
Abstract
Background:
Chronic pain significantly impairs the quality of life in older adults, with current treatments often being inadequate or accompanied by side effects. Virtual reality (VR) is emerging as a promising non-pharmacological intervention for chronic pain management.
Objective:
To evaluate the effectiveness, feasibility, and acceptability of VR interventions for managing chronic pain in older adults.
Methods:
A systematic review was conducted using databases including PubMed, Cochrane CENTRAL, Scopus, and EBSCOhost. Inclusion criteria were studies focusing on adults aged ≥60 years, employing VR for chronic pain management, and reporting quantitative outcomes. Randomised Controlled Trials (RCTs) were primarily included. Critical appraisal of methodological quality was performed using the Cochrane Risk of Bias (ROB) 2 tool.
Results:
Three studies, with a total of 239 participants, met the inclusion criteria. VR interventions ranged from CBT-integrated programs to nature-based guided meditations. One study demonstrated significant reductions in pain intensity for chronic low back pain, while others highlighted increased adherence to exercise and a reduction in anxiety. However, technical challenges, such as cybersickness and hardware malfunctions, affected the feasibility. Acceptability and user satisfaction were generally high, though usability issues were noted.
Conclusion:
VR interventions show potential as effective tools for managing chronic pain in older adults, enhancing adherence and providing non-pharmacological relief. Nonetheless, limitations include small sample sizes, technical barriers, and variable study quality. Future research should focus on improved methodological rigour, technological robustness, and long-term evaluations to validate the utility of VR for chronic pain management.
Keywords
Introduction
Chronic pain is a pervasive and debilitating condition that significantly affects the lives of older adults worldwide. Defined as persistent pain lasting three months or longer, chronic pain in this population is associated with reduced physical functioning, diminished quality of life, and increased reliance on healthcare services.[1–3] Chronic pain affects 1.9 billion people globally, with tension-type headaches, low back, and neck pain as leading causes of disability.[4] The prevalence of chronic pain is expected to rise with the ageing global population, thereby intensifying its impact on individuals, families, and healthcare systems.[1,5] Current pain management strategies for older adults predominantly include pharmacological treatments, such as nonsteroidal anti-inflammatory drugs (NSAIDs) and opioids, alongside non-pharmacological approaches like physical therapy and cognitive-behavioural therapy (CBT).[6,7] However, these conventional methods often present significant limitations. Pharmacological treatments carry the risk of adverse effects, including gastrointestinal issues, cardiovascular problems, and the potential for dependency, particularly concerning opioid use.[7] Non-pharmacological interventions, while beneficial, may require sustained participation and adherence, which can be challenging for older adults due to mobility issues, cognitive impairments, and limited access to specialised care.
Virtual reality (VR) has recently gained attention as a non-pharmacological intervention for chronic pain management.[8] By creating immersive environments, VR can distract attention from pain, promote relaxation, and support therapeutic movement. Its analgesic mechanisms include cognitive distraction and interactive engagement, which can enhance adherence to rehabilitation.[9,10] VR platforms may also integrate cognitive-behavioural and mindfulness-based components, offering a multidimensional approach to pain that addresses both somatic and psychological domains. Numerous studies have demonstrated VR’s potential in reducing pain and improving function across diverse populations.[11–15] However, research specifically focused on older adults remains limited. This group, potentially well-suited to benefit from tailored VR interventions, is underrepresented in the literature. Methodological heterogeneity across existing studies, including variability in interventions, outcome measures, and study designs, complicates the interpretation of overall efficacy. Additionally, technical barriers such as cybersickness and poor usability limit accessibility for older users. This systematic review compiles available evidence on the effectiveness of VR interventions for chronic pain management in older adults.
Methodology
A comprehensive literature search was conducted across PubMed, Cochrane CENTRAL, Scopus, and EBSCOhost (including MEDLINE, CINAHL, and PsycINFO) up to 16 November 2024. Search strategies were customised to each database’s syntax and controlled vocabulary to maximise the retrieval of relevant studies. The review has been officially registered with PROSPERO under the identification number CRD420251053610.[16]
PubMed Search Strategy
(‘Chronic Pain’[MeSH] OR ‘Pain Management’[MeSH] OR ‘Chronic Pain’ OR ‘Pain Management’ OR ‘persistent pain’) AND (‘Virtual Reality Exposure Therapy’[MeSH] OR ‘Virtual Reality’[MeSH] OR ‘VR intervention’ OR ‘VR therapy’ OR ‘VR-based intervention’ OR ‘Immersive VR’) AND (‘Aged’[MeSH] OR ‘Older Adults’ OR ‘Elderly’ OR ‘Geriatric Population’ OR ‘Seniors’)
Cochrane CENTRAL Search Strategy
(chronic pain OR ‘pain management’ OR ‘persistent pain’) AND (‘virtual reality exposure therapy’ OR ‘virtual reality’ OR ‘VR intervention’ OR ‘VR therapy’ OR ‘VR-based intervention’ OR ‘immersive VR’) AND (aged OR ‘older adults’ OR elderly OR ‘geriatric population’ OR seniors)
Scopus Search Strategy
(TITLE-ABS-KEY(‘chronic pain’) OR TITLE-ABS-KEY(‘pain management’) OR TITLE-ABS-KEY(‘persistent pain’)) AND (TITLE-ABS-KEY(‘virtual reality exposure therapy’) OR TITLE-ABS-KEY(‘virtual reality’) OR TITLE-ABS-KEY(‘VR intervention’) OR TITLE-ABS-KEY(‘VR therapy’) OR TITLE-ABS-KEY(‘VR-based intervention’) OR TITLE-ABS-KEY(‘immersive VR’)) AND (TITLE-ABS-KEY(‘aged’) OR TITLE-ABS-KEY(‘older adults’) OR TITLE-ABS-KEY(‘elderly’) OR TITLE-ABS-KEY(‘geriatric population’) OR TITLE-ABS-KEY(‘seniors’))
EBSCOhost Search Strategy
((‘Chronic Pain’ OR ‘Pain Management’ OR ‘persistent pain’) AND (‘Virtual Reality Exposure Therapy’ OR ‘Virtual Reality’ OR ‘VR intervention’ OR ‘VR therapy’ OR ‘VR-based intervention’ OR ‘Immersive VR’) AND (‘Aged’ OR ‘Older Adults’ OR ‘Elderly’ OR ‘Geriatric Population’ OR ‘Seniors’))
CADIMA software was used to import and manage the identified records, with duplicates being removed prior to screening.[17,18]
Eligibility Criteria
Inclusion criteria required that studies focus on older adults aged 60 years or above, diagnosed with chronic pain conditions, and evaluate VR interventions specifically aimed at managing chronic pain. Studies needed to include a comparator, which could be any control condition, including standard care, placebo VR, or other non-VR interventions. Eligible studies must report quantitative outcomes related to pain intensity, pain-related interference, adherence to intervention, acceptability, feasibility, or user satisfaction. Only randomised controlled trials (RCTs), including pilot and feasibility trials, were considered for inclusion.
The exclusion criteria encompassed studies involving participants younger than 60 years, those assessing non-VR interventions or interventions not focused on chronic pain management, and studies on acute pain conditions. Observational studies, case reports, reviews, and qualitative studies without quantitative effectiveness data were excluded. Additionally, studies not published in English were not considered eligible for inclusion.
Study Selection
Following the search, all identified records were imported into CADIMA for duplicate removal and management. Subsequently, two independent reviewers screened the titles and abstracts against the defined inclusion and exclusion criteria. Full-text articles were retrieved for studies considered potentially eligible based on the title and abstract screening. The same two reviewers then assessed these full-text articles for final inclusion. Any discrepancies between reviewers were resolved through discussion and by involving a third reviewer when consensus could not be reached.
Data Extraction
Two independent reviewers performed data extraction using a standardised form to ensure consistency. Extracted data included study and participant characteristics, intervention details (VR type, hardware/software, duration, frequency, training), and control conditions. Outcome measures, statistical methods, missing data handling, and confounder adjustments were documented. Discrepancies were resolved through discussion and consultation with a third reviewer.
Critical Appraisal
The methodological quality of included studies. The Cochrane ROB 2 tool was used in this review to assess the risk of bias across five domains: the process of randomisation, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results. Two reviewers evaluated these assessments independently, and disagreements were resolved by consulting a third reviewer. A general risk of bias rating for each included study was determined through an assessment of all individual domains.
Data Synthesis
Given the heterogeneity in interventions, populations, and outcome measures, a qualitative synthesis was undertaken. Findings were organised by primary outcomes: pain intensity reduction, feasibility, acceptability, and user satisfaction. Where possible, cross-study comparisons highlighted shared patterns and divergences. Qualitative data enriched the interpretation, offering a comprehensive view of VR’s effectiveness and feasibility in managing chronic pain in older adults. Owing to the limited number of studies and variability in design and outcomes, a narrative synthesis was used to emphasise key findings, methodological strengths, and study limitations.
Data Analysis
The data analysis aimed to assess the effectiveness, feasibility, and acceptability of VR interventions for chronic pain management in older adults. A narrative approach was used to synthesise the extracted data, highlighting the central findings of each study, as well as their methodological strengths and weaknesses.
Results
Study Selection
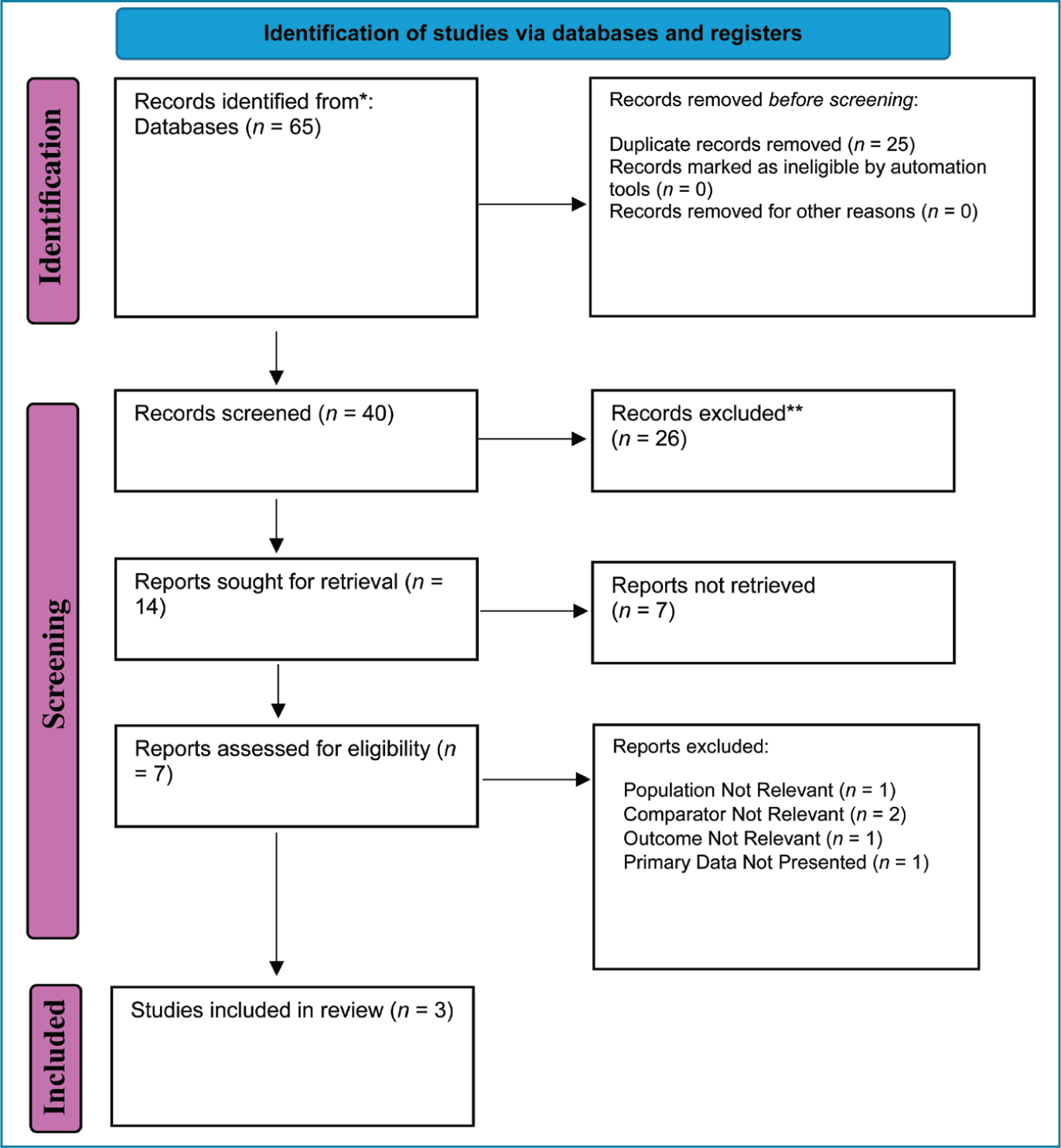
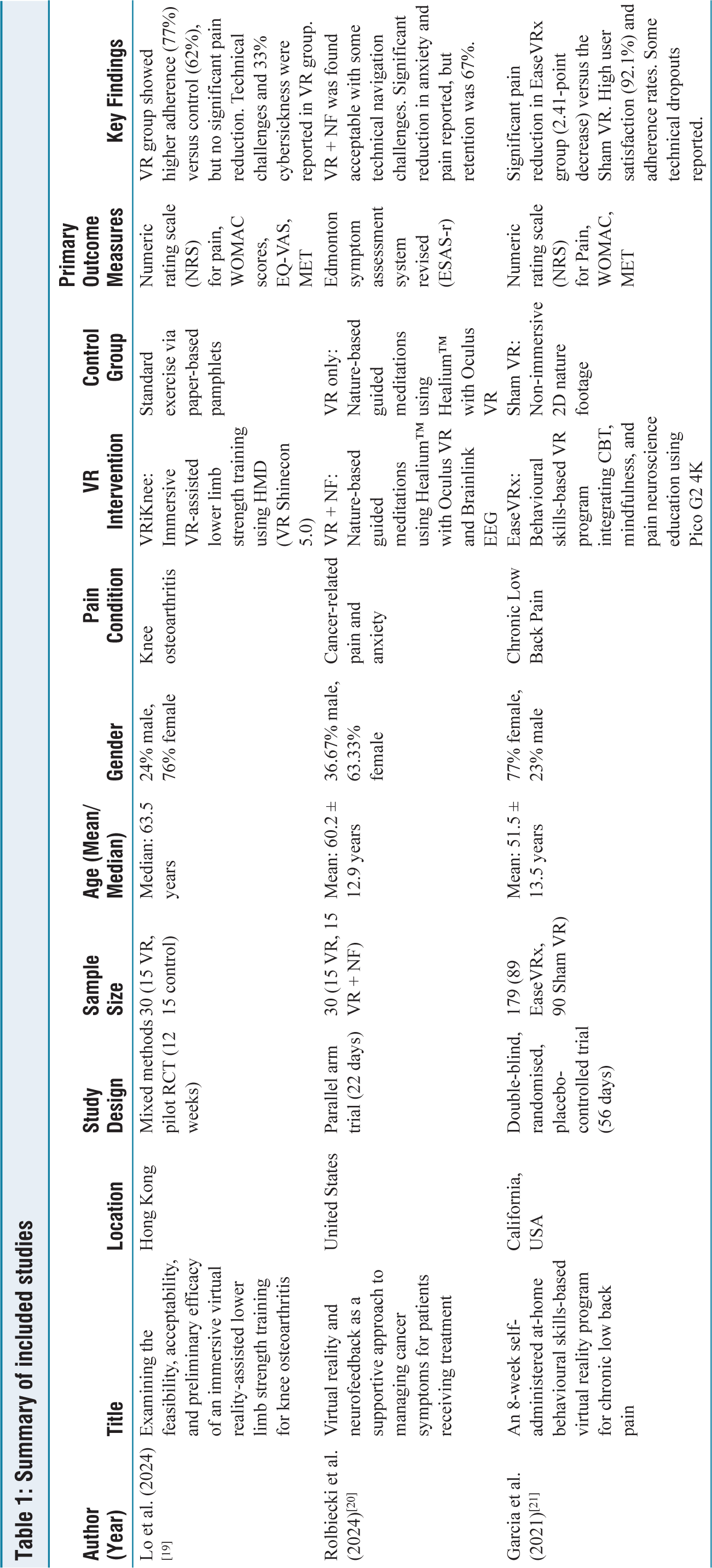
The study selection process is outlined in the PRISMA flow diagram [Figure 1]. A total of 65 records were identified through database searches, with no additional records from other sources. After removing duplicates, 40 records were screened by title and abstract, resulting in the exclusion of 26 records. Fourteen full-text articles were assessed for eligibility, of which 11 were excluded. Ultimately, three studies met all inclusion criteria and were included in the systematic review. Their key characteristics, interventions, outcomes, and effectiveness are detailed in Table 1. The methodological quality, appraised using the Cochrane Risk of Bias (ROB) 2 tool, is presented in Table 2. The included studies involved a combined total of 239 participants, aged 51.5–63.5 years, with predominantly female samples (63%-76%). Geographically, the studies were conducted in Hong Kong and the United States. Each study examined a distinct chronic pain condition: knee osteoarthritis, cancer-related pain, and chronic low back pain.
PRISMA flow diagram
Summary of included studies
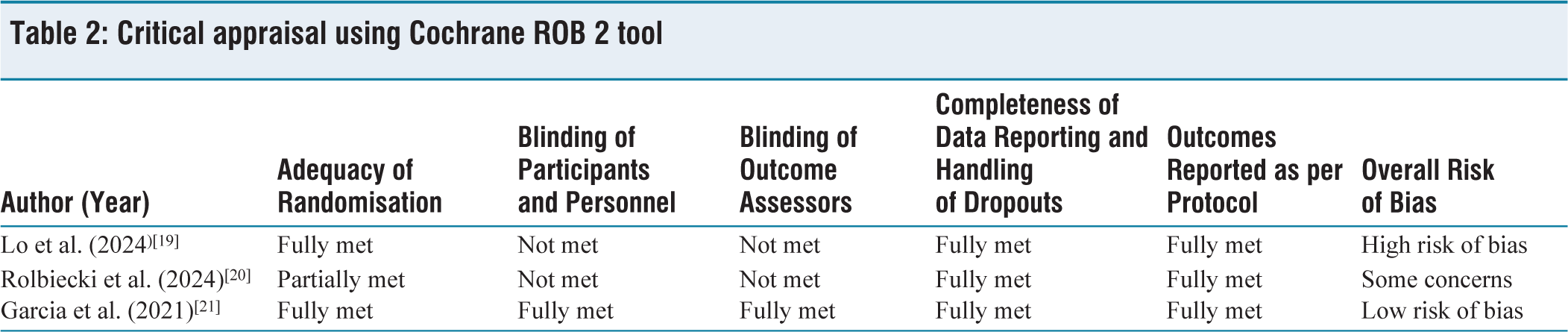
Critical appraisal using Cochrane ROB 2 tool
VR Interventions and Control Conditions
The VR interventions employed in these studies varied in both design and focus. Lo et al. developed an immersive VR-assisted lower limb strength training program called VRiKnee, aimed at patients with knee osteoarthritis.[19] The intervention, delivered using a head-mounted display (HMD) device and a smartphone app, facilitated repetitive quadriceps and isometric vastus medialis oblique exercises over a 12-week period. The control group received standard exercise instructions through paper-based pamphlets. Rolbiecki et al. combined VR with neurofeedback (VR + NF) for managing cancer-related symptoms, including pain and anxiety.[20] This intervention involved nature-based guided meditations using Healium™ software, Oculus VR headsets, and Brainlink EEG devices, administered over two sessions spaced approximately three weeks apart. The control group received only VR-guided meditations, excluding NF. Garcia et al. conducted a double-blind, randomised, placebo-controlled trial to assess an at-home VR-based program called EaseVRx, designed for chronic low back pain.[21] The intervention included CBT, mindfulness, and pain neuroscience education, delivered via the Pico G2 4K VR headset over an eight-week period. Participants in the control group experienced a Sham VR condition, involving non-immersive 2D nature footage.
Outcomes and Effectiveness
Pain Intensity Reduction
The studies provided mixed findings on pain intensity reduction. Garcia et al. reported a significant reduction in average pain intensity in the EaseVRx group, showing a 2.41-point decrease on the Numeric Rating Scale (NRS) compared to the Sham VR control group, indicating the strong effectiveness of the VR intervention in managing chronic low back pain.[21] In contrast, Lo et al. did not find a statistically significant reduction in pain intensity between the VRiKnee and control groups, although the VR group demonstrated higher adherence to the exercise regimen.[19] Rolbiecki et al. observed a significant reduction in anxiety and pain levels in participants who received the VR + NF intervention, suggesting preliminary efficacy for cancer-related symptom management.[20]
Feasibility and Retention
Feasibility and adherence rates were reported across the studies, indicating varying levels of success in retaining participants and maintaining adherence to intervention protocols. Lo et al. reported a high recruitment rate of 100%, with retention rates of 80% in the VR group and 93% in the control group.[19] The VR group demonstrated a higher adherence rate (77%) compared to the control group (62%), although the difference was not statistically significant. Rolbiecki et al. recorded a retention rate of 67%, with adherence rates approximating five sessions per week for the VR-only group and six sessions per week for the VR + NF group.[20] Dropouts in this study were largely attributed to technical difficulties and health-related challenges. Garcia et al. achieved high retention rates, with 87.5% of participants completing the eight-week EaseVRx intervention, and 78.6% completing a six-month follow-up.[21] Adherence rates were comparable between the EaseVRx and Sham VR groups.
Acceptability and User Satisfaction
The studies also evaluated acceptability and user satisfaction with the interventions. Lo et al. identified significant technical difficulties, including hardware malfunctions and cybersickness, which affected approximately 33% of participants and had a notable impact on intervention acceptability.[19] Conversely, Rolbiecki et al. found the VR + NF intervention to be generally acceptable for managing cancer symptoms, though participants reported some challenges with technical navigation.[20] Garcia et al. reported high levels of user satisfaction, with 92.1% of participants expressing satisfaction or higher with the EaseVRx program.[21] Usability ratings were high and similar for both the EaseVRx and Sham VR groups.
Quality Assessment
Quality assessments of the included studies were conducted using the Cochrane ROB 2 tool. Garcia et al. demonstrated a low risk of bias across all domains, with adequate randomisation, effective blinding, and complete data reporting.[21] Lo et al. were found to have a high risk of bias, largely due to the inability to blind participants and outcome assessors, despite meeting the criteria for proper randomisation and data completeness.[19] Rolbiecki et al. raised some concerns regarding the adequacy of randomisation procedures and the lack of sufficient blinding, although data reporting and outcome adherence were deemed acceptable.[20]
The three studies showed variable effectiveness of VR for chronic pain in older adults. Garcia et al. offered strong evidence for pain reduction,[21] while Lo et al. and Rolbiecki et al. highlighted the feasibility and preliminary efficacy.[19,20] Technical issues and adherence variability impacted overall outcomes.
Discussion
This review suggests VR may effectively reduce pain, support exercise adherence, and offer an acceptable non-pharmacological option for chronic pain in older adults, though effectiveness varied across studies. The study by Garcia et al. provided the most robust evidence regarding the efficacy of VR in pain management.[21] Specifically, the EaseVRx program was found to significantly reduce chronic low back pain intensity compared to a Sham VR control. The double-blind, randomised, placebo-controlled design, coupled with a large sample size, strengthens the reliability of these findings. Notably, the integration of CBT, mindfulness, and pain neuroscience education within the VR platform appeared to enhance its effectiveness, suggesting that a multidisciplinary approach delivered via VR may be a valuable strategy in chronic pain management. In contrast, the studies by Lo et al. and Rolbiecki et al. focused more on the feasibility and preliminary efficacy of VR interventions rather than on definitive pain reduction outcomes.[19,20] Lo et al. reported higher adherence rates in participants using VR compared to control groups, indicating some behavioural benefit.[19] However, the study failed to demonstrate a significant reduction in pain levels, and the presence of technical difficulties, such as cybersickness, limited the overall effectiveness of the intervention. Rolbiecki et al., exploring the combined use of VR and NF for managing cancer-related pain, reported reductions in anxiety and pain.[20] However, issues related to retention rates and feasibility prevented conclusive efficacy assessments. Despite these limitations, the initial evidence from these studies suggests that VR may contribute positively to the psychological aspects of pain management, though further evidence is needed to establish consistent effects on pain intensity.
The reviewed studies generally reported favourable feasibility metrics, although challenges remained. Garcia et al. demonstrated high recruitment and retention rates, emphasising the acceptability of VR interventions for older adults when designed thoughtfully and executed with technical reliability.[21] In contrast, technical barriers presented significant obstacles in Lo et al., where issues such as cybersickness, hardware malfunctions, and participant frustration with VR technology were prominent.[19] Similar, though less severe, issues were reported in Rolbiecki et al.[20] Despite these challenges, participants expressed a positive perception of VR interventions, with Garcia et al. showing particularly high user satisfaction and Rolbiecki et al. demonstrating that acceptability remained adequate when technical issues were minimised.[20,21] These findings underscore the importance of ensuring the technological robustness of VR platforms, as such issues may deter participants from engaging with and benefiting from these interventions.
The quality appraisal revealed notable variability in risk of bias across studies. Garcia et al. demonstrated low risk due to robust randomisation, effective blinding, and rigorous data handling, enhancing internal validity.[21] In contrast, Lo et al. had a high risk of bias from inadequate blinding, raising concerns about performance and detection biases.[19] Rolbiecki et al. showed some concerns related to randomisation and blinding, though data reporting was adequate.[20] Common limitations included limited sample diversity, as most participants were female and ethnically homogeneous, restricting generalisability. Technical issues such as cybersickness, hardware malfunctions, and software glitches were frequent, underscoring the need for more reliable VR systems. Furthermore, short follow-up periods across studies limited understanding of long-term efficacy. These methodological weaknesses and practical challenges highlight the need for future research employing rigorous designs, diverse samples, and extended follow-up to better evaluate the sustainability and broader applicability of VR interventions for chronic pain in older adults.
The positive findings from Garcia et al. advocate for integrating VR into multimodal pain management for older adults.[21] As a non-pharmacological adjunct, VR may enhance pain relief and quality of life,[22,23] yet technical barriers continue to limit clinical implementation. Addressing these challenges is critical to facilitate broader uptake. Future research should prioritise more diverse participant samples to improve generalisability across ethnicity, gender, and socioeconomic status. Technological advancements must focus on creating intuitive, dependable VR systems tailored to older adults, mitigating issues such as cybersickness and hardware malfunction.[24] Longitudinal studies are essential to assess the durability of VR’s benefits over time, including sustained pain reduction and behavioural change. Mechanistic research is needed to elucidate how VR modulates pain perception and psychological well-being, thereby guiding content refinement. High-quality research, emphasising rigorous blinding and robust control conditions, is crucial to reduce bias and reinforce the validity of findings, ultimately informing clinical applicability.
This review identified only three eligible studies, underscoring the nascent stage of research on VR for chronic pain in older adults. Significant heterogeneity in interventions, conditions, and outcomes precluded meta-analysis, necessitating a narrative synthesis. Methodological variability and risk of bias compromised reliability. The predominance of female participants, limited diversity, and language bias restricted generalisability. Short follow-up periods hindered the assessment of long-term effects. Exclusion of non-randomised and qualitative studies reduced insight into feasibility and user experience. Additionally, publication bias was not assessed, potentially affecting conclusions. Future reviews should address these limitations to strengthen evidence synthesis and clinical applicability.
Conclusion
VR interventions hold significant promise as effective tools for managing chronic pain in older adults, offering benefits in pain reduction, adherence to exercise regimens, and user satisfaction. However, the effectiveness of these interventions is moderated by several challenges, including technical issues such as cybersickness and hardware usability, as well as variability in the quality of current evidence. The inconsistencies in outcomes across various studies underscore the need for improved methodological rigour and more diverse, larger sample populations. Future research should focus on refining VR technology for enhanced usability, expanding the diversity of participants, and exploring long-term effects. Addressing these areas could significantly bolster VR’s viability as an accessible and sustainable tool for chronic pain management in older adults.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Shuti Shankar and Dr Tamilselvan Selvam for their contributions in the conduct of this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical permission was not applicable for this article, as this is a review article drafted from various research articles and not from patients directly.
Informed consent
Consent was not applicable, as this is a review article compiled from various research articles and guidelines and not from patients directly.
Credit author statement
Conceptualisation: Swaminathan Ramasubramanian, Sathish Kumar K, Ravi Sundararaj.
Methodology: Swaminathan Ramasubramanian, Ravi Sundararaj, Malai Ammal M.
Formal Analysis and Investigation: Swaminathan Ramasubramanian, Vigneshwaran Maheshwaran, Sonali Dhanaseelan, Yamuna Devi, Kavitha Varatharajan, Arun Murugan.
Writing – original draft preparation: Swaminathan Ramasubramanian, Yamuna Devi, Ravi Sundararaj.
Writing – review and editing: Swaminathan Ramasubramanian, Yamuna Devi, Ravi Sundararaj.
Data availability
Contained within the manuscript.
Use of artificial intelligence
AI was used for language editing
Prospero registration
CRD420251053610