
Abstract
Background:
Medically unexplained symptoms (MUS) are common in clinical practice, often leading to repeated investigations, escalating healthcare costs, and patient distress. Despite their high prevalence, MUS are frequently mismanaged due to delayed psychiatric involvement, resulting in fragmented care and poor outcomes.
Objective:
To highlight the diagnostic and therapeutic relevance of psychiatric evaluation in patients with persistent physical symptoms lacking an organic basis.
Methods:
This retrospective case series describes six individuals (aged 22–55) who presented with chronic, unexplained physical symptoms across various specialities in a tertiary care hospital. All underwent extensive investigations with no definitive organic diagnosis. Upon referral to psychiatry, they were assessed using ICD-10 criteria and relevant symptom severity scales. Diagnoses included somatisation disorder (n = 4), somatoform pain disorder (n = 1), and factitious disorder (Münchausen syndrome) (n = 1). Interventions included SSRIs/SNRIs, psychoeducation, cognitive-behavioural therapy (CBT), and supportive psychotherapy. Follow-up ranged from 1 to 3 months.
Results:
Five of six patients showed significant clinical improvement within 3 months of psychiatric intervention. Unnecessary investigations ceased, functional recovery improved, and health service use decreased. The Münchausen case demonstrated partial engagement but reduced hospital-seeking behaviour.
Conclusion:
Early psychiatric evaluation is pivotal in the management of MUS. Consultation-liaison psychiatry plays a crucial role in bridging the mind-body gap, reducing healthcare burden, and improving outcomes through integrated care.
Keywords
Introduction
Medically unexplained symptoms (MUS) are physical complaints that persist despite appropriate medical evaluations and lack a clear organic cause.[1] These symptoms—commonly including fatigue, pain, gastrointestinal distress, and neurological disturbances—are frequently encountered across specialities, accounting for up to 30% of consultations in outpatient settings.[2]
In many cases, these presentations reflect somatisation, where psychological distress manifests as bodily symptoms. This may occur without the patient being aware of the psychological origin, making the diagnosis difficult. Variants include somatoform pain disorder, illness anxiety disorder, and factitious disorders. Patients often resist psychiatric explanations, influenced by stigma and misconceptions, leading to repeated investigations and fragmented care.[3]
Such delays can cause emotional and financial distress and increase the risk of unnecessary procedures.[4] Factitious disorders like Münchausen syndrome pose further diagnostic and ethical challenges due to the intentional production of symptoms, often without external incentives. Despite its high clinical and economic burden, MUS remains under-recognised, especially in India, where structured psychiatric referral is often lacking.[5]
This case series presents six patients with MUS who, after extensive investigations across specialities, were referred to psychiatry. Diagnoses included somatisation disorder (n = 4), somatoform pain disorder (n = 1), and factitious disorder (n = 1). These cases highlight the crucial role of early psychiatric evaluation in improving outcomes and reducing healthcare strain.
Methods
This is a retrospective descriptive case series from a tertiary healthcare centre in Kolkata, West Bengal. The hospital has an established liaison psychiatric service actively involved in inpatient and outpatient referrals from medicine, surgery, neurology, dermatology, and other specialities.
Six individuals aged between 22 and 45 years, presenting to various medical specialities with persistent physical complaints lacking a clear organic basis, are reported here. All patients had undergone extensive medical investigations (laboratory, imaging, speciality consultations), with no conclusive medical diagnosis explaining the symptomatology. They were referred to a psychiatrist between January 2025 and March 2025.
Inclusion criteria:
Age 18 years and above At least 3 months’ history of physical symptoms without a consistent organic aetiology Documented referral from a non-psychiatric speciality Final diagnosis consistent with neurotic, stress-related, and somatoform disorders (as per the ICD-10 classification)
Exclusion criteria:
Known neurological or systemic illnesses with a confirmed organic basis Cognitive impairment impeding psychiatric assessment History of substance use disorder influencing symptoms
All six patients were evaluated by a consultant psychiatrist based on ICD-10 diagnostic criteria.[6] In addition to somatisation disorder (n = 4), one patient fulfilled criteria for persistent somatoform pain disorder, and another for factitious disorder imposed on self (Münchausen syndrome).
Each patient also underwent:
Treatment included a combination of psychoeducation, pharmacotherapy (SSRIs or tricyclic antidepressants), and structured psychotherapeutic interventions such as cognitive behavioural therapy (CBT) and supportive psychotherapy. The patients were followed up over 1 to 3 months post-psychiatric referral. Treatment adherence, symptom resolution, and functional improvement were documented.
Verbal informed consent was obtained from each patient for the use of anonymised clinical data. It was obtained in their own language.
Case Description
Six individuals with persistent, distressing physical symptoms unaccounted for by medical diagnoses were referred from various departments to psychiatry over three months. The demographic and clinical profiles varied, yet all had undergone extensive investigations and multiple consultations across specialities prior to psychiatric evaluation. A brief summary of each case is provided below:
Case 1: Somatisation Disorder (Gastrointestinal Focus)
A 28-year-old woman presented with recurrent abdominal pain, bloating, and altered bowel habits for over a year. Despite repeated gastroenterological workups, including endoscopy, colonoscopy, and CT abdomen, no organic pathology was identified. She had visited three hospitals and was on various proton pump inhibitors and antispasmodics. Psychiatric evaluation revealed significant health anxiety and unresolved grief due to a miscarriage a year ago. She was started on escitalopram 10 mg/day and supportive psychotherapy. Over 3 months, she reported a marked reduction in symptom distress and healthcare-seeking behaviour.
Case 2: Somatisation Disorder (Cardiorespiratory Focus)
A 35-year-old male with multiple emergency visits for chest tightness, palpitations, and breathlessness underwent cardiology and pulmonology evaluations, including ECGs, echocardiogram, Holter monitoring, and spirometry—all normal. Psychiatric assessment revealed panic episodes and workplace-related stress. Diagnosis of somatisation disorder with panic features was made. He responded well to sertraline 50 mg/day and CBT. He resumed work with no further ER visits by the 2-month follow-up.
Case 3: Somatisation Disorder (Neurological Focus)
A 40-year-old homemaker presented with frequent episodes of limb weakness, tingling, and transient speech arrest. Neurology evaluation, including MRI brain, EEG, and nerve conduction studies, was normal. She had already received multiple neurovitamins and anxiolytics without improvement. Psychiatric evaluation suggested a somatoform conversion subtype. She was initiated on amitriptyline 25 mg/night along with relaxation therapy. At 1-month follow-up, symptoms had significantly reduced in frequency.
Case 4: Somatisation Disorder (Multiple Systems)
A 22-year-old male engineering student complained of fatigue, headache, nausea, and joint pains for 6 months. Extensive rheumatology, endocrinology, and infectious disease workups were inconclusive. He had a history of academic stress and insomnia. Somatisation disorder with underlying dysthymia was diagnosed. Fluoxetine 20 mg/day was prescribed with problem-solving therapy. At 3 months, he reported improvement in fatigue and resumed regular classes.
Case 5: Somatoform Pain Disorder
A 45-year-old female had persistent lower back and pelvic pain for over 2 years. Orthopaedic, gynaecological, and neurological evaluations found no aetiology. Pain symptoms were inconsistent with imaging and unresponsive to analgesics. She had a background of spousal neglect and chronic low mood. She was started on duloxetine 30 mg/day and engaged in pain-focused CBT. Her pain scores reduced by 50% at 2 months, and she reported improved functionality.
Case 6: Factitious Disorder (Münchausen Syndrome)
A 33-year-old male nurse repeatedly presented with self-reported seizures, unexplained bruises, and haematuria. Investigations across departments revealed inconsistencies; video EEG ruled out seizures. He was eventually caught falsifying urine samples and injecting himself with unknown substances. Psychiatric interview revealed a pattern of hospital-seeking behaviour since adolescence, with no external gain. Diagnosed with Münchausen syndrome, he was offered psychotherapy and family counselling. Engagement was partial, but he dropped out at the 1-month follow-up.
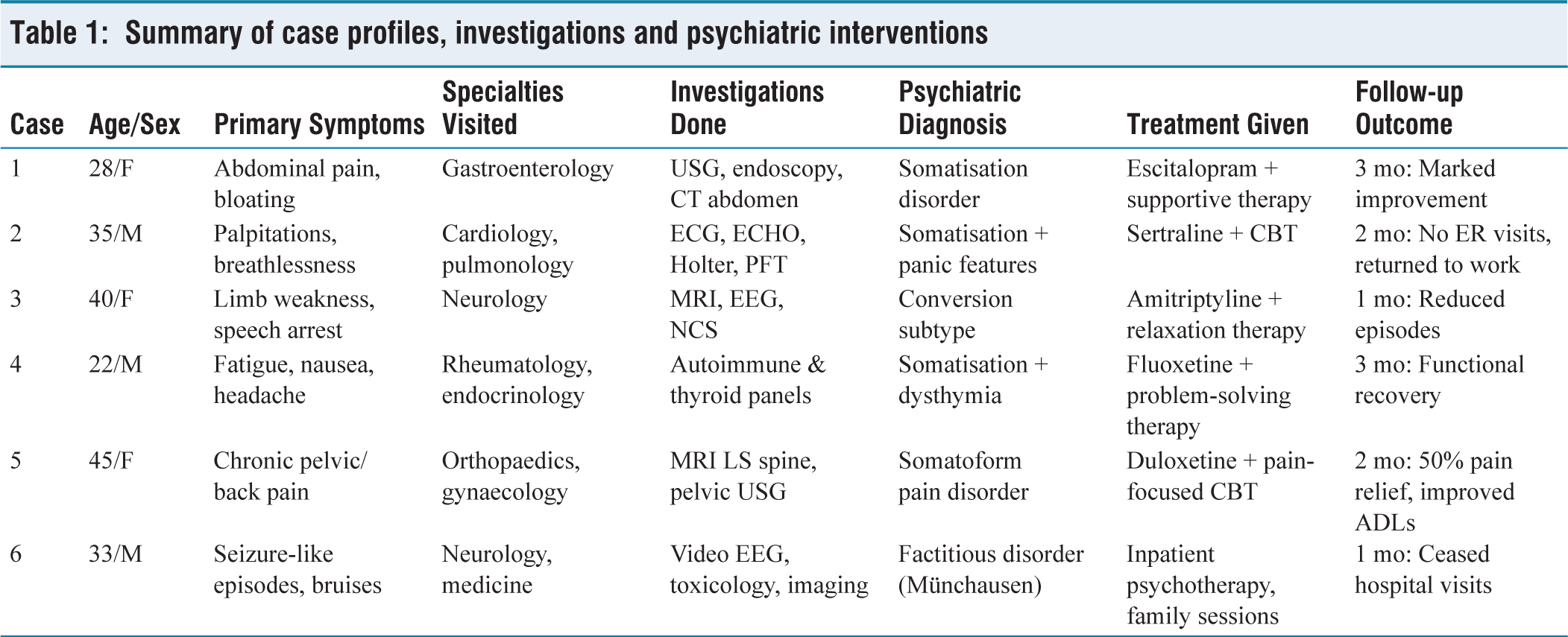
Table 1 summarises the clinical and treatment details of these six individuals.
Summary of case profiles, investigations and psychiatric interventions
Discussion
This case series underscores the multifaceted clinical burden and diagnostic ambiguity associated with MUS, a category that bridges the disciplines of psychiatry and medicine. Across the six cases presented, a common pattern emerges: prolonged suffering, inconclusive diagnostic investigations, multiple speciality consultations, and a delayed yet ultimately transformative psychiatric referral. These findings reflect the existing literature, which consistently documents high health service utilisation and suboptimal outcomes in MUS without integrated psychiatric care.[10]
MUS represents not merely a diagnostic vacuum but a manifestation of distress shaped by biological vulnerability, psychological conflict, and sociocultural context. In Indian settings, where mental illness is often stigmatised or misattributed to ‘weakness’ or ‘overthinking’, somatisation becomes an acceptable idiom of distress. Patients presenting with chest pain, breathlessness, or limb weakness are more likely to be taken seriously in medical settings than those describing anxiety or low mood. This ‘medicalisation of suffering’ was evident in all our cases, where physical complaints overshadowed underlying psychosocial turmoil until psychiatric consultation was sought.[3]
The predominance of somatisation disorder in four of the six cases mirrors epidemiological data suggesting it to be the most prevalent among somatoform conditions in outpatient settings.[11] These patients often exhibit heightened interoceptive sensitivity, amplifying bodily sensations that are benign in origin but interpreted as ominous due to illness anxiety and cognitive distortions. For example, the patient with abdominal complaints (Case 1) had undergone multiple unnecessary tests when psychological grief was the root cause. Her recovery post-psychiatric referral was rapid once the psychosocial stressor was addressed.
Similarly, the case of somatoform pain disorder (Case 5) illustrates how chronic pain, when devoid of a clear organic aetiology, is often attributed to obscure or even mythical diagnoses. Patients may receive a range of empiric treatments—from vitamins to unproven herbal remedies—while the emotional context of the pain remains unexplored. This aligns with findings that suggest up to two-thirds of chronic pain patients have concurrent affective disorders or maladaptive coping strategies.[12,13]
Münchausen syndrome, represented by Case 6, is an extreme form of factitious disorder often missed due to its rarity and the clinician’s discomfort in confronting deception. However, its presence in medical wards can significantly drain resources and disrupt therapeutic rapport. These individuals require non-judgemental yet firm containment strategies, intensive psychotherapy, and often long-term psychiatric supervision.[14] Notably, in this case, even a partial engagement in therapy led to cessation of emergency visits—demonstrating the importance of coordinated care.
From a treatment perspective, most patients in this series benefited from low-dose antidepressants such as SSRIs and SNRIs, combined with non-pharmacological interventions like psychoeducation and CBT. This approach reflects international best practices, which recommend integrated care pathways for MUS involving both psychiatric and primary care professionals.[15] The goal is not only symptom remission but restoration of function, reduction of unnecessary healthcare use, and enhancement of patient insight.
The early improvement seen in five of the six patients within 1–3 months challenges the myth that MUS is inherently chronic or treatment-resistant. It reinforces that with the right approach, even longstanding cases can improve. This has practical implications: primary care physicians and specialists should be trained to recognise red flags of somatisation, such as shifting symptoms, lack of correlation with investigations, emotional dysregulation, or a long list of prior consultations.[16]
In the Indian context, the reluctance to involve psychiatry early in the care pathway remains a formidable barrier. Fear of stigma, misbeliefs about ‘madness’, and lack of awareness among general physicians contribute to diagnostic delay. Moreover, health insurance policies often do not cover psychiatric treatment, adding financial hurdles. Our series shows that even basic psychiatric interventions—when integrated into medical care—can offer cost-effective and meaningful outcomes.
This series also highlights a systemic issue: over-reliance on investigations. The tendency to keep ‘ruling out’ rare diseases often delays diagnosis and increases patient frustration. It reflects a deeper discomfort among clinicians in addressing emotional issues, perhaps due to a lack of training in mental health.
However, an important consideration in the evolving understanding of these disorders is the shift in diagnostic nosology. While ICD-10 relied heavily on the construct of somatoform disorders and the requirement that symptoms be “medically unexplained,” DSM-5 has moved away from this approach, introducing the category of somatic symptom and related disorders.[17] This reclassification emphasizes the patient’s disproportionate thoughts, feelings, and behaviors about their symptoms rather than the absence of a medical explanation. Such a change reduces the stigma attached to being told that symptoms are “all in the mind” and acknowledges the genuine suffering of patients, regardless of whether an organic etiology is identified. In clinical practice, however, the absence of a definitive diagnosis often leads to frustration for both patients and their families, fostering repeated consultations, poor compliance, and mistrust of the medical system.[18] This underscores the need for careful psychoeducation, empathic communication, and a focused physical examination, which can validate the patient’s distress while also facilitating early psychiatric intervention.
Limitations
This case series has certain limitations. The small sample size (n = 6) and retrospective design limit generalisability. All patients were selected from a tertiary care setting and may not represent those in primary care or rural settings. The follow-up duration was short (1–3 months), which does not allow for conclusions about long-term outcomes or relapse rates. Additionally, while validated psychiatric tools were used, standardised somatic symptom severity scales such as the SSS-8 were not applied uniformly. Finally, there was no control group or comparator, and improvements were based on clinical judgement and subjective patient reports.
Conclusion
MUS remain a significant diagnostic and therapeutic challenge in general medical practice, often leading to over-investigation, patient distress, and fragmented care. This case series illustrates the diverse ways in which MUS can present—across systems and specialities—and highlights the potential of timely psychiatric referral. The patients described, despite prolonged suffering and multiple failed treatments, demonstrated clear improvement with simple, structured psychiatric interventions, underscoring that MUS is not untreatable—it is simply often mistreated or misunderstood.
A critical takeaway from this series is the indispensable role of consultation-liaison psychiatry in the multidisciplinary care of MUS. Psychiatric involvement not only aids diagnosis but also bridges the mind-body gap that commonly impedes effective treatment.
In the Indian healthcare landscape, where time, resources, and awareness are often constrained, integrating psychiatric expertise into routine medical practice is no longer optional—it is essential. Training clinicians to recognise early signs of somatisation, normalising psychiatric referral, and embedding liaison services in hospital systems are key steps toward holistic and humane patient care.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
N/A.
Informed consent
Verbal informed consent was obtained from each patient for the use of anonymised clinical data. It was obtained in their own language.
Credit author statement
Debanjan Banerjee: Conceptualisation, data curation, methodology, writing – original draft, writing – reviewing and editing.
Jayanta Sharma: Conceptualisation, data curation, writing – reviewing and editing.
Akash Roy: Conceptualisation, data curation, writing – reviewing and editing.
Aritra Konar: Conceptualisation, data curation, writing – reviewing and editing.
Debabrata Chakraborty: Conceptualisation, data curation, writing – reviewing and editing.
Data availability
Available on request.
Use of artificial intelligence
None.