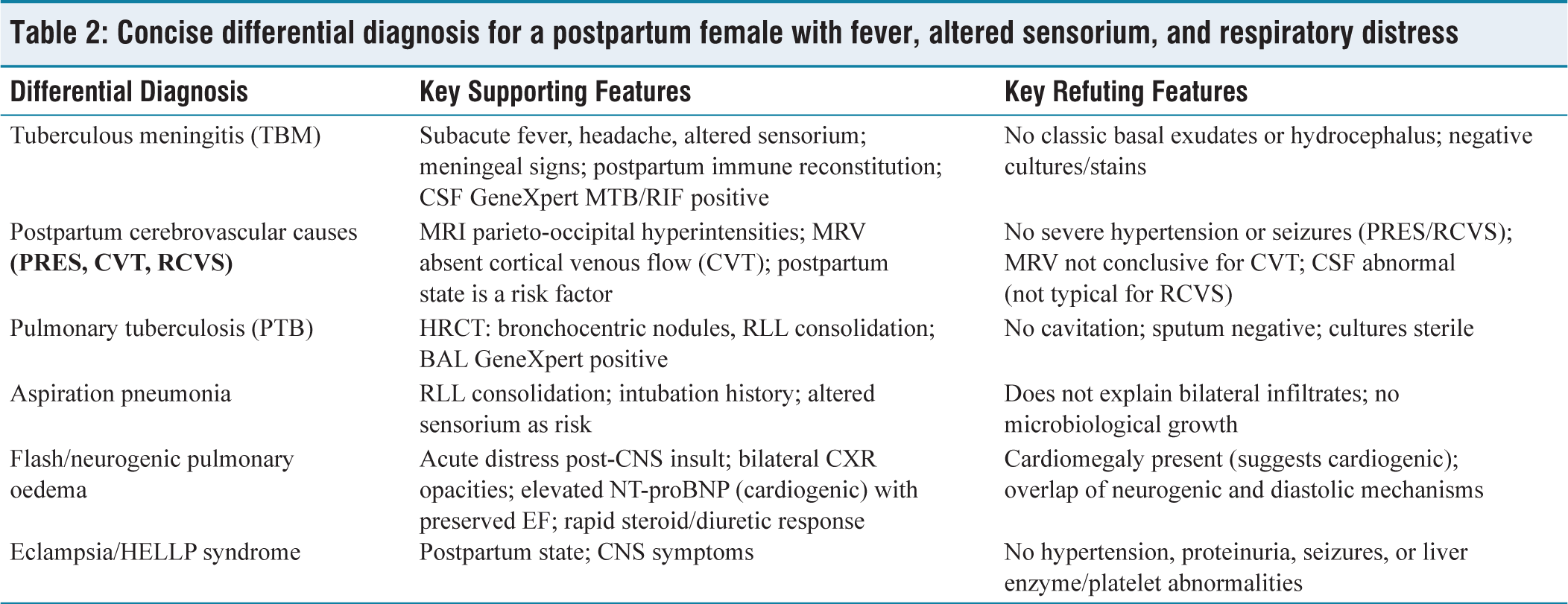
TB remains a major global health challenge, with extrapulmonary TB comprising 15%–20% of cases in immunocompetent individuals and up to 50% in immunocompromised states, including pregnancy and the postpartum period.[1,2] The postpartum period is a recognised high-risk window due to immune reconstitution, which can unmask latent TB or accelerate progression of subclinical disease.[4] Among extrapulmonary forms, TBM is the most severe, with high mortality and disability if not promptly diagnosed and treated.[3] Several differential diagnoses were considered based on the patient’s clinical, radiological, and laboratory features, summarised in Table 2.
Concise differential diagnosis for a postpartum female with fever, altered sensorium, and respiratory distress
In this patient, TBM was confirmed by CSF GeneXpert MTB/RIF positivity and neuroimaging features of vasculitis with parieto-occipital cortical-subcortical hyperintensities. Such imaging patterns may mimic PRES, CVT, or RCVS—all recognised postpartum neurological complications.[7,11] Early MRI/MRV and rapid molecular diagnostics facilitated the timely initiation of ATT, a critical factor in improving TBM outcomes.
An ischaemic infarct in the left internal capsule, likely secondary to TB vasculitis, was identified on MRI. Plantar asymmetry and transient mild right upper limb pronator drift corresponded to this lesion. Management of TB vasculitis involves prompt ATT, adjunctive corticosteroids to reduce inflammatory vascular injury, and antiplatelet therapy when ischaemic infarcts are present.[9,12] In our patient, aspirin was initiated after confirming the infarct and ruling out haemorrhage.
Pulmonary involvement, confirmed by HRCT and BAL GeneXpert positivity, was consistent with bronchocentric granulomatous TB and aspiration pneumonia. Pulmonary TB coexisting with TBM is common in disseminated disease, occurring in up to half of cases.[13]
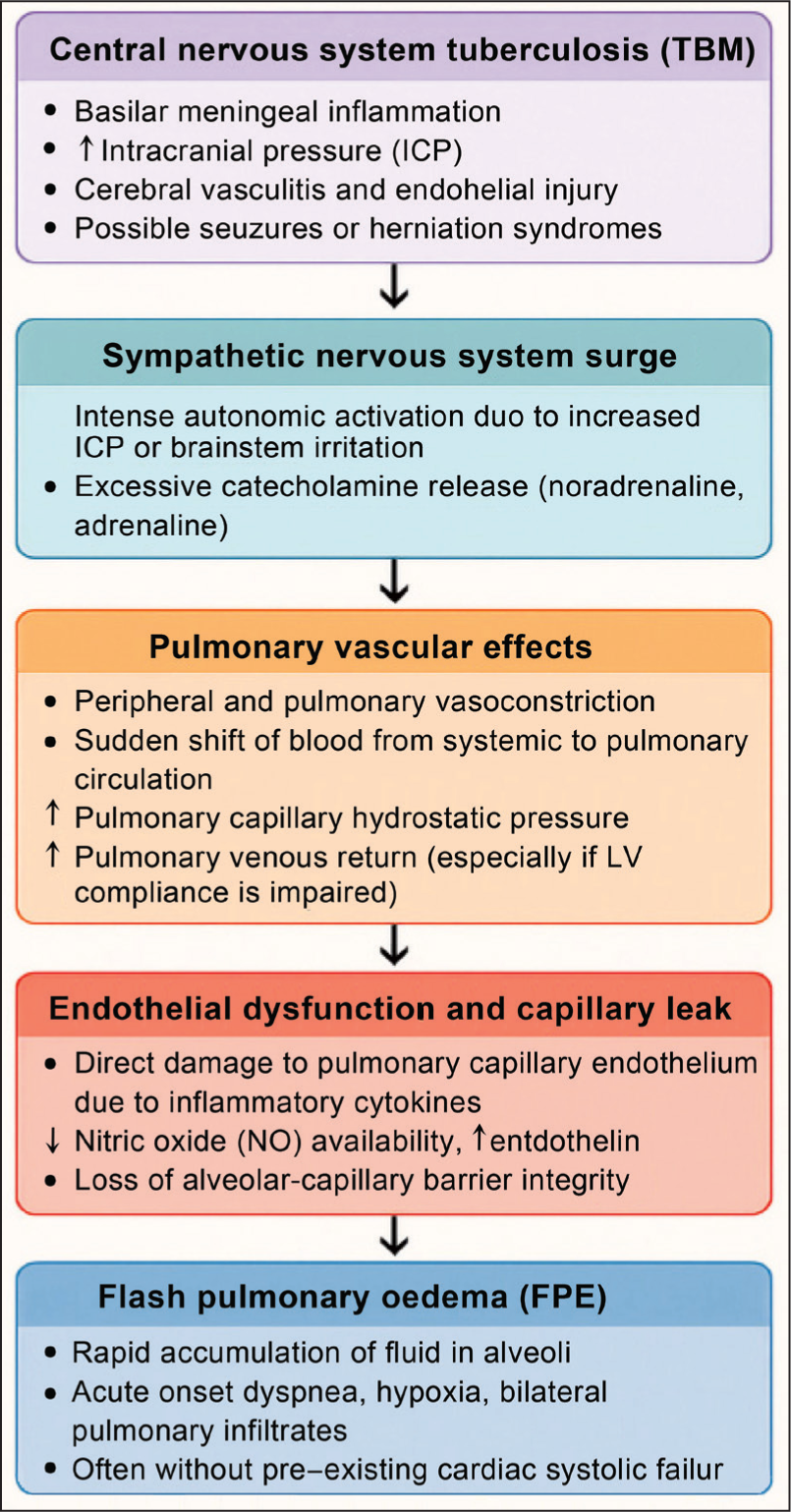
The most striking and unique feature of this case was two discrete episodes of FPE during the same admission—a phenomenon rarely documented in TBM and, to our knowledge, not previously reported in postpartum TBM. Prior reports describe only single-episode pulmonary oedema in CNS TB,[14–16] usually attributed to a neurogenic mechanism. In our patient, echocardiographic findings (preserved systolic function, diastolic dysfunction, elevated LV end-diastolic pressure) and markedly raised NT-proBNP supported a cardiogenic mechanism, while the close temporal association with CNS insult suggested an overlapping neurogenic component. The combined pathophysiological cascade is illustrated in Figure 3.
Pathophysiological mechanisms leading to flash pulmonary oedema in tuberculous meningitis (TBM). This flowchart illustrates the stepwise cascade beginning with central nervous system inflammation in TBM, leading to sympathetic nervous system overactivation, pulmonary vasoconstriction, endothelial injury, and, in some cases, coexisting diastolic dysfunction—ultimately resulting in flash pulmonary oedema. The combination of neurogenic and cardiogenic mechanisms contributes to sudden pulmonary fluid overload and hypoxia in such patients
This case reinforces several key clinical lessons:
Postpartum disseminated TB can present with rare, life-threatening complications such as recurrent FPE. GeneXpert has been shown to improve diagnostic accuracy in TBM, especially in resource-limited or high-burden settings.[8] Early echocardiography and NT-proBNP measurement are essential in differentiating cardiogenic from neurogenic pulmonary oedema. Multidisciplinary management—integrating neurology, infectious diseases, pulmonology and cardiology—is vital for favourable outcomes.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the Departments of Neurology, Pulmonology, Obstetrics, and Critical Care at Indraprastha Apollo Hospitals for their multidisciplinary efforts in managing this complex case.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Informed consent
Written informed consent was obtained from the patient’s legal guardian for publication of this case report and accompanying clinical details.
Credit author statement
Dr Ramesh Krishnan: Clinical Evaluation, Neurological Management, Manuscript Writing.
Dr Pushpendra Nath Renjen: Neurology Oversight, Manuscript Review and Guidance.
Dr Avinash Gosawmi: Case Coordination, Literature Review, Manuscript Editing.
Data availability
All relevant clinical and investigational data related to this case are available from the corresponding author upon reasonable request.
Use of artificial intelligence
No AI tools were used in the preparation or writing of this manuscript.