
Abstract
Background:
Proximal humerus fractures are frequently encountered injuries, particularly among the elderly with osteoporotic bones. Complex three-part and four-part fractures present unique treatment challenges. Surgical management using locking plates, notably the Proximal Humeral Internal Locking System (PHILOS™) plate, offers stable fixation and promotes early mobilisation.
Methods:
This prospective study included 24 adult patients with Neer type three-part and four-part proximal humerus fractures who underwent open reduction and internal fixation (ORIF) with PHILOS™ system plating. Demographic data, fracture type, side affected, mechanism of injury and complications were documented. Functional outcomes were evaluated using the Constant-Murley score at 6 weeks, 3 months, 6 months and 12 months postoperatively. Statistical analysis was conducted using statistical package for the social sciences (SPSS) software.
Results:
The mean patient age was 50.95 years. Females comprised 58.3% of the cohort. Right-sided involvement was more common (58.3%). Road traffic accidents (RTA) (66.7%) were the predominant mechanism of injury. Nineteen patients had three-part fractures, whereas five had four-part fractures. At 1 year, 33.3% had excellent outcomes, 62.5% had good outcomes and 4.2% had poor outcomes. One patient developed shoulder stiffness due to non-compliance with physiotherapy. No cases of infection, avascular necrosis (AVN), nonunion or implant failure were noted.
Conclusions:
ORIF with PHILOS™ plate is a reliable method for managing complex proximal humerus fractures, yielding favourable functional outcomes and low complication rates. Success hinges on anatomical reduction, stable fixation and dedicated rehabilitation.
Keywords
Introduction
Fractures of the proximal humerus account for approximately 6% of all adult fractures and are the third most common osteoporotic fracture after those of the hip and distal radius.[1,2] These injuries predominantly affect elderly individuals, especially postmenopausal women, owing to reduced bone mineral density. However, they also occur in younger populations due to high-energy trauma such as road traffic accidents (RTA).[3] Among these fractures, three-part and four-part fracture patterns, as described in the Neer classification, are particularly complex, comprising up to 16% of proximal humerus fractures and often associated with poor outcomes if not appropriately treated.[4]
It is well established that non-displaced or minimally displaced fractures can be managed conservatively with acceptable functional recovery.[5] However, displaced multi-part fractures are prone to complications such as malunion, nonunion, avascular necrosis (AVN) and joint stiffness when treated non-operatively.[6] This has led to an increasing trend toward surgical management for three-part and four-part fractures. Several operative options exist, including percutaneous pinning, intramedullary nailing, hemiarthroplasty and open reduction and internal fixation (ORIF) using locking compression plates.[7–9] Each technique has distinct biomechanical and clinical profiles, with varying degrees of success.
Recent advances in implant design have favoured the use of anatomically contoured locking plates, such as the Proximal Humeral Internal Locking System (PHILOS™) plate, which provide angular stability and are especially useful in osteoporotic bone.[10,11] Biomechanical studies and early clinical reports suggest that the PHILOS™ system plate offers stable fixation, restores alignment and permits early mobilisation, thus promoting better functional recovery.[12–14] However, despite these potential advantages, the literature shows variability in clinical outcomes. Reported complications such as screw penetration, subacromial impingement and stiffness remain areas of concern.[15,16] Furthermore, many studies are retrospective, involve heterogeneous populations or lack standardised rehabilitation protocols.[17,18]
Thus, while locking plate fixation is a promising modality, there remains uncertainty regarding its optimal application in three-part and four-part fractures, particularly in resource-constrained settings and among diverse patient demographics. There is also limited prospective data specifically evaluating the Constant-Murley score as a functional endpoint in such cases.
This study hypothesises that the use of the PHILOS™ system plate in the surgical management of displaced three-part and four-part proximal humerus fractures results in good to excellent functional outcomes with minimal complications, provided that anatomical reduction and standardised rehabilitation are achieved.
PHILOS™ system plating is a well-recognised and widely adopted surgical technique for proximal humerus fractures, as highlighted by Thanasas et al. in their 2009 systematic review.[19] However, existing literature often includes heterogeneous fracture types and varied surgical protocols, limiting the applicability of results to complex fracture patterns. The present prospective study focuses exclusively on displaced three-part and four-part fractures, treated with a standardised surgical and rehabilitation protocol by a single orthopaedic team and provides context-specific outcome data from an Indian tertiary care centre.
The aim was to prospectively evaluate functional outcomes over 1 year, using the Constant-Murley scoring system at defined follow-up intervals and to correlate these outcomes with demographic, injury-related and procedural factors. Through this approach, the study sought to clarify the role of PHILOS™ system plating in contemporary orthopaedic practice and to provide data that may guide treatment planning, implant selection and patient counselling, particularly in the Indian context, where prospective studies of this nature remain limited.
Patients and Methods
This prospective observational study was conducted in a tertiary care teaching hospital between January 2021 and December 2023. Institutional Ethics Committee (IEC) clearance was obtained before commencement (IEC No: GMCKKD/IEC/2021/125) and informed written consent was obtained from all participants in their native language.
A total of 24 adult patients presenting with displaced three-part and four-part fractures of the proximal humerus were enrolled. This prospective observational study group, representing all consecutive eligible cases during the study period, has a sample size determined by feasibility rather than a priori calculation, in line with similar single-centre observational series.[14,20] A priori power analysis was not conducted due to the exploratory nature of this prospective study and the limited patient pool available during the study period.
Fracture classification was done using the Neer system[4] based on plain radiographs and computed tomography (CT) imaging where needed. All patients were admitted either through the outpatient department or the emergency trauma services.
Patients were eligible for inclusion if they were aged 18 years or older and had sustained a closed, displaced three-part or four-part proximal humerus fracture classified according to the Neer system. Only those who were medically fit for anaesthesia and surgery, provided informed written consent and agreed to adhere to the follow-up schedule were considered for enrolment.
Patients were excluded if they had pathological fractures, open injuries or associated fractures involving the ipsilateral humeral shaft or distal humerus. Individuals with pre-existing shoulder pathologies such as rotator cuff tears, those presenting with neurovascular deficits, active infections or who were unfit for surgery or anaesthesia were also not considered for the study.
Surgical Technique
All patients underwent ORIF using the PHILOS™ system plate under general or regional anaesthesia. ORIF using a PHILOS™ system plate was chosen as the treatment modality, in line with current orthopaedic practice guidelines and its wide acceptance in the literature as a standard surgical option for three-part and four-part proximal humerus fractures.[14,15,19,20]
The deltopectoral approach was employed in all cases. The plate was positioned 5–8 mm below the greater tuberosity and calcar screws were placed for inferomedial support when feasible.[10] Intraoperative reduction and implant positioning were confirmed with fluoroscopy.
Postoperatively, arm slings were applied and patients began pendulum and elbow range of motion (ROM) exercises on day one. Passive shoulder mobilisation was initiated after 2 weeks, followed by active mobilisation at 4 weeks, depending on radiological signs of stability.
Functional Outcome Assessment
The Constant-Murley score[21] was used as the primary tool to assess functional outcomes. It includes subjective and objective components, assessing pain, range of motion, strength and activities of daily living, scored out of 100. Patients were evaluated at 6 weeks, 3 months, 6 months and 12 months postoperatively. Clinical examination was supplemented with shoulder radiographs to assess union, implant position and complications such as malunion, nonunion, AVN or screw cut-out. Radiological union was confirmed in all cases but was not analysed as a primary endpoint.
Data Collection and Statistical Analysis
Baseline patient data, including age, sex, dominance of involved limb, fracture classification (Neer), ASA physical status classification, smoking status, presence of diabetes mellitus, hypertension, ischaemic heart disease and osteoporosis (based on preoperative dual-energy X-ray absorptiometry (DEXA) scan or clinical diagnosis) were recorded.
Data were recorded using a standardised proforma and later compiled into Microsoft Excel. Statistical analysis was performed using International Business Machines Corporation (IBM) statistical package for the social sciences (SPSS) Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY). Descriptive statistics (means and percentages) were used for demographic and categorical data. Repeated measures analysis of variance (ANOVA) was applied to evaluate changes in Constant scores over time. A P value <.05 was considered statistically significant. Post hoc power calculation was performed for the primary outcome measure. Subgroup analyses were conducted to compare Constant-Murley scores at 1 year between patients with and without selected comorbidities using independent t-tests.
Results
Baseline clinical characteristics and comorbidities are summarised in Table 1.
Baseline clinical characteristics and comorbidities of study participants (n = 24)
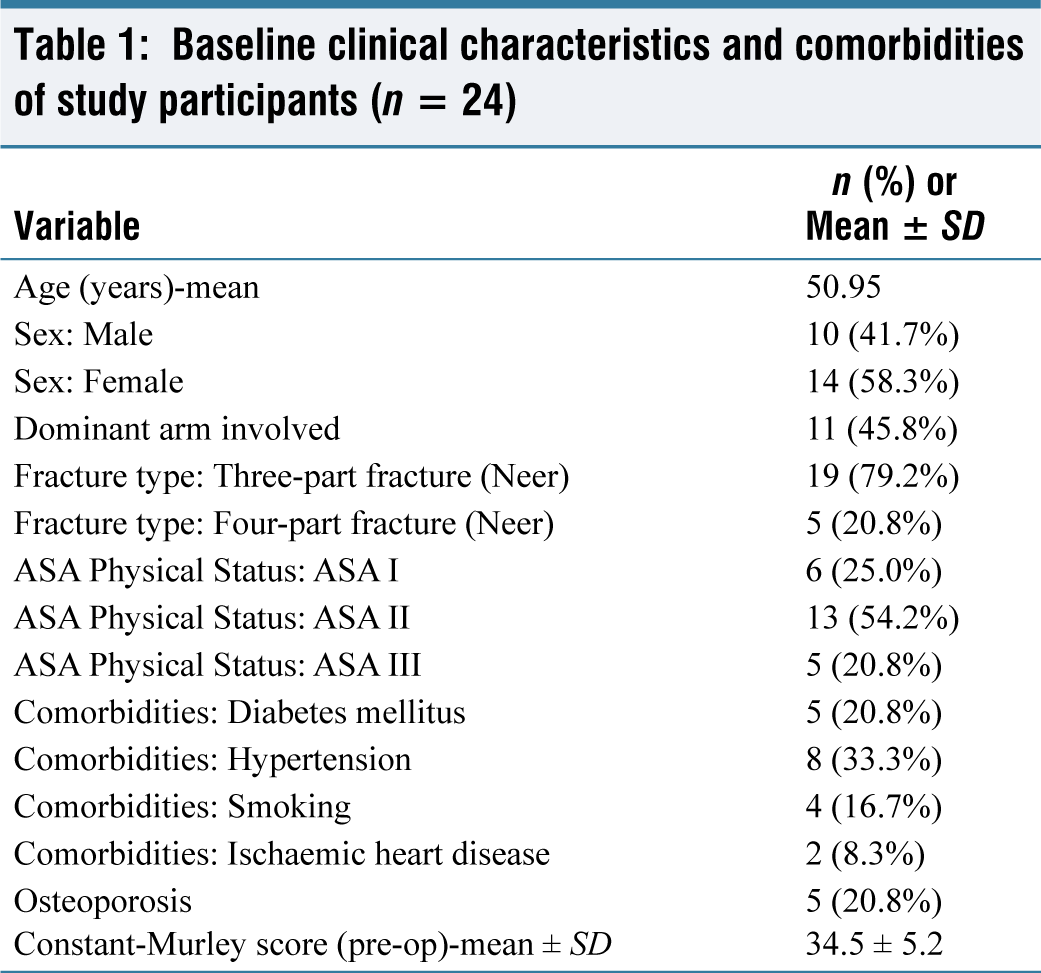
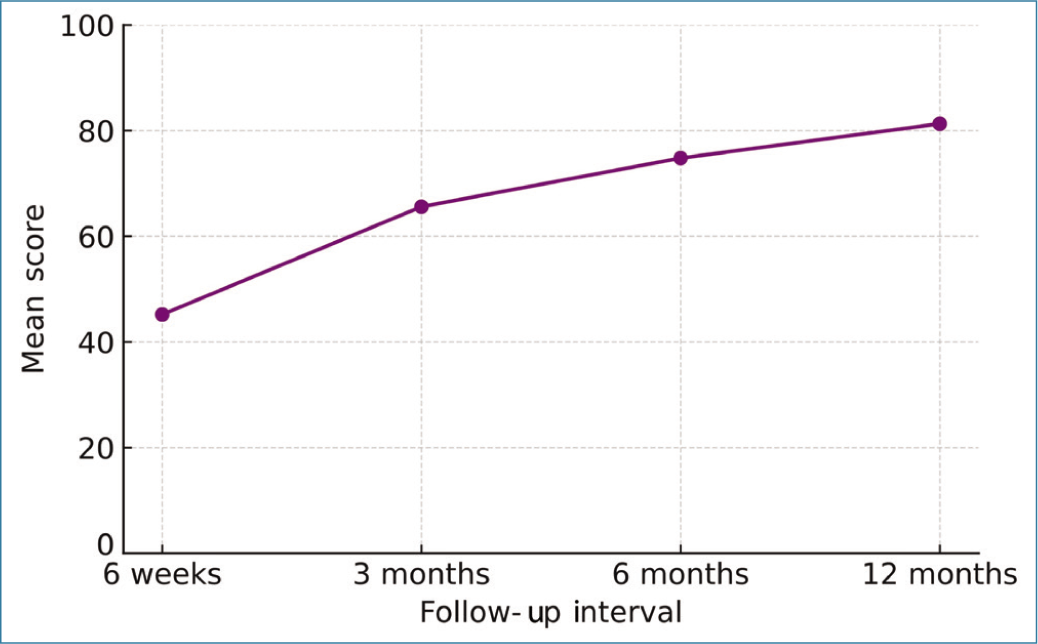
The most common mechanism of injury was RTA, accounting for 66.7% of cases, while 33.3% sustained injuries due to low-velocity falls. At final follow-up, all fractures had achieved radiological union. The mean time to union was 12.5 weeks (range 10–16 weeks). Functional outcomes, assessed using the Constant-Murley score, showed progressive improvement at each follow-up interval [Figure 1]. The mean scores were 45.2 at 6 weeks, 65.6 at 3 months, 74.8 at 6 months and 81.3 at 12 months, with the improvement being statistically significant (P < .001, repeated measures ANOVA).
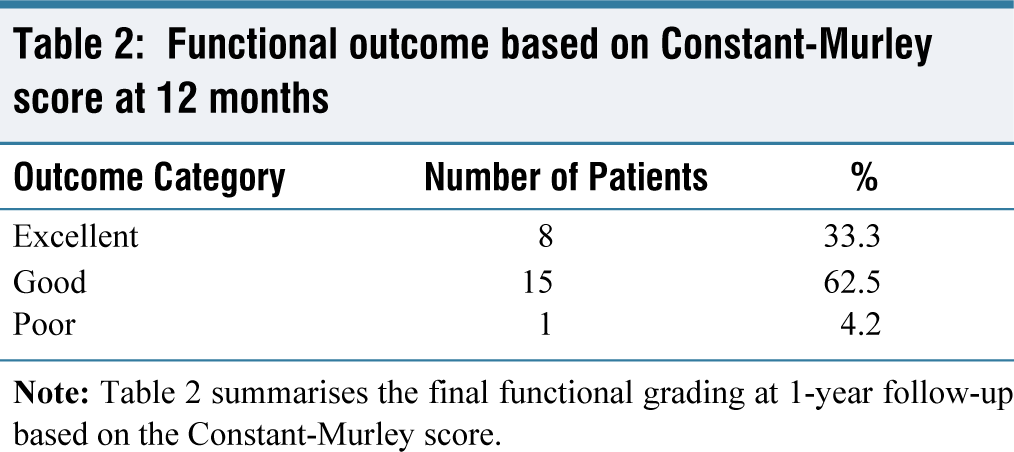
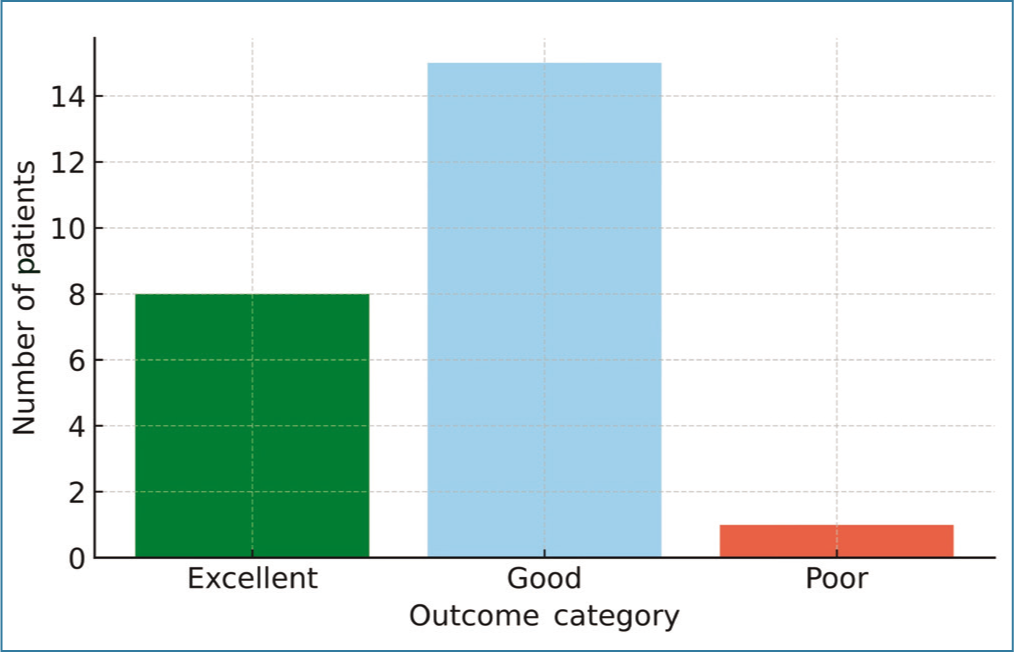
At the 1-year mark, functional outcomes were graded as excellent in eight patients (33.3%), good in 15 patients (62.5%) and poor in one patient (4.2%) based on Constant scores [Table 2, Figure 2]. The patient with a poor outcome had developed adhesive capsulitis due to poor adherence to the rehabilitation protocol. No cases of AVN, nonunion, implant failure or screw cut-out were observed.
Functional outcome based on Constant-Murley score at 12 months
When stratified by fracture type, patients with three-part fractures had a mean Constant score of 82.2 (SD ± 6.3), whereas those with four-part fractures had a mean score of 77.6 (SD ± 7.9), although this difference was not statistically significant (P = .19, independent samples t-test). Similarly, male patients had marginally higher mean scores (82.4 ± 5.7) compared to females (80.5 ± 7.2), without statistical significance (P = .37).
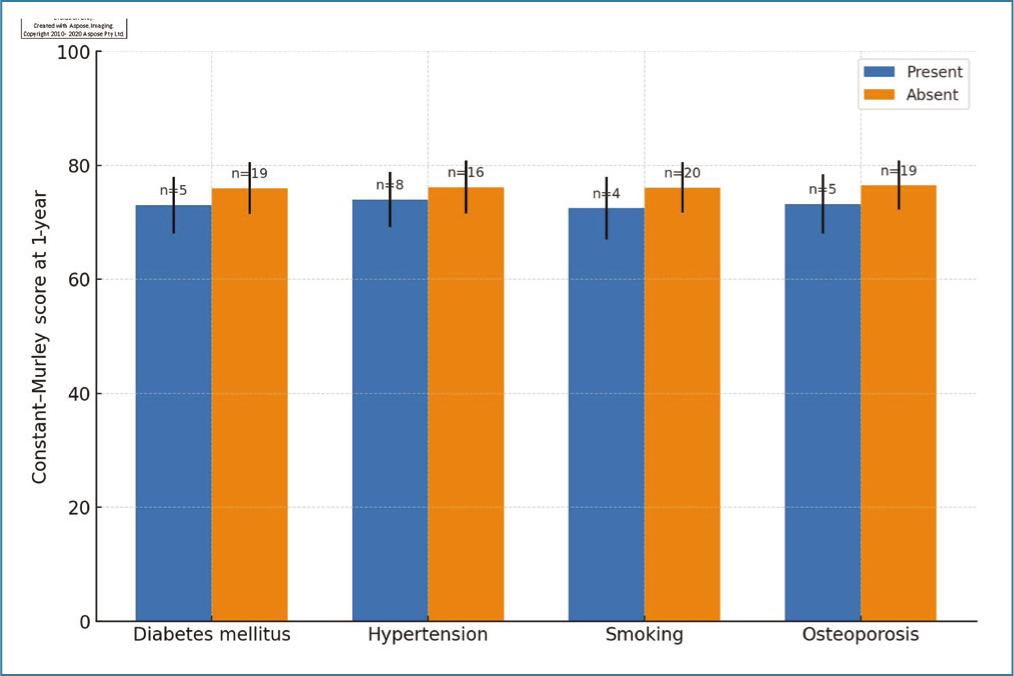
Subgroup analyses by comorbidity status are presented in Figure 3. Although mean Constant-Murley scores at 1 year tended to be lower in patients with comorbidities such as diabetes, smoking and osteoporosis, these differences did not reach statistical significance.
A post hoc analysis of the Constant score trend showed the greatest rate of improvement between 6 weeks and 3 months (∆mean = +20.4), suggesting that early rehabilitation contributed significantly to recovery.
One patient (4.2%) experienced stiffness and required prolonged physiotherapy. No superficial or deep infections, screw back-out or intra-articular penetration were documented. This low complication rate supports the biomechanical advantages of PHILOS™ system plating in complex fractures.
Overall, 95.8% of the patients achieved a good to excellent outcome at 1 year, underscoring the efficacy and reliability of this surgical method in both younger trauma victims and elderly osteoporotic individuals.
Discussion
Proximal humerus fractures represent a significant orthopaedic challenge, particularly when they involve three or four displaced fragments. These injuries can severely impair shoulder function, especially in the elderly, where osteopenia further complicates fixation and healing.[1] In this prospective study, the use of the PHILOS™ system plate in managing such fractures demonstrated encouraging outcomes, both in terms of fracture union and functional recovery. Our results substantiate the growing consensus in orthopaedic literature favouring locking plate fixation for complex proximal humerus fractures.[2–4]
While several treatment modalities exist for complex proximal humerus fractures, including conservative treatment, intramedullary nailing, hemiarthroplasty and reverse shoulder arthroplasty (RSA), the choice of intervention remains controversial, particularly in younger or middle-aged individuals with good bone stock.[5–7] The PHILOS™ system plate, designed for anatomical congruence and angular stability, offers a biomechanically robust solution. However, variations in patient demographics, fracture morphology, surgical technique and rehabilitation protocols across existing studies create ambiguity in outcomes.[8] This prospective analysis provides clarity in an Indian clinical context, involving a uniform surgical technique, structured postoperative rehabilitation and consistent outcome assessment using the validated Constant-Murley scoring system.[9]
The progression of Constant-Murley scores across the follow-up intervals shows 45.2 at 6 weeks to 81.3 at 12 months, which reflects a statistically and clinically significant improvement (P < .001). These findings align with those of Brunner et al.[13] who observed similar gains following PHILOS™ system fixation and Südkamp et al.[15] who noted mean final scores around 82 in their multicentric cohort.
The majority of patients in our study achieved excellent or good outcomes (95.8%). This is slightly superior to the success rates reported in some previous studies, such as by Kettler et al.[16] (88%) and Agrawal et al.[14] (91.2%). One plausible reason for this favourable result is the strict adherence to a standardised physiotherapy protocol and timely surgical intervention. Additionally, patients were operated on by a single experienced orthopaedic team, minimising technique variability.
When outcomes were stratified by fracture type, patients with three-part fractures showed a higher mean Constant score (82.2 ± 6.3) than those with four-part fractures (77.6 ± 7.9). Although this difference did not reach statistical significance (P = .19), it is clinically relevant and in line with biomechanical expectations, as four-part fractures often involve greater disruption of vascular supply to the humeral head and may necessitate more extensive soft tissue dissection.[22]
Similarly, the gender-based comparison revealed a marginally higher score in males than in females (82.4 vs. 80.5), without statistical significance (P = .37). These results are comparable to observations made by Agudelo et al.[10] who found fracture morphology and patient compliance with rehabilitation to be more decisive than demographic variables in determining outcomes.
In contrast to the relatively high complication rates reported in earlier studies, such as screw penetration (16%–28%),[23] AVN (4%–16%)[24] and implant-related issues (up to 10%),[25] in our study reported a remarkably low complication profile. There were no cases of infection, implant loosening or hardware failure. Only one patient developed adhesive capsulitis, attributed to poor physiotherapy compliance.
This low complication rate may reflect meticulous surgical technique, careful intraoperative reduction and screw placement under fluoroscopic guidance and stringent postoperative supervision. Calcar screw usage was prioritised where anatomically feasible, which has been proven to significantly enhance fixation stability and prevent varus collapse in osteoporotic bone.[26]
The statistical robustness of our findings enhances their reliability. Repeated measures ANOVA confirmed a highly significant improvement in Constant-Murley scores over time (P < .001). Although subgroup analyses did not reach statistical significance, this may be attributed to the small sample size, particularly in the four-part fracture group. Nevertheless, the narrow standard deviations across assessments indicate consistency and precision in outcome measurement.
The post hoc analysis revealing the most substantial functional improvement between 6 weeks and 3 months (Δmean = +20.4) emphasises the critical importance of early mobilisation, a factor echoed in other prospective studies.[27]
Compared to hemiarthroplasty and RSA, which are often preferred for four-part fractures in the elderly, locking plate fixation offers the advantage of anatomical preservation and potential for superior long-term function, especially in compliant, active patients.[28] While RSA has gained popularity, especially in Western populations, it entails higher costs, longer operative times and is associated with complications such as scapular notching and limited rotational power.[28]
In younger populations, locking plates such as the PHILOS™ system are particularly advantageous as they maintain native shoulder biomechanics. Our study supports this approach, as the mean patient age was relatively low (50.95 years) and none required conversion to arthroplasty.
This study stands apart from existing literature in several important respects. First, it was designed as a purely prospective cohort study, thereby eliminating recall and selection biases inherent in retrospective analyses.[13] Second, all surgical procedures were performed using a consistent protocol by a single orthopaedic unit, ensuring uniformity in technique and reducing variability in outcomes.[15] Third, functional recovery was assessed exclusively using the Constant-Murley scoring system at clearly defined intervals, offering a focused and validated measure of shoulder performance.[19] Additionally, the study represents one of the few prospective investigations from a tertiary care centre in India, thus contributing valuable insights into outcomes within a regional healthcare context where patient compliance and follow-up practices may differ from Western populations.[14] This combination of methodological rigour and contextual relevance enhances the reliability and applicability of the findings.
Despite its strengths, this study has certain limitations. First, the sample size was relatively small, which may limit the statistical power to detect subtle differences, particularly between fracture subtypes. Second, the follow-up period of 12 months, while adequate for early functional outcomes, may not capture late complications such as AVN or post-traumatic arthritis. Third, all procedures were conducted in a single institution by one surgical team, which may affect the generalisability of the results. Additionally, the study lacked a control or comparative group treated by alternative methods, precluding direct evaluation of relative efficacy. Advanced imaging and objective radiological scoring systems were not employed, which might have provided deeper insights into the quality of fracture reduction and healing. This study also did not include radiological parameters as a primary endpoint, focusing solely on functional outcomes. Additionally, the relatively small sample size and lack of a priori power calculation may limit generalisability.
Conclusion
In this single-centre observational series of 24 consecutive patients with complex three-part and four-part proximal humeral fractures, PHILOS™ system plate fixation achieved satisfactory 1-year functional outcomes, consistent with earlier reports. Unlike most earlier studies, our analysis focused solely on these complex fracture types, used functional recovery as the primary endpoint and incorporated detailed baseline data, including comorbidities, ASA grade and osteoporosis status, to explore their potential influence on outcome. These findings provide region-specific, real-world evidence to guide surgical decision-making. However, the small cohort, absence of a comparator and non-randomised design warrant confirmation through larger, well-designed comparative or randomised trials.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval has obtained. It is being already included in the patients and method section as a sentence “Institutional Ethics Committee (IEC) clearance was obtained prior to commencement (IEC No: GMCKKD/IEC/2021/125)”.
Informed consent
Informed written consent was obtained from all participants in their native language.
Credit author statement
All authors have read and approved the final manuscript and meet the criteria for authorship as defined by the International Committee of Medical Journal Editors (ICMJE). No part of this manuscript has been published or is under consideration for publication elsewhere.
Data availability statement
The datasets generated and analysed during the current study are not publicly available due to patient confidentiality and privacy agreements under which the study was conducted with approval from the Institutional Ethics Committee. Anonymised data may be made available from the corresponding author upon reasonable request, subject to permission from the institutional data governance committee.
Use of artificial intelligence
We confirm that artificial intelligence (AI) tools, including ChatGPT (OpenAI), were used to assist with language refinement, grammar correction and formatting of the manuscript. However, all clinical content, interpretation of data, analysis and final conclusions were conceived, validated and approved entirely by the authors. The authors take full responsibility for the integrity, originality and accuracy of the scientific content.
No AI tools were used for data analysis, data generation or in the writing of patient-related clinical observations or results.