
Abstract
Background and Aims:
Musculoskeletal (MSK) radiology is integral for diagnosing and managing traumatic, degenerative, inflammatory and neoplastic disorders. Many MSK imaging modalities, particularly computed tomography (CT) and fluoroscopy, involve ionising radiation, raising concerns about cumulative patient dose, especially in children, pregnant women and patients undergoing repeated imaging for chronic or cancer-related conditions.
Purpose:
To review current challenges in radiation safety within MSK radiology and to highlight strategies, technologies and workflow modifications aimed at minimising radiation exposure while maintaining diagnostic accuracy. Importance is given to artificial intelligence (AI) and its applications for dose optimisation.
Content:
The review outlines radiation protection principles (justification, optimisation, dose limitation) and their application to MSK radiology. Specific focus is given to paediatric imaging (emphasising protocol tailoring, non-ionising alternatives and ALARA compliance), pregnancy and trauma (dose mitigation during urgent imaging and obstetric safety considerations), chronic disease and cancer surveillance (balancing diagnostic yield with dose tracking and cumulative exposure management), technology solutions (AI-based dose optimisation, synthetic CT generation from MRI, dual-energy CT, low-dose CT protocols), emerging innovations (photon-counting CT, robotic ultrasound, low-field portable MRI, and augmented reality guidance for interventions) and operational strategies (radiation safety audits, adherence to diagnostic reference levels (DRLs) and occupational protection measures, and real-time dosimetry).
Summary:
Radiation safety in MSK radiology is a multidisciplinary responsibility requiring integration of optimised protocols, modern technology, AI applications and adherence to international safety standards. Practical recommendations provided in this review aim to minimise radiation risks to both patients and healthcare workers while ensuring high diagnostic quality in MSK imaging.
Keywords
Introduction
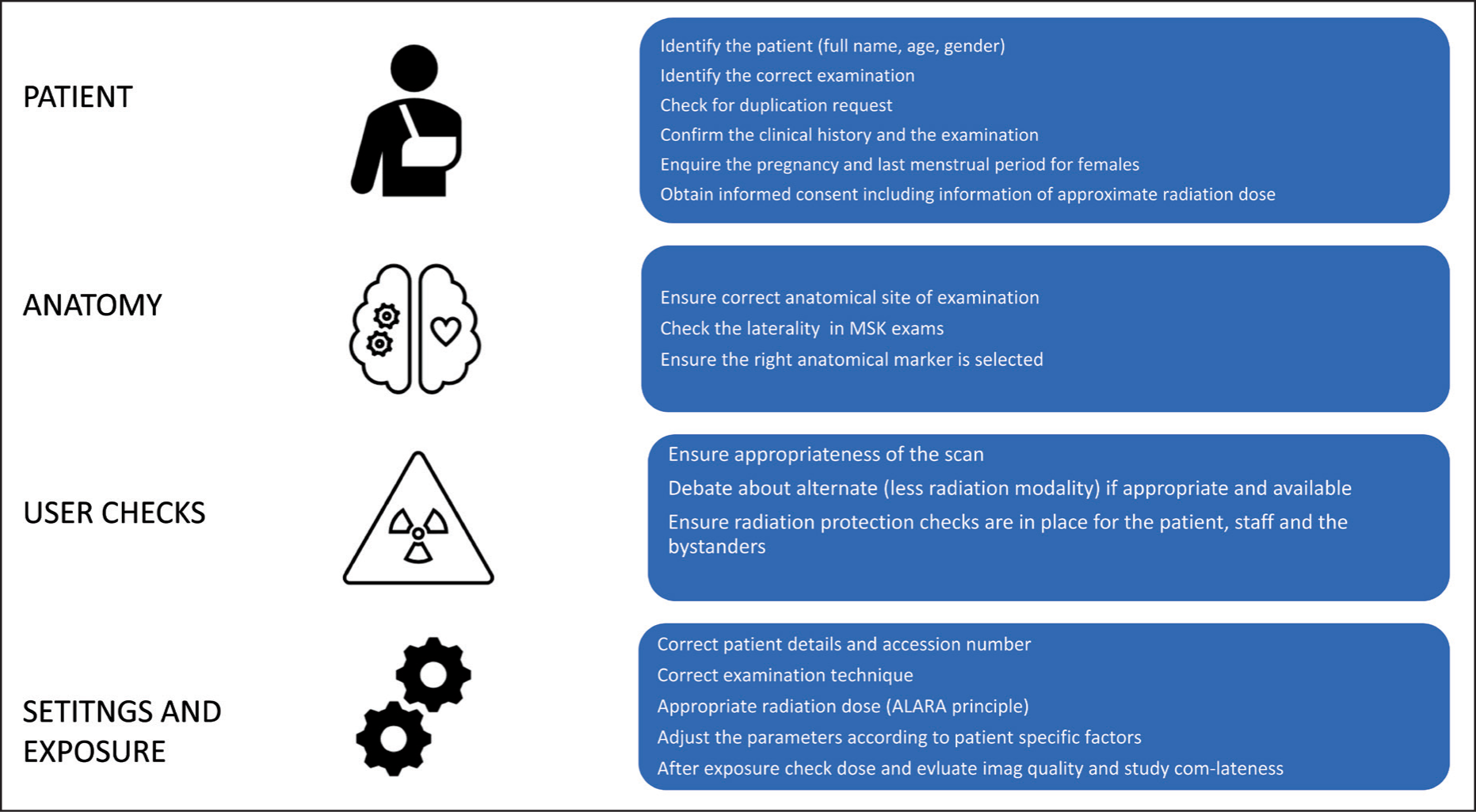
Musculoskeletal (MSK) radiology is an essential subspecialty in medical imaging, supporting diagnosis, disease monitoring and treatment planning for a wide range of conditions, including trauma, arthritis, sports injuries and bone malignancies. However, the growing reliance on ionising imaging modalities such as computed tomography (CT) and fluoroscopy has raised significant concerns about patient and occupational radiation exposure. This is especially critical for patients undergoing repeated scans for chronic conditions or cancer surveillance. The overarching principle of radiation protection—ALARA (As Low as Reasonably Achievable)—must guide all imaging practices to mitigate risks while maintaining diagnostic efficacy [Figure 1].
General Principles of Radiation Protection and International Law
Radiation safety is grounded in three core principles defined by the International Commission on Radiological Protection (ICRP): justification, optimisation and dose limitation.[1] Justification mandates that any imaging involving radiation should offer a net clinical benefit. Optimisation aims to minimise dose without compromising diagnostic quality, and dose limits ensure occupational and public exposures remain within safe thresholds.
Internationally, ICRP recommends an annual effective dose limit of 20 mSv for radiation workers, averaged over five years, and 1 mSv for the general public.[1–3] In medical imaging, however, patients are not subject to hard dose limits but benefit from diagnostic reference levels (DRLs) to guide safe practice. National regulatory bodies such as the American College of Radiology (ACR) and the National Council on Radiation Protection and Measurements (NCRP) provide country-specific protocols aligned with these principles.[4]
Radiation Safety in MSK Radiology
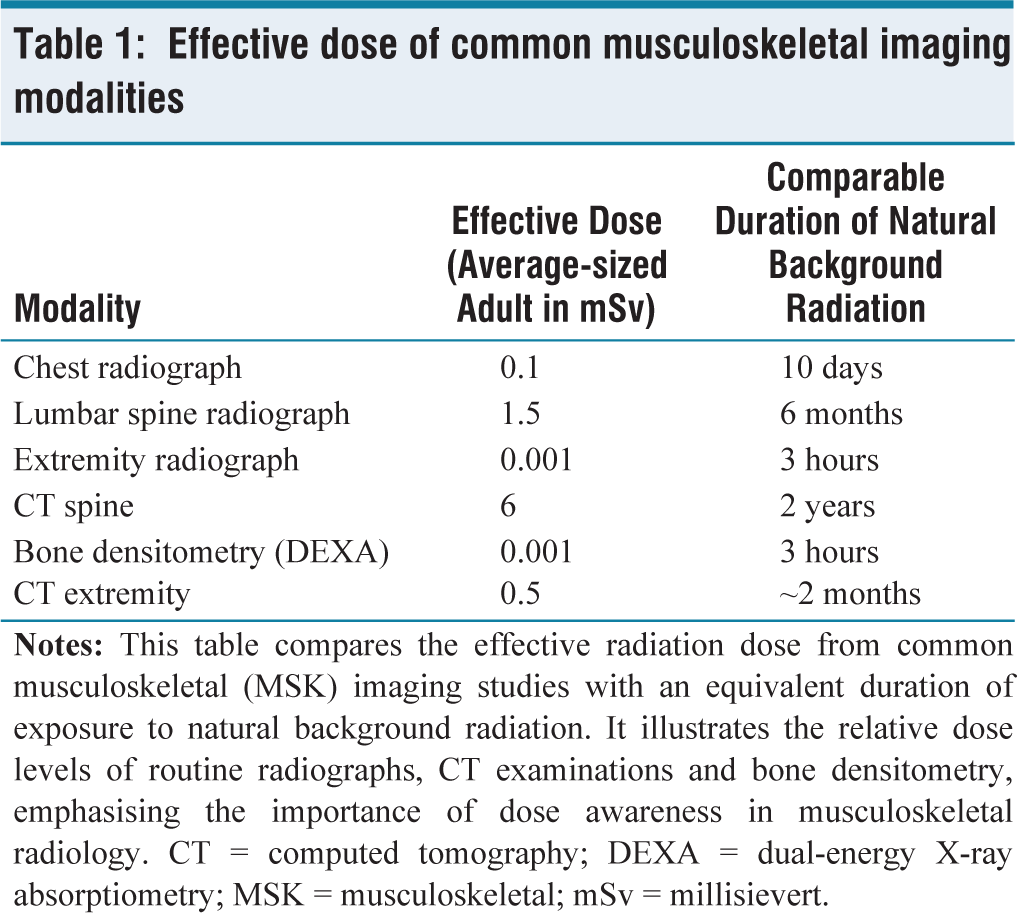
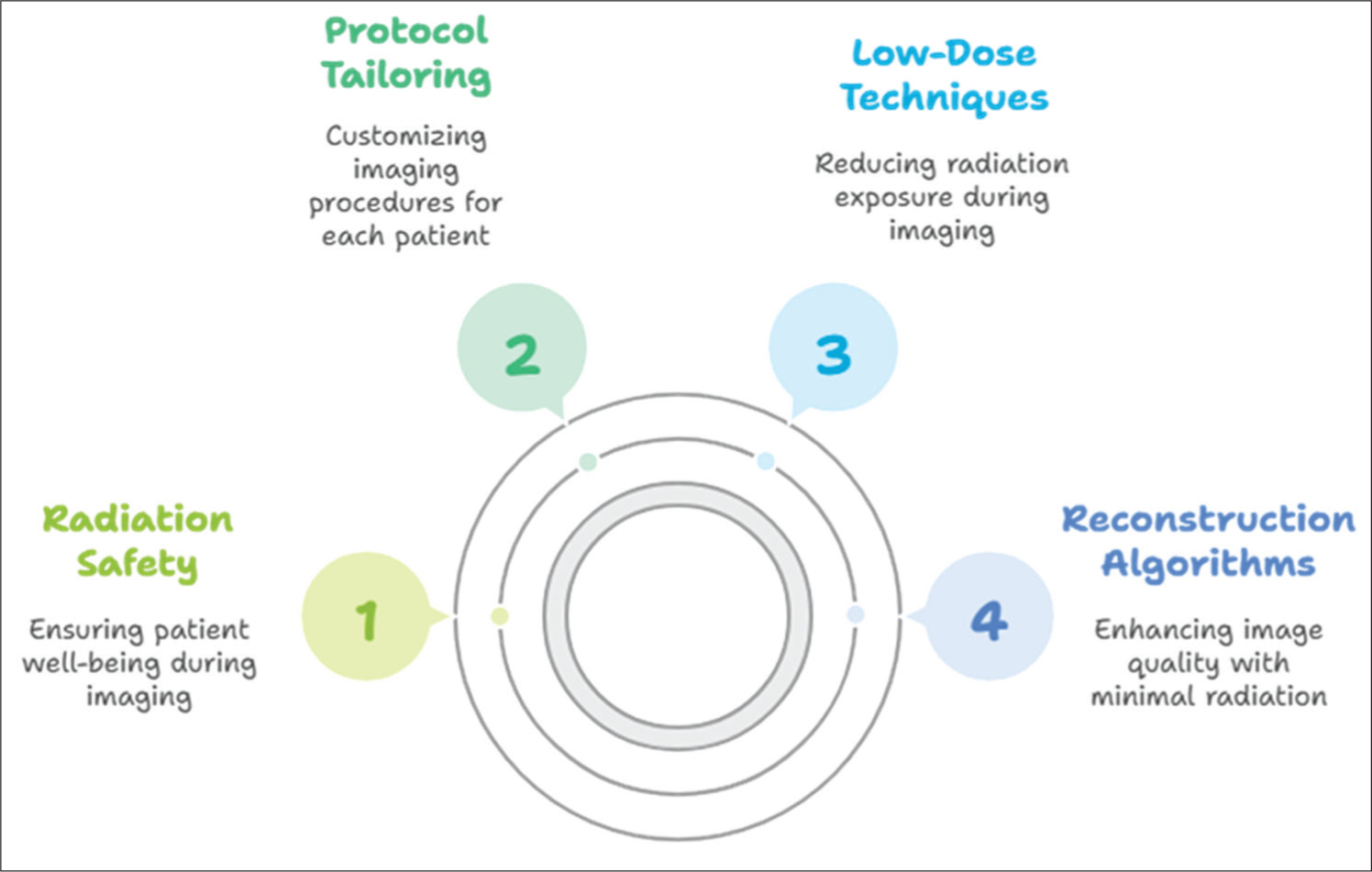
MSK imaging frequently utilises radiographs, CT scans, and fluoroscopic guidance for interventions. While radiographs contribute relatively low doses, CT and fluoroscopy involve higher exposures, particularly in trauma, oncology and interventional procedures. Risks are amplified with repetitive imaging in chronic disease management [Table 1]. CT of the lumbar spine, for example, can reach up to 19 mSv, equivalent to over 600 chest X-rays. Therefore, protocol tailoring, low-dose techniques, and advanced reconstruction algorithms are critical for MSK radiology practice [Figure 2].
Effective dose of common musculoskeletal imaging modalities
Radiation safety in MSK radiology
Radiation Protection in Special Categories
Radiation Safety in Children: Focus on MSK Radiology
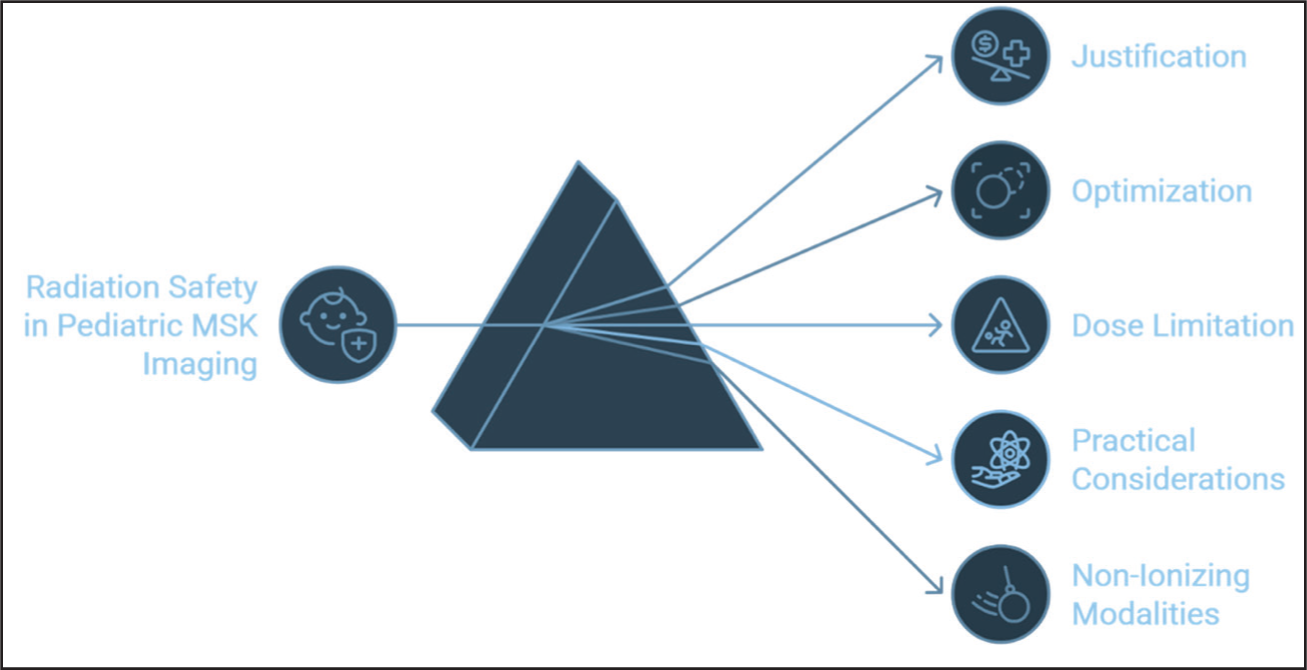
Radiation safety in paediatric MSK radiology is of critical importance due to children’s increased radiosensitivity, which arises from their smaller body size, rapid cellular proliferation and longer remaining life expectancy. These factors heighten the risk of radiation-induced long-term effects such as cancer.[5,6] Accordingly, the foundational principles of radiation protection—justification, optimisation and dose limitation—are especially crucial in paediatric imaging[1–3] [Figure 3]. Given that MSK imaging frequently involves radiographs, CT and MRI, practitioners must carefully balance the need for diagnostic accuracy with the imperative to minimise radiation exposure.
Radiation safety in paediatric MSK imaging
Justification and Optimisation
All imaging procedures that involve ionising radiation must be clearly justified, ensuring that the expected clinical benefit outweighs any associated risk.[1] In paediatric MSK imaging, radiographs remain the primary modality due to their low radiation dose, wide availability and cost-effectiveness. However, CT and MRI may be necessary for complex evaluations, such as detailed fracture assessment, bone tumours, or soft tissue pathology.
Optimisation involves adapting imaging parameters to the child’s age, body size and clinical indication to ensure the lowest achievable dose while preserving diagnostic quality.[1–3] This includes the use of:
Tight collimation to restrict the irradiated area Appropriate shielding to protect radiosensitive organs Weight-based or age-based CT protocols that tailor tube current and voltage to the child’s physiology[7]
Practical Considerations
Implementing paediatric-specific protocols and equipment settings is essential, as the use of standard adult protocols can lead to unnecessary or excessive radiation exposure in children. Medical physicists play a vital role in reviewing and adjusting imaging parameters, ensuring compliance with DRLs, and maintaining quality assurance processes.[8]
Whenever possible, non-ionising imaging modalities should be prioritised. Ultrasound, which is both safe and highly effective, is increasingly used as a first-line modality in paediatric MSK imaging—particularly for assessing soft tissue injuries, joint effusions and inflammatory conditions. MRI, while free from ionising radiation, may present challenges in the paediatric population due to longer scan times and the potential need for sedation, especially in younger or less cooperative patients. Thus, the decision to use MRI must consider both the diagnostic benefit and the practical risks
Radiation Safety in Pregnancy: Focus on Musculoskeletal Radiology
Imaging pregnant patients requires careful consideration, particularly in MSK radiology, where trauma or orthopaedic evaluation may necessitate radiographic or CT imaging. Ensuring foetal safety is paramount, and all imaging should adhere to the ALARA principle to minimise radiation exposure without compromising diagnostic efficacy.[1–3]
Most diagnostic imaging procedures deliver foetal radiation doses well below the 50 mSv threshold associated with potential harm. Importantly, the majority of single diagnostic examinations result in foetal doses under 10 mSv, levels not typically linked with adverse effects. However, the critical period of organogenesis (weeks 3–15 of gestation) demands particular caution, as exposure to doses exceeding 100 mGy during the first trimester has been associated with increased risks of spontaneous abortion, congenital malformations and neurodevelopmental delay.[9,10]
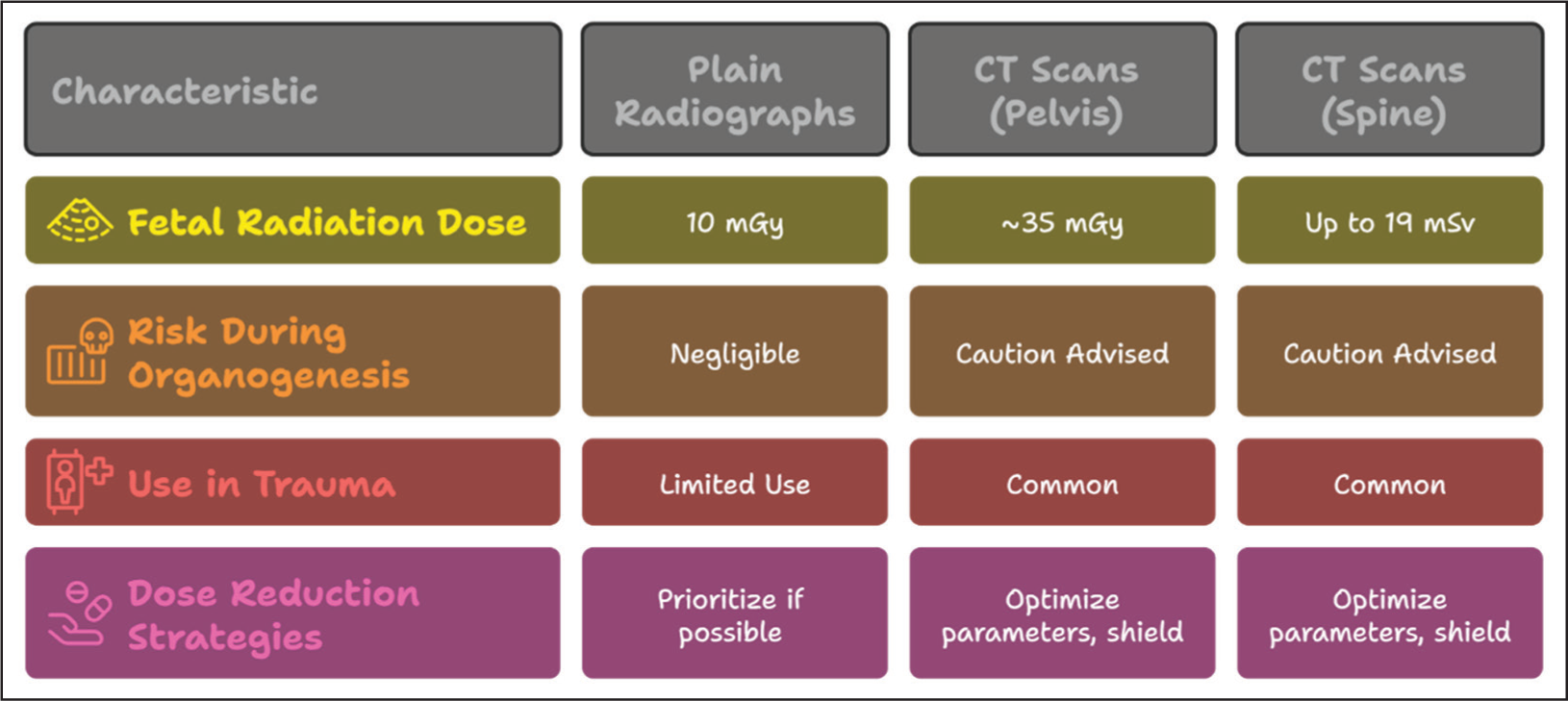
Plain radiographs of peripheral joints and the cervical spine typically expose the foetus to negligible doses, often less than 10 mGy. In contrast, CT scans of the pelvis, which are occasionally required in trauma settings, may deliver approximately 35 mGy—a value still below the deterministic threshold but significantly higher than standard radiographs [Figure 4].
Radiation exposure from different modalities in pregnancy and dose reduction strategies
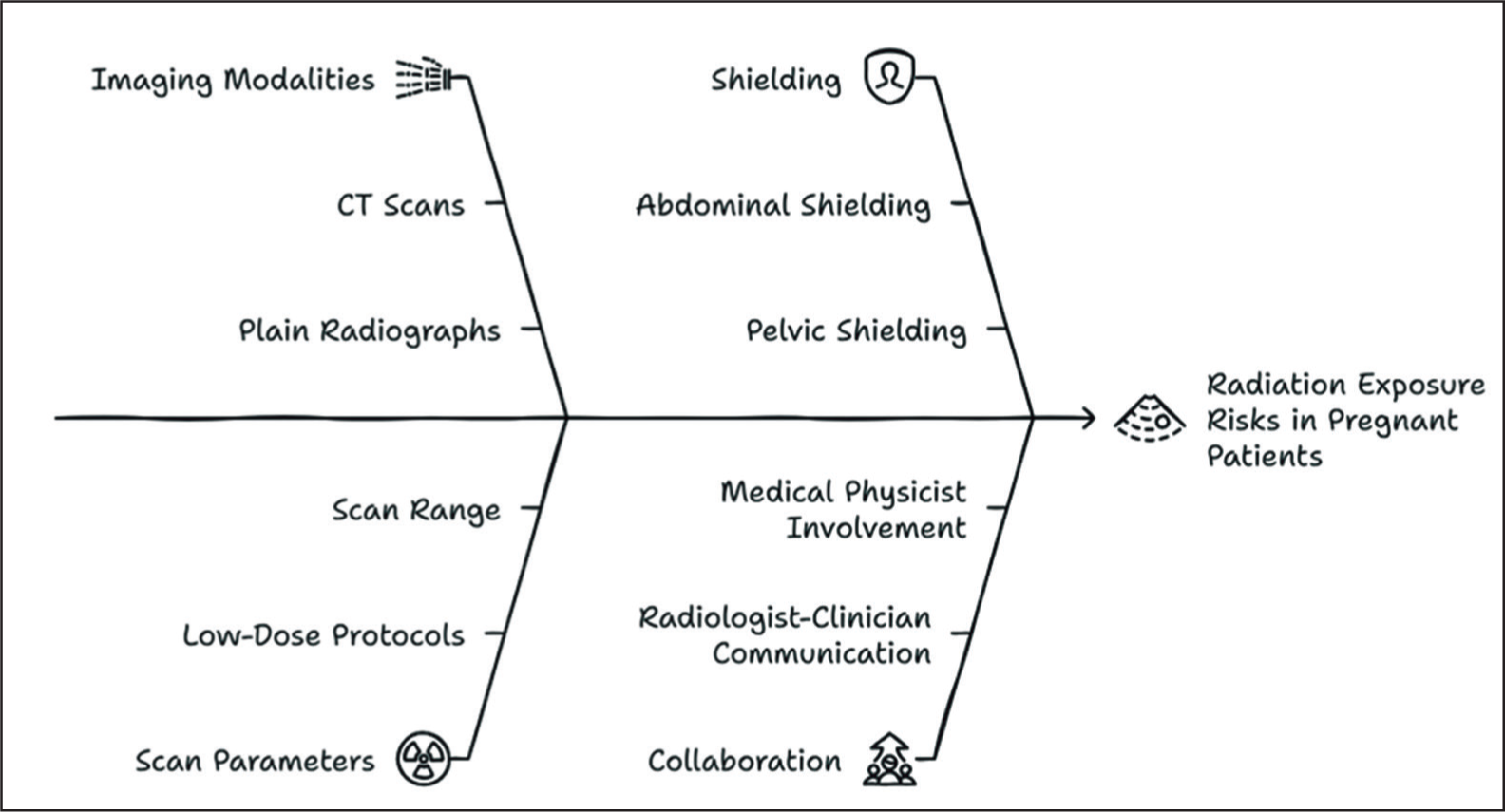
To mitigate foetal risk, cumulative radiation exposure should be monitored, particularly in patients undergoing repeated imaging.[11] Non-ionising modalities such as ultrasound and MRI should be prioritised when clinically appropriate, especially for soft tissue evaluation or when imaging the extremities [Figure 5].
Radiation safety in pregnancy
Additional dose reduction strategies include:
Optimising scan parameters (e.g., using low-dose CT protocols) Limiting scan range to the region of interest Employing lead shielding over the abdomen and pelvis whenever feasible Avoiding multiphase or contrast-enhanced studies unless absolutely necessary
Collaboration between radiologists, referring clinicians and medical physicists is critical to ensure that imaging in pregnancy is both safe and diagnostically effective.
Major Trauma
In acute trauma, expedient diagnosis is paramount, often necessitating high-dose modalities. A pelvic CT (4.8 mSv) or spine CT (up to 19 mSv) are common. Nevertheless, dose minimisation through pulsed fluoroscopy, iterative reconstruction and limiting scan range must be employed.
Chronic MSK Conditions and Cancer
Patients with rheumatoid arthritis, osteoarthritis, or bone metastases often require serial imaging. Adopting low-dose CT, replacing surveillance scans with MRI, and tracking cumulative dose exposure are vital strategies.
Role of MSK Ultrasound in Radiation Safety
Ultrasound is a radiation-free imaging modality and is increasingly used in MSK radiology, particularly for evaluating tendons, ligaments, joint effusions and guiding injections. In paediatrics and pregnancy, it often replaces X-rays and CT. Innovations such as high-frequency linear probes and contrast-enhanced ultrasound further enhance its diagnostic value. It is the preferred first-line modality where appropriate, significantly contributing to overall dose reduction.
Role of Low Dose CT in MSK Imaging
Modern CT scanners enable significant radiation reduction using techniques such as:[12]
Automatic exposure control (AEC) Tube current modulation Iterative reconstruction algorithms
For extremity imaging or chronic follow-up studies, low-dose protocols can achieve diagnostic quality at a fraction of conventional doses. For example, a low-dose CT for knee arthritis can be performed at <1 mSv [Table 2].
Radiation dose in low-dose CT protocols for musculoskeletal applications
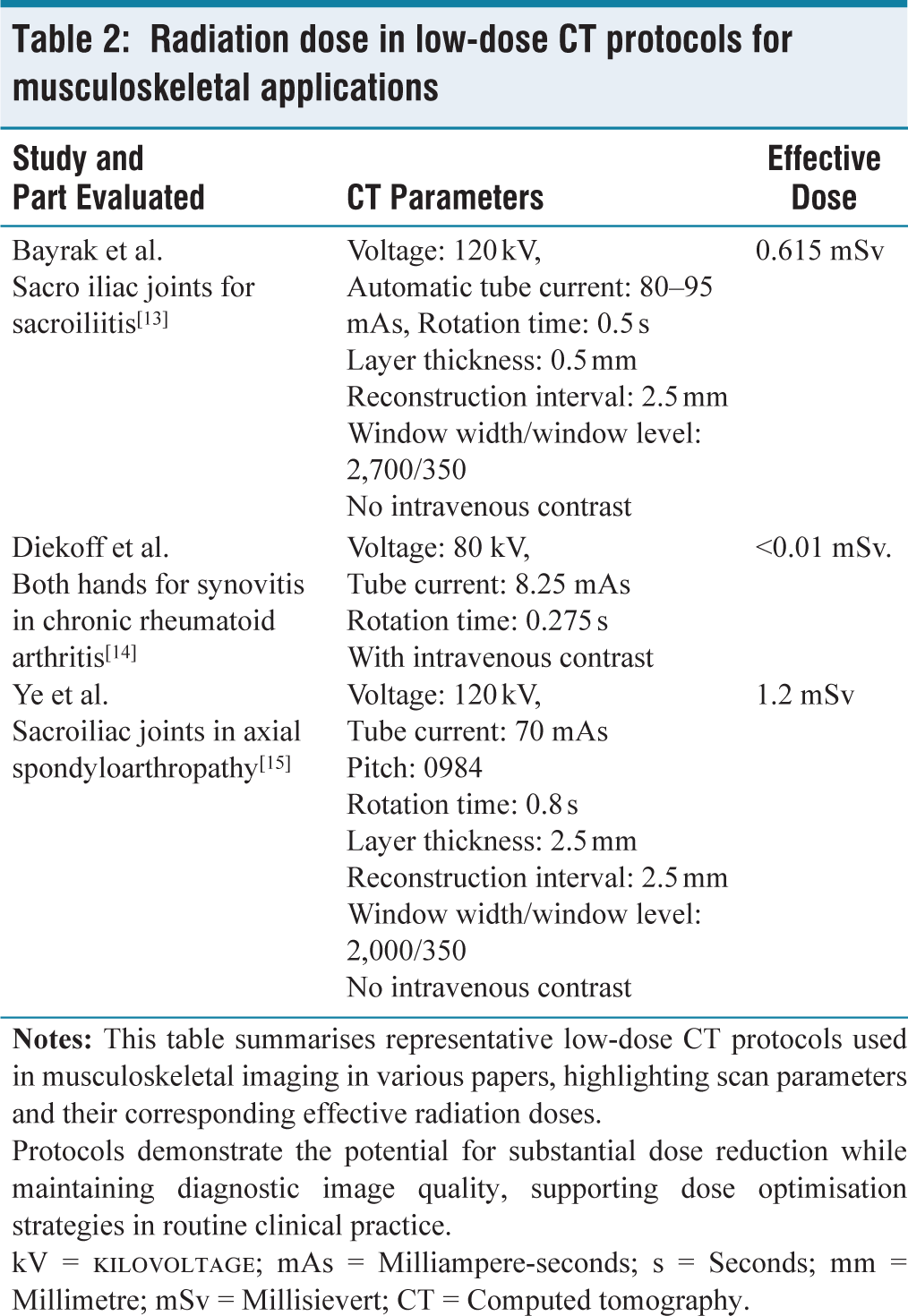
Protocols demonstrate the potential for substantial dose reduction while maintaining diagnostic image quality, supporting dose optimisation strategies in routine clinical practice.
kV = Kilovoltage; mAs = Milliampere-seconds; s = Seconds; mm = Millimetre; mSv = Millisievert; CT = Computed tomography.
Role of MRI in Radiation Safety
Magnetic Resonance Imaging (MRI) plays an indispensable role in MSK radiology due to its superior soft tissue contrast, multi-planar capability and absence of ionising radiation [Figure 6]. It is particularly beneficial for evaluating ligamentous injuries, bone marrow oedema, tumour characterisation, cartilage assessment and neuromuscular disorders.
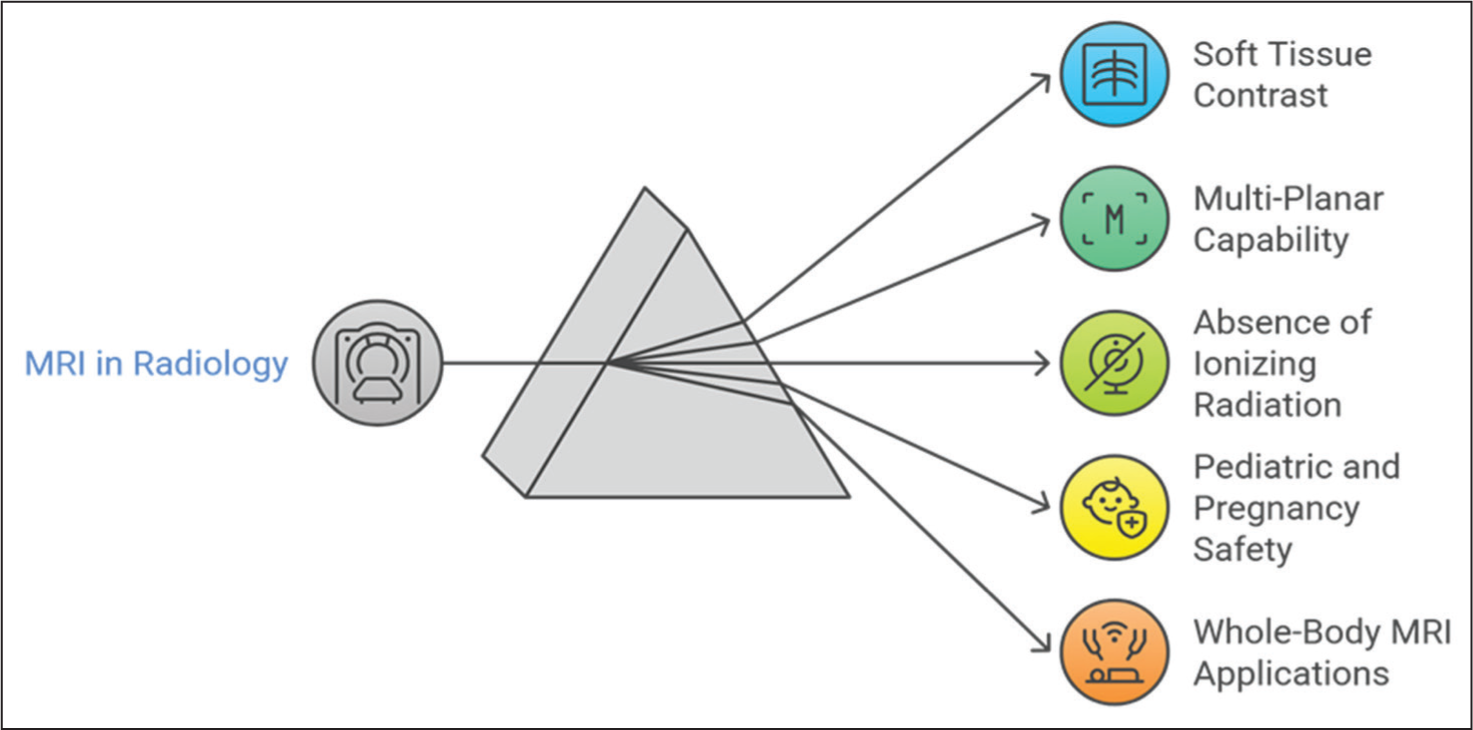
MRI is often the modality of choice in children and pregnant patients, where ionising radiation poses a higher risk. In paediatric inflammatory arthritis, juvenile osteomyelitis and soft tissue tumours, MRI provides both anatomical and functional insights without compromising safety.
A significant advance in this field is the increasing use of Whole-Body MRI (WB-MRI) as a radiation-free alternative to conventional skeletal survey or whole-body CT.[16] WB-MRI is particularly useful in:
Multiple myeloma: WB-MRI has demonstrated superior sensitivity in detecting bone marrow infiltration compared to skeletal surveys, and it can identify early medullary involvement even before cortical destruction is visible. Bone metastases: WB-MRI allows comprehensive assessment of skeletal metastases with higher diagnostic accuracy than scintigraphy or PET in certain cancers. Chronic recurrent multifocal osteomyelitis (CRMO): WB-MRI provides a holistic view of multifocal lesions in a single session, aiding early diagnosis and therapy monitoring. Rheumatoid arthritis: MRI of the whole body, or targeted joints, can detect synovitis, erosions and tenosynovitis in the early stages, guiding aggressive management before irreversible damage occurs.
Although MRI has limitations such as longer acquisition times, cost and requirement for sedation in some children, the advent of faster sequences and motion correction algorithms continues to expand its utility.
Role of Artificial Intelligence Algorithms in Radiation Protection
Artificial intelligence (AI) is revolutionising radiation safety through multiple applications. Each function contributes uniquely to dose reduction and clinical workflow enhancement.[17] [Figure 7] AI provides a wealth of knowledge in the field of MSK radiology and is an indispensable tool as we look to further our expertise as radiologists and clinicians treating patients with common and occult MSK conditions.[18]
Role of AI in radiation protection
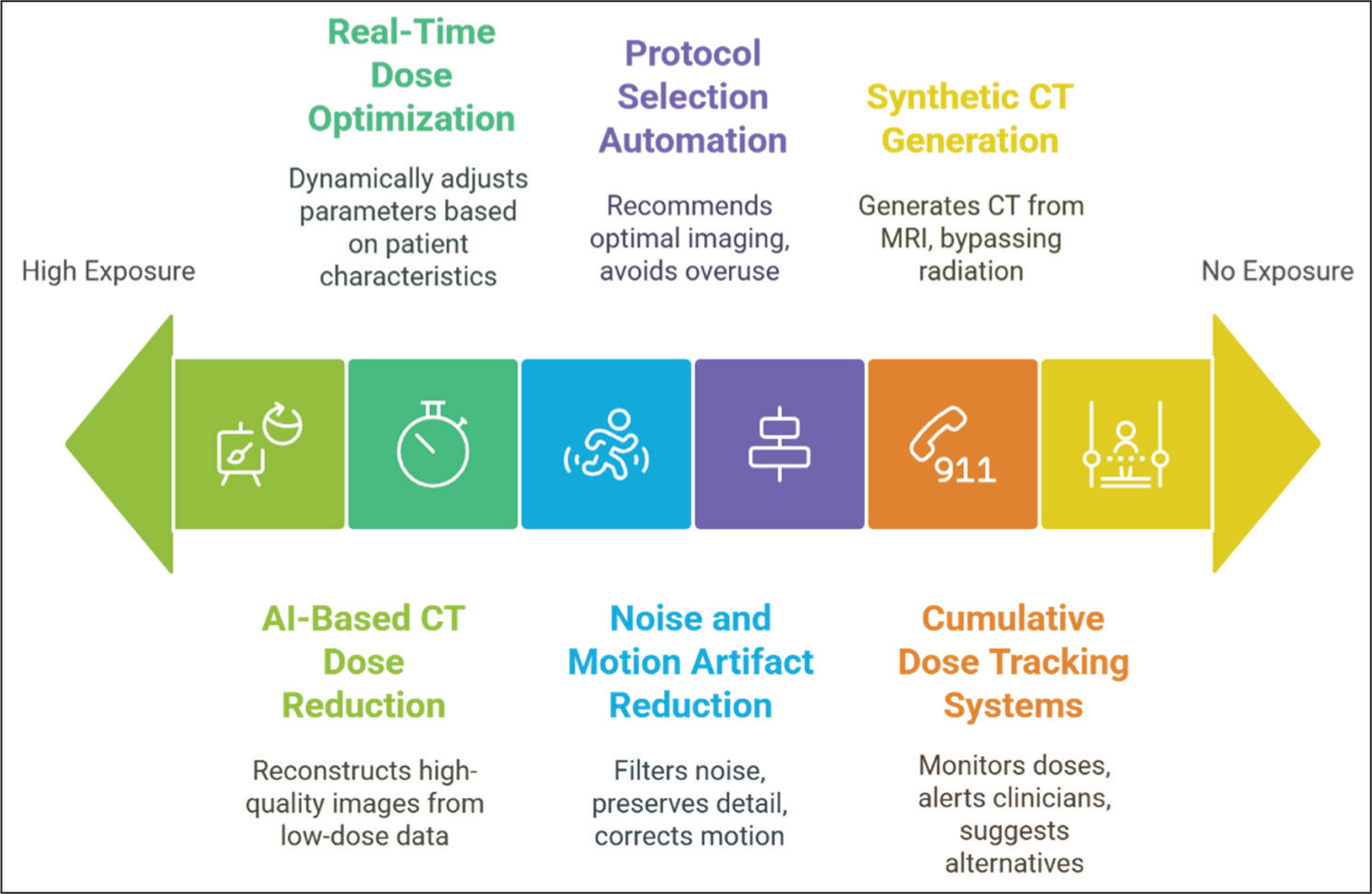
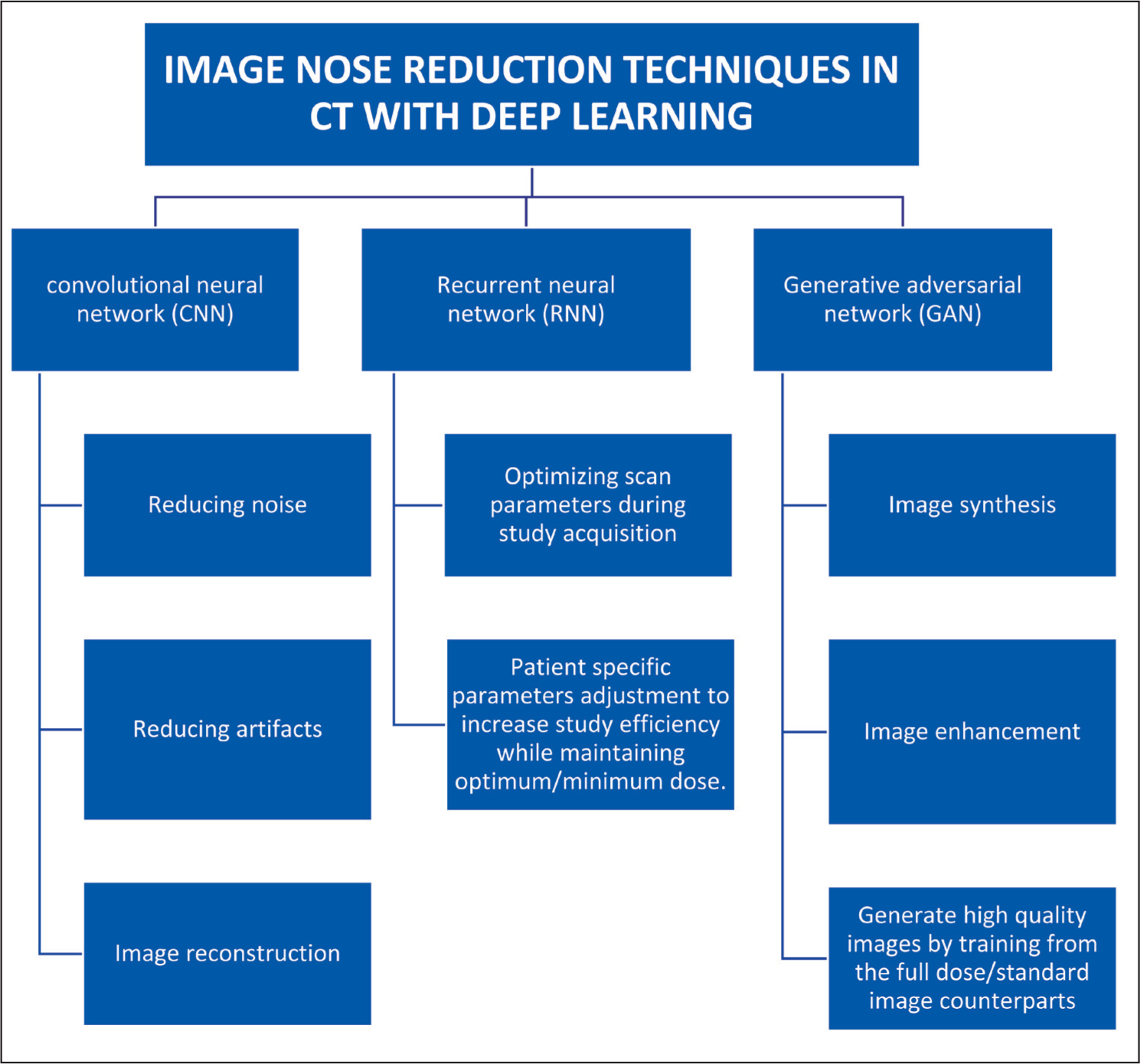
AI-based CT Dose Reduction and Dose Prediction
Machine learning (ML) techniques are increasingly being used to reduce radiation dose in CT imaging by reconstructing high-quality images from lower-quality or limited raw data acquired at reduced tube currents.[19] Similar to acceleration strategies in MRI, these AI-based algorithms enhance image quality despite low-dose acquisition.[20] This demonstrates AI’s significant potential in enabling substantial radiation dose reductions without compromising diagnostic accuracy [Figure 8].
Real-time Dose Optimisation Based on Patient Size and Anatomy
AI algorithms can adjust scan parameters dynamically by analysing patient size, anatomy and clinical indications prior to the scan.[21,22] These systems automatically tailor kilovoltage, tube current and scan length, ensuring diagnostic quality while minimising exposure.[23] This is particularly useful in CT and fluoroscopy, where operator-dependent variability is high.[24]
Synthetic CT Generation from MRI
AI models can generate synthetic CT datasets from MRI scans, enabling applications such as pre-operative planning for spine surgery and radiotherapy simulation.[25] This bypasses the need for additional CT scans, eliminating associated radiation exposure, especially beneficial in paediatric scoliosis, spine tumours and deformity corrections.
Noise and Motion Artefact Reduction
Deep learning-based denoising tools enhance image quality in low-dose acquisitions by filtering noise while preserving anatomical detail.[26] This is crucial in CT imaging, where image quality often deteriorates with reduced dose. Motion artefact correction also reduces the need for repeat scans, especially in uncooperative or paediatric patients.
Protocol Selection Automation to Avoid Unnecessary Scans
AI systems can recommend optimal imaging protocols based on clinical history, prior imaging and institutional best practices. This avoids overuse of high-dose modalities and ensures alignment with diagnostic goals, thereby contributing to radiation stewardship.[27,28]
Cumulative Dose Tracking Systems for Chronic Patients
AI-powered dashboards can aggregate and monitor patient radiation doses across multiple studies over time. These tools alert clinicians when thresholds are being approached and suggest alternative imaging pathways, helping to balance diagnostic necessity with safety, especially in patients with chronic conditions or malignancies.[27]
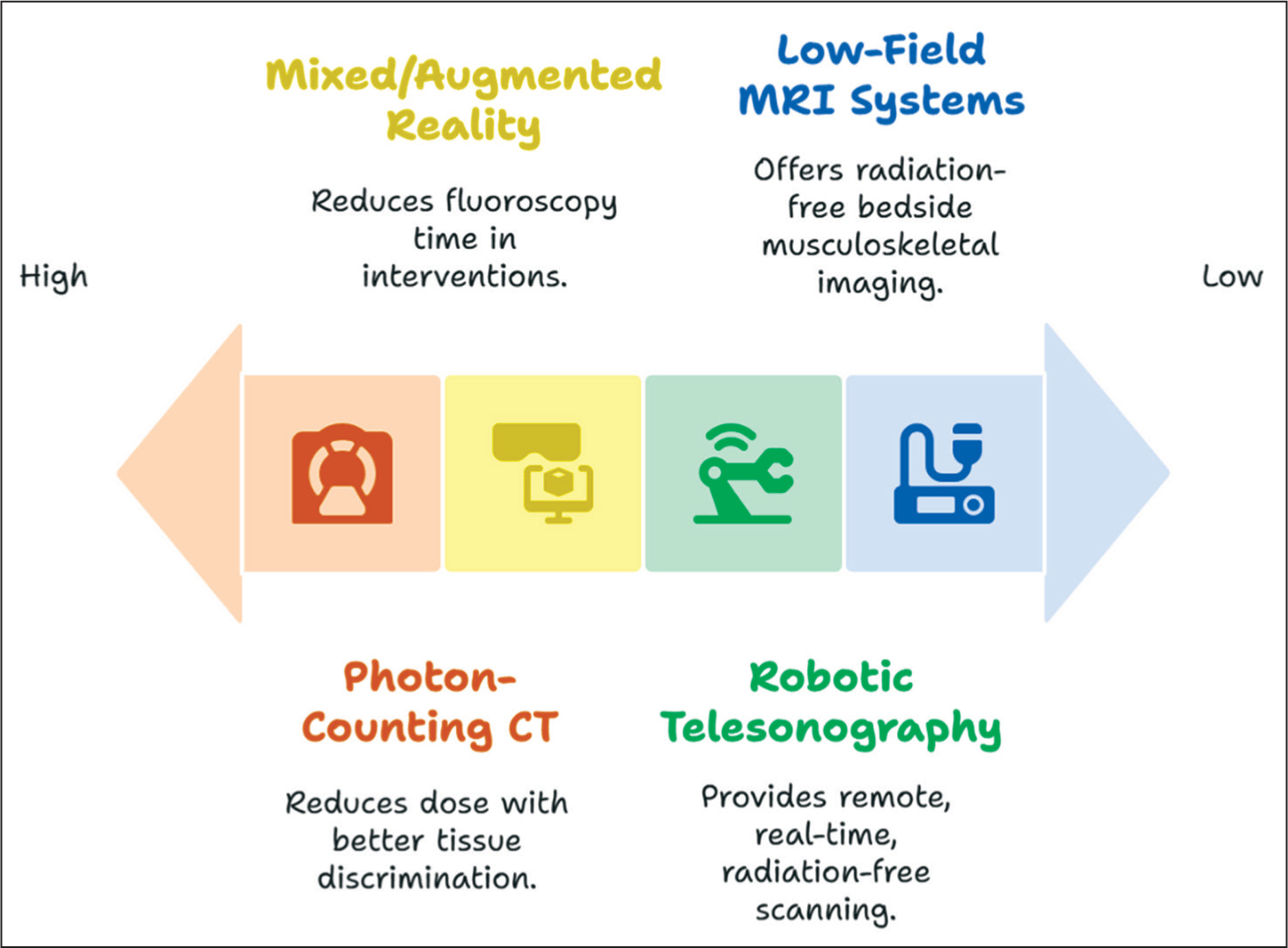
Role of Emerging Technologies
The frontier of radiation safety in MSK imaging is being redefined by several cutting-edge technologies [Figure 9].
Role of emerging technologies in radiation protection
Ultra-low Dose Total Body PET/CT in Arthritis Evaluation
Recent first-in-human research has demonstrated the feasibility of ultra-low dose total body 18F-FDG PET/CT for systemic evaluation of autoimmune inflammatory arthritis (AIA).[29] The study, involving 30 participants and nearly 2,000 joints, showed strong concordance between PET/CT findings and standard rheumatological assessments, with particularly high agreement in osteoarthritis patients. Importantly, PET/CT identified subclinical inflammation not detected by conventional joint exams in approximately 20% of AIA cases. This technique offers a powerful tool for whole-body assessment of disease burden, treatment monitoring and biomarker development, all while maintaining a very low radiation dose, underscoring its potential in managing systemic autoimmune disorders.[30,31]
Photon-counting CT
Photon-counting detectors offer enhanced spatial resolution, reduced electronic noise and improved contrast-to-noise ratio at significantly lower doses compared to conventional energy-integrating detectors.[32] Their high efficiency allows thinner slices and better tissue discrimination—transformative for detecting subtle fractures, early osteomyelitis, or cartilage injuries.
Robotic Tele Sonography
Robotic ultrasound systems allow real-time scanning of patients at remote locations by expert radiologists, reducing the need for patient transfers and ensuring prompt imaging without radiation.[33] This is especially impactful in rural or underserved areas, as well as during pandemics or isolation mandates.
Mixed/Augmented Reality in Image-guided Interventions
By integrating CT or MRI datasets into head-mounted displays or overlay screens, these technologies allow 3D navigation during procedures like biopsies, tumour ablation, or joint injections.[34] Reduced reliance on fluoroscopy shortens procedural time and cumulative dose.
Low-field MRI Systems
Portable low-field MRI (0.2–0.6T) units offer radiation-free imaging at the bedside or outpatient setting. Although historically limited by image quality, recent improvements in coils, AI-enhanced reconstruction and faster sequences are making these units viable for routine MSK evaluations.[35–37]
Role of Audit in Radiation Protection
Radiation audits form the backbone of institutional radiation safety programs. They involve systematic assessment and documentation of all aspects of imaging practices.[38]
Adherence to DRLs
Audits verify that average patient doses for specific examinations are within national DRLs, ensuring that practices align with community standards and regulations.
Protocol Optimisation
Review of scan parameters and examination protocols helps identify outdated or suboptimal settings, allowing for updates that maintain diagnostic quality at lower doses.
Staff Training Compliance
Audits monitor whether radiologists, radiographers and referring clinicians are up to date with training in radiation protection principles and modality-specific protocols. There should be regular checks in place, with continued medical learning and retraining of the active staff with regard to the ALARA principle and its optimum utilisation. For example, the use of a mini C-arm in the orthopaedic and surgical operating theatres during various procedures should be controlled to minimise the radiation exposure to the patient, the operator, as well as the bystanders in the theatre.[39]
PPE Usage and Shielding Design
Evaluating the availability and usage rates of lead aprons, thyroid collars, mobile shields and room layout ensures both structural and behavioural safety standards are upheld.
Cumulative Dose Records for Patients
Audits should include an assessment of dose documentation systems and whether cumulative exposures are tracked for at-risk groups such as children, oncology patients, or those with chronic diseases.
Protecting Healthcare Workers in MSK Radiology
Occupational radiation safety is paramount, particularly in high-volume procedural areas. Prolonged and cumulative low-dose exposure increases risks of cataracts, thyroid disease and malignancy [Figure 10].
Lead Aprons, Thyroid Shields and Lead Glasses
These remain the first line of defence. Aprons should have a lead equivalency of 0.5 mm and be regularly inspected for cracks. Thyroid shields and glasses reduce the risk of thyroid and ocular exposure, respectively, which are among the most radiosensitive organs.
Ceiling-mounted Shielding
In fluoroscopy suites and hybrid ORs, ceiling-mounted lead acrylic panels provide effective scatter protection, especially during long procedures. Adjustable positioning ensures ergonomic benefit and optimal coverage.
Maintaining Distance from the Beam
The principle of the inverse square law applies—doubling the distance from the source quadruples the exposure. Whenever possible, staff should step away during image acquisition or use extension tools for positioning.
Real-time Dosimeter Usage
Electronic personal dosimeters (EPDs) offer instant feedback on accumulated dose, improving awareness and reinforcing safer practices in real-time. These are increasingly replacing badge-only systems.
Training in Proper Equipment Positioning
Ensuring that operators are well-versed in optimal C-arm angulation, patient positioning and beam collimation reduces both patient and staff dose. Simulation-based workshops and regular refresher courses enhance safety culture.
The ICRP limit of 20 mSv/year for effective occupational exposure must be diligently monitored, with special attention to eye lens (<20 mSv/year) and extremity (<500 mSv/year) thresholds. Robust monitoring, training and engineering controls collectively safeguard healthcare professionals.
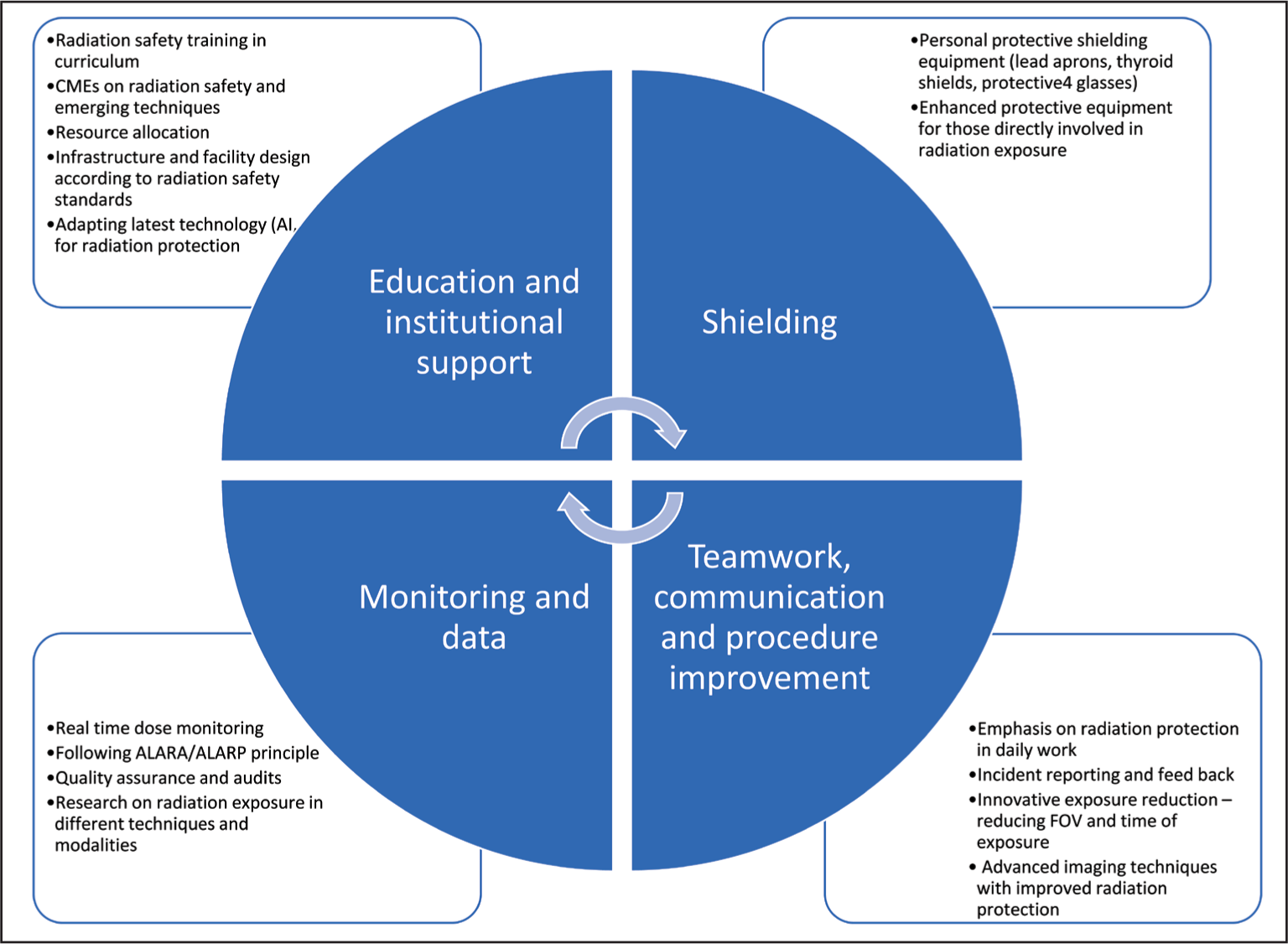
This infographic illustrates four essential pillars of radiation safety for radiology personnel:
Education and Institutional Support: Incorporating radiation safety training into curricula, offering continuing medical education (CME) on radiation safety and emerging techniques, allocating resources for radiation protection, designing infrastructure per safety standards, and adopting advanced technologies, including AI. Shielding: Use of personal protective equipment such as lead aprons, thyroid shields, and protective eyewear, and provision of enhanced protective devices for staff directly involved in radiation exposure. Monitoring and Data: Real-time dose monitoring, adherence to ALARA/ALARP principles, implementation of quality assurance and audit programs, and supporting research on radiation exposure across modalities. Teamwork, Communication and Procedure Improvement: Emphasising safety in daily workflow, incident reporting and feedback mechanisms, innovative exposure-reduction strategies (e.g., reducing field of view and exposure time), and use of advanced imaging techniques designed to minimise radiation risk.
Radiation protection hierarchy
Take-home points
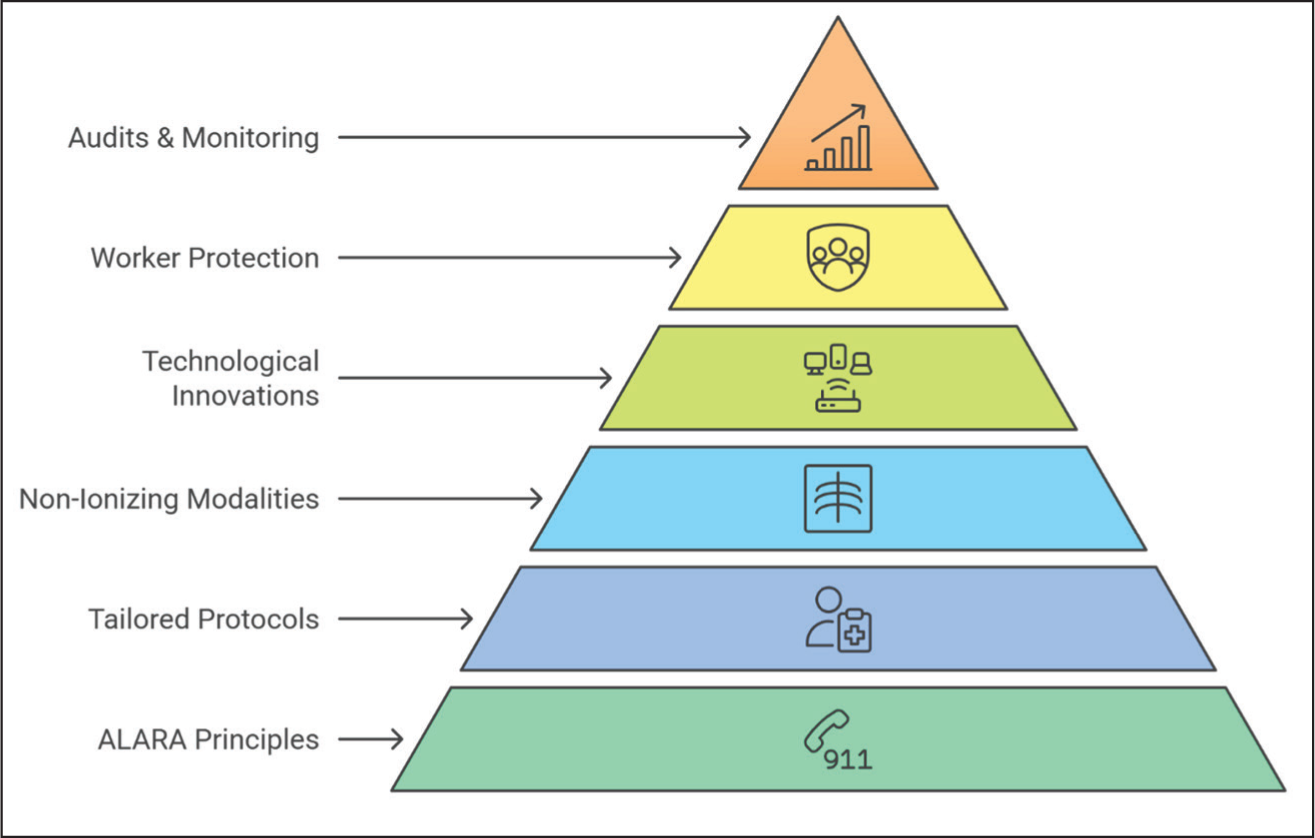
Adhering to ALARA principles remains the foundation of radiation safety in MSK radiology [Figure 11]. Paediatric, pregnant and chronic care patients require tailored imaging protocols to limit cumulative exposure. Non-ionising modalities like ultrasound and MRI should be prioritised when appropriate. Technological innovations, including low-dose CT, dual-energy CT and AI-driven protocols, are reshaping safe imaging practices. Protecting healthcare workers through appropriate shielding, audits and continuous education is essential. Regular audits and dose monitoring enhance safety for both patients and professionals.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Credit author statement
Shayeri Roy Choudhary: Conceptualization, Writing: Original Draft, Literature Review.
Tessa Kenaria: Methodology, Writing: Review & Editing, Supervision.
Jagdish Jagalpathy: Formal Analysis, Supervision, Writing: Review & Editing.
Ojasvi Vemuri: Literature Review, Data Curation.
Vishwanathan Muruhaiah: Technical Review, Writing: Review & Editing.
Vijay Ram Kumar Papineni: Conceptualization, Supervision, Writing: Review & Editing, Final Approval.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Use of artificial intelligence
No AI tools were used in the preparation of this manuscript.