
Abstract
Background:
Thyroid dysfunction is one of the endocrine dysfunctions that is known to be linked to Type 2 diabetes mellitus. The goal of the current study was to compare the prevalence of thyroid dysfunctions in individuals with Type 2 diabetes mellitus to that of a healthy control group.
Materials and Methods:
A case-control study was conducted over 1 year, at a tertiary care hospital, involving 216 patients (105 diabetic subjects and 111 non-diabetic individuals). Age, gender, comorbidities, duration of diabetes, TSH, fasting blood sugar (FBS), postprandial blood sugar and Glycated Hemoglobin (HbA1C) levels were collected from electronic health records. Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) software, with the Karl Pearson or Spearman rank-order correlation test to assess the relationship between TSH and HbA1C. A P value of less than .05 was considered statistically significant.
Results:
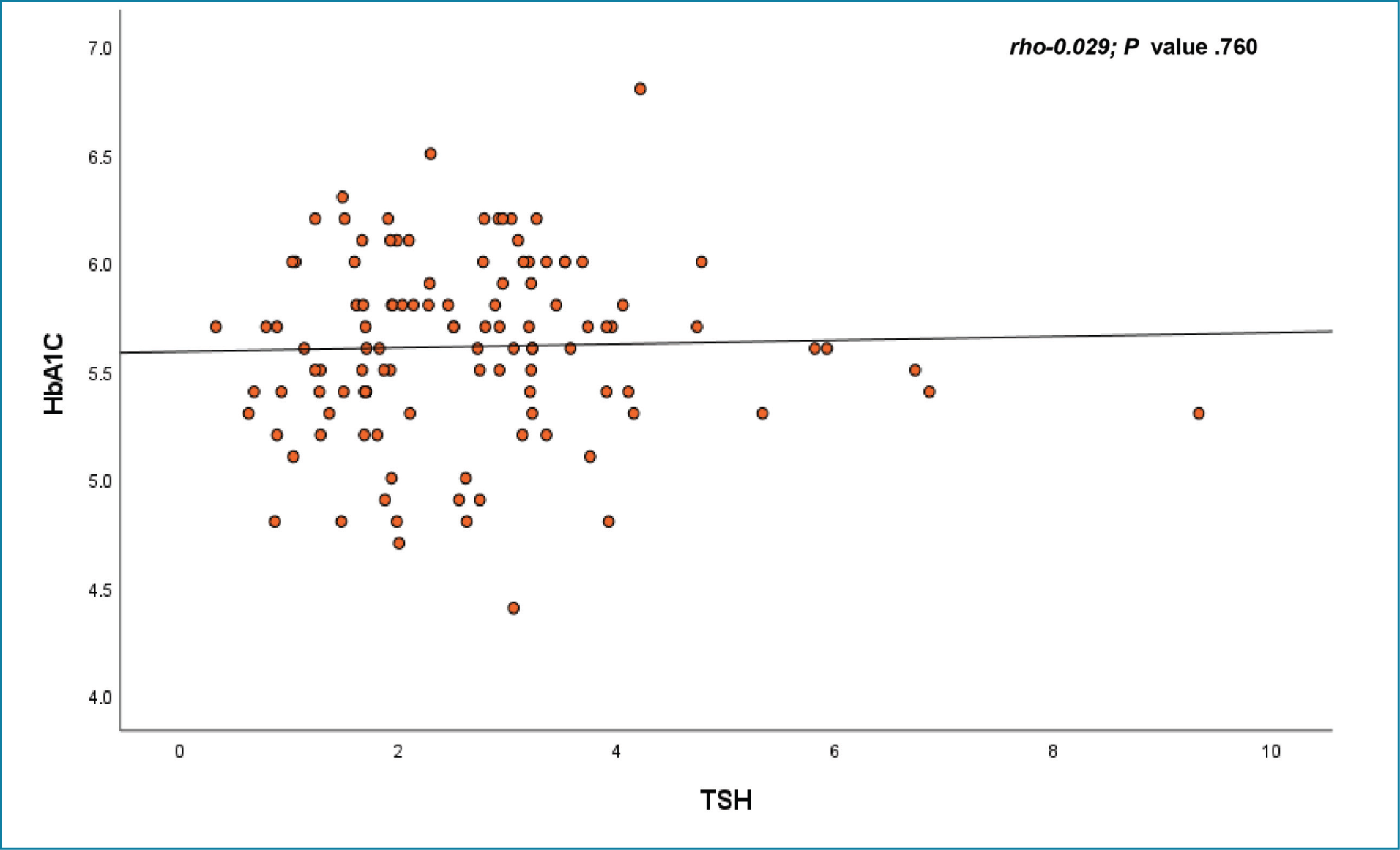
The FBS (153.79 ± 60.99 mg/dL) and HbA1C (7.76 ± 1.49%) of the diabetes group were substantially greater than those of the healthy controls (FBS: 97.94 ± 11.28 mg/dL; HbA1C: 5.61 ± 0.42%). Nonetheless, there was no discernible change in TSH levels between the control group (2.63 ± 1.41 mU/L) and the diabetes group (2.59 ± 1.82 mU/L). However, no significant association was found between HbA1C and TSH levels by correlation analysis in either the diabetic (Rho = 0.009; P = .930) or non-diabetic (Rho = 0.029; P = .760) groups.
Conclusion:
These findings conclude that there is no correlation between TSH and HbA1C levels in either groups.
Introduction
A major global health issue that affects many people is diabetes mellitus. Chronic hyperglycemia and disruptions in protein, lipid and carbohydrate metabolism due to absolute or relative deficits in insulin secretion are the hallmarks of this group of metabolic diseases.[1] The International Diabetes Federation projects that by 2045, there will be 700.2 million diabetics worldwide, up from 463 million in 2019.[2] Thyroid dysfunction is the second most prevalent endocrine condition after diabetes mellitus.[3] Thyroid abnormalities are claimed to affect 6.6%–13.4% of the general population worldwide, but the frequency is higher in the diabetic population, ranging from 10% to 24%.[4] Both increased glycogenolysis and increased hepatic glucose production, which are symptoms of thyrotoxicosis, cause glucose intolerance, which exacerbates elevated blood glucose levels in diabetics.[3] By reducing glucose absorption, hypothyroidism lowers hepatic glucose output and, consequently, insulin production, which accounts for the decline in peripheral glucose utilisation and insulin resistance.[4] Conversely, poorly managed diabetes can impact thyroid function because unchecked hyperglycemia changes plasma T3 and T4 levels.[4] It is hypothesised that individuals with diabetes have a disproportionately higher prevalence of thyroid dysfunction than the overall population.[5]
Materials and Methods
This study was conducted over 1 year at a tertiary care hospital in Chennai. It was a retrospective case-control study involving 216 patients, comprising 105 diabetic subjects and 111 non-diabetic individuals.
Inclusion criteria for cases:
All patients with underlying Type 2 diabetes mellitus. Age more than 18 years.
Inclusion criteria for the control group:
Age and sex-matched normal healthy individuals with FBS < 126 mg/dl and Glycated Hemoglobin (HbA1C) < 6.5 %.
Exclusion criteria:
Patient less than or equal to 18 years of age Those with a history of thyroid disease Those who did not give consent to the study On drugs that may affect thyroid function, for example, steroids, amiodarone and phenytoin Pregnancy Patient who underwent radiotherapy (head and neck) Drug-induced diabetes Type 1 diabetes mellitus
Study Protocol
Demographic, clinical and laboratory data will be obtained from electronic health records using a standardised data collection form. The data to be collected include age, gender, duration of Type 2 diabetes mellitus, current medications, TSH, fasting blood sugar (FBS), postprandial blood sugar and HbA1C levels.
Statistical Analysis
Summary statistics were presented as mean ± SD and frequency (percentage) for non-skewed data and as median interquartile range (IQR) for skewed data. Student’s t-test or Mann-Whitney U test was used to determine the significant changes between diabetic and non-diabetic participants. Chi-square or Fisher’s exact test was used to determine the association between 2 independent factors. The Spearman rank-order correlation test was used to determine the linear relationship between HbA1C and TSH. A P value <.05 was considered statistically significant. All the statistical analyses were carried out by using Statistical Package for the Social Sciences (SPSS) (IBM, 28.0).
Results
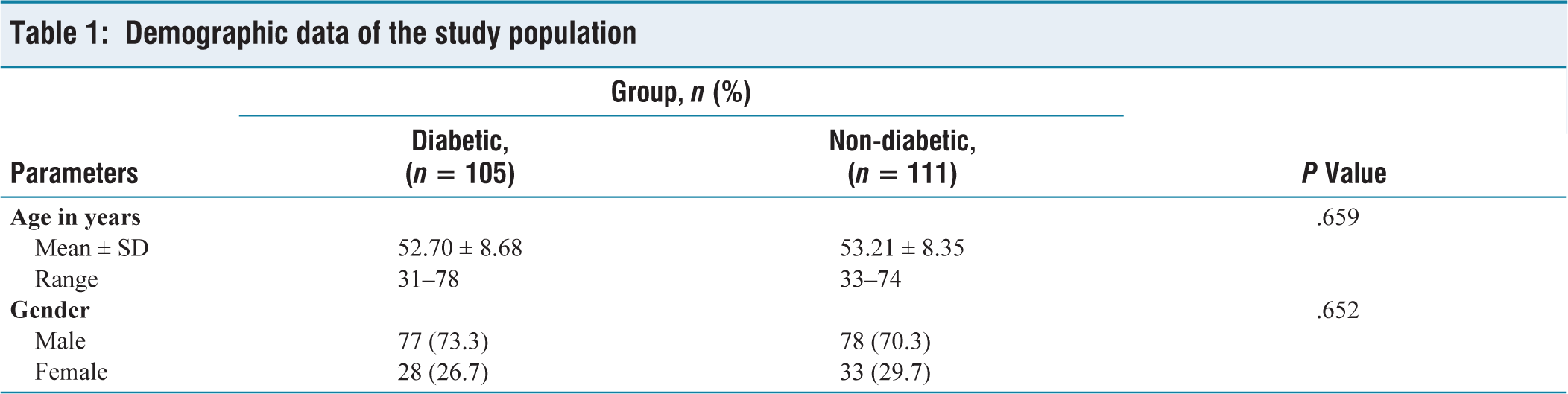
The mean age of the diabetic population was 52.70 ± 8.68 years, whereas the mean age of the non-diabetic population was 53.21 ± 8.35 years. As shown in [Table 1], the diabetic and non-diabetic populations comprised 73.3% and 70.3% males, respectively, while 26.7% and 29.7% were females, respectively.
Demographic data of the study population
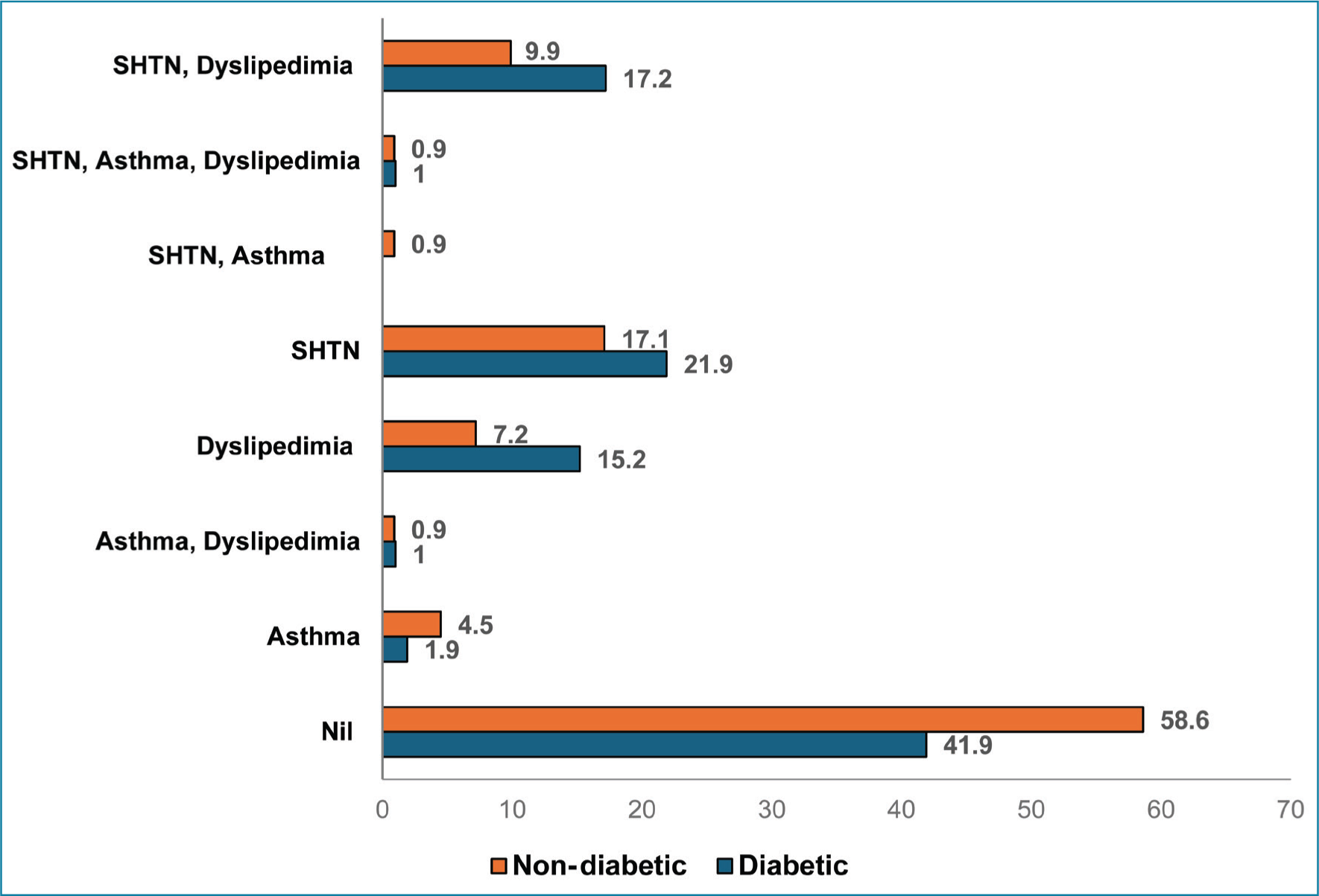
Among non-diabetic individuals, 58.6% had no comorbid conditions, compared with 41.9% of diabetic individuals. Systemic hypertension was present in 21.9% of individuals with diabetes, compared with 17.1% of non-diabetics. Dyslipidaemia was present in 15.2% of individuals with diabetes, compared with 7.2% of those without diabetes [Figure 1]. Both systemic hypertension and dyslipidaemia were present in 17.2% of individuals with diabetes, compared with 9.9% of those without diabetes [Figure 1]. Both asthma and dyslipidaemia were present in 1% of individuals with diabetes, compared with 0.9% of those without diabetes [Figure 1]. Asthma is more common in non-diabetics (4.5%) than in individuals with diabetes (1.9%) [Figure 1]. Systemic hypertension, asthma and dyslipidemia (triple comorbidity) are rare in both groups [Figure 1].
Illustrating the distribution of comorbidities among the study population
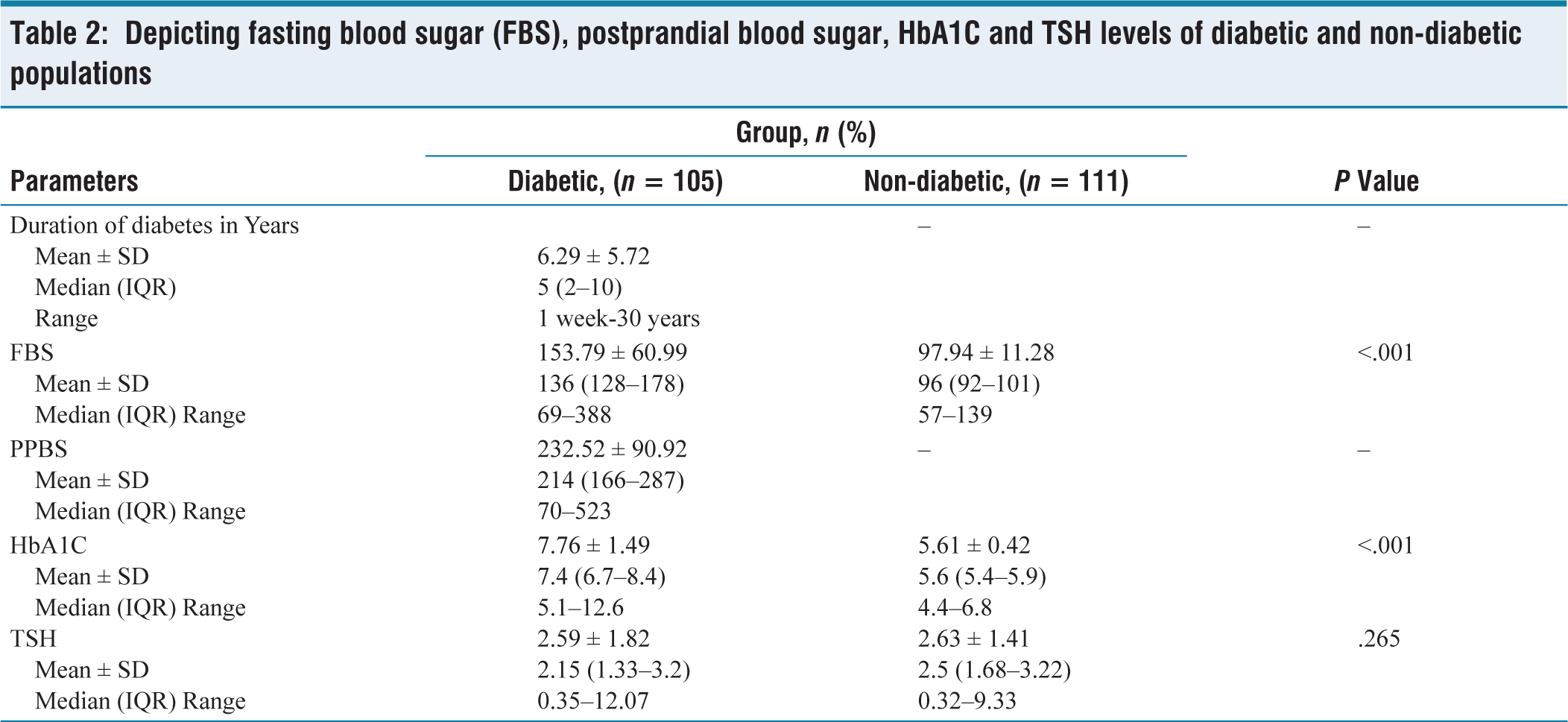
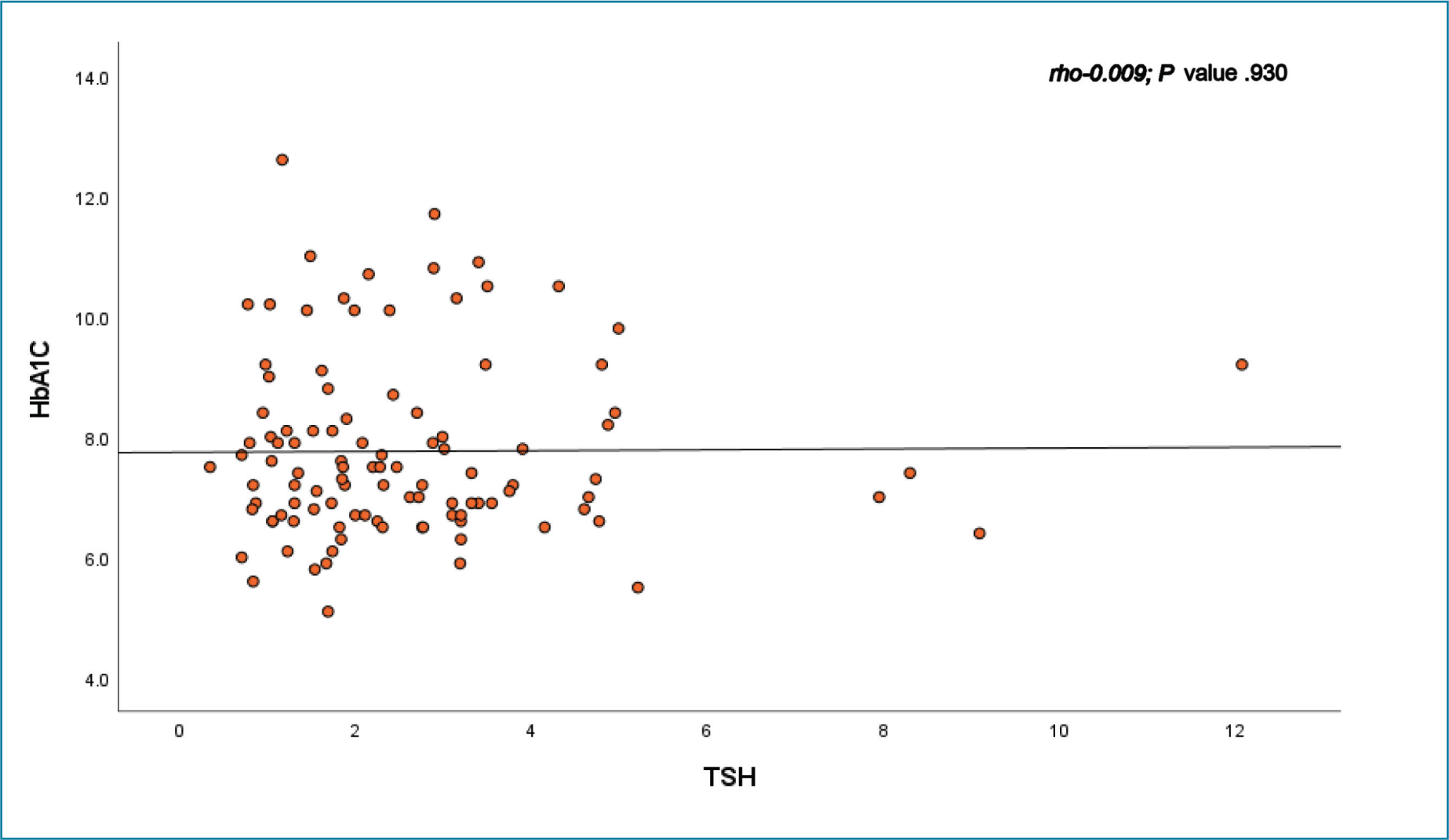
The median duration of diabetes in the case group was 5 years (2–10). The median FBS, postprandial blood sugar and HbA1C level in the diabetic population were 136.0 mg/dL (128–178 mg/dL), 214.0 mg/dL (166–287 mg/dL) and 7.4% (6.7%–8.4%), respectively [Table 2]. The median TSH level in the diabetic population was 2.15 (1.33–3.2) [Table 2]. The median FBS, HbA1C and TSH levels in the non-diabetic population were 96.0 mg/dL (92–101 mg/dl), 5.6% (5.4%–5.9%) and 2.5 (1.68–3.22), respectively. Rho = 0.009 represents no significant correlation between HbA1C and TSH levels in the diabetic group, with a P value of .930 (>0.05, statistically not significant) [Table 2]. Rho = 0.029 represents no significant correlation between HbA1C and TSH levels in the non-diabetic group, with a P value of .760 (>0.05, statistically not significant) [Figures 2 and 3].
Depicting fasting blood sugar (FBS), postprandial blood sugar, HbA1C and TSH levels of diabetic and non-diabetic populations
Scatter plot showing the relationship between TSH and HbA1C levels in the diabetic population
Scatter plot showing the relationship between TSH and HbA1C levels in the non-diabetic population
Discussion
In our study, a total of 216 subjects were enrolled, comprising 105 individuals with diabetes and 111 without diabetes. There was no correlation between TSH and HbA1C in both diabetic and non-diabetic populations. Iwakura et al. in their study involving 200 diabetic patients and 225 non-diabetic patients, found no difference in the prevalence of thyroid dysfunction among diabetic and non-diabetic subjects.[5]
Vamshidhar et al. in their study found that out of 50 diabetic patients, 16% had thyroid disorders.[6] Rahman et al. in their study involving 120 diabetic patients and that the mean TSH level was higher in poorly controlled diabetes.[2] A positive correlation between TSH and HbA1C was also found.[2] Malek et al. in their case-control study involving 50 diabetic and 50 non-diabetic subjects, found that 31% of diabetic patients showed thyroid disorders.[1] Elgazar et al. in their study involving 200 diabetic and 200 non-diabetic patients, determined that there were significantly higher levels of TSH and T3 in diabetic subjects compared with the non-diabetic individuals. High TSH levels were positively correlated with HbA1C and duration of diabetes.[3]
The higher rate of thyroid screening among diabetic patients in our institute compared to the control group, along with the exclusion of previously diagnosed thyroid disorders, may have caused a bias, potentially underestimating the true prevalence of thyroid dysfunction in patients with diabetes.[5]
Conclusion
The relationship between HbA1C and TSH levels in patients with Type 2 diabetes remains uncertain, as studies have shown varied results. Differences in the design of the study, characteristics of the subjects and their comorbidities and duration and control of diabetes may contribute to these inconsistent results.
Footnotes
Acknowledgements
To the Research Department, Apollo Main Hospital, Chennai, Tamil Nadu.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Approval was obtained from the Institutional Ethical Committee on 24 March 2025.
Informed consent
Informed consent has not been obtained from the patients as it was a retrospective study.
Credit author statement
RP participated in conceptualisation, methodology, data collection, data analysis, literature search and manuscript preparation.
AA was involved in conceptualisation, literature search, validation, supervision and manuscript revision.
All the authors have reviewed and approved the manuscript.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author upon request.
Use of artificial intelligence
No generative Artificial Intelligence (AI) tools were used in the writing, editing, data collection, statistical analysis, or figure/table preparation for this article. The entire work was conducted by the authors.