
Abstract
Background:
Total knee arthroplasty (TKA) is the definitive solution for advanced knee osteoarthritis (OA). A key variable in TKA is implant design, particularly regarding posterior cruciate ligament (PCL) management. Deep-dish congruent tibial polyethylene inserts offer a design alternative to conventional cruciate-retaining (CR) and posterior-stabilised (PS) implants, providing posterior stability without femoral bone resection.
Methods:
A prospective observational study was conducted involving 42 patients undergoing primary TKA with PCL-sacrificing and deep-dish congruent tibial polyethylene implants at a tertiary care centre. Preoperative and postoperative assessments were done using the Oxford Knee Score (OKS) and Knee Society Score (KSS) at 3–6 months.
Results:
The mean OKS improved from 15.7 ± 4.2 preoperatively to 37.9 ± 4.6 at 3 months and 40.3 ± 3.8 at 6 months and 41.3 ± 4.7 at the 1-year follow-up. The KSS pain component rose from 38.8 ± 11.5 to 79 ± 4.4 and the function score increased from 36.7 ± 23.4 to 82.6 ± 12.3 by the sixth postoperative month. At the final 1-year follow-up, the overall KSS improved from 41.6 ± 7.8 to 86.9 ± 6.2. Range of motion (ROM) improved significantly from 92.3 ± 8.5° preoperatively to 118.4 ± 9.2°, with no fixed flexion deformity observed. Statistical analysis showed highly significant improvements across all outcome measures (P < .001).
Conclusions:
Deep-dish congruent polyethylene inserts in TKA offer excellent early functional and clinical results. By providing posterior stability while preserving bone, this design represents an optimal balance between CR and PS philosophies and may be especially suitable for elderly patients with deficient PCL.
Introduction
Total knee arthroplasty (TKA) remains one of the most successful orthopaedic procedures, offering consistent pain relief and improved function for patients with end-stage knee osteoarthritis (OA). Over the past few decades, significant refinements in implant design, materials and surgical techniques have improved outcomes and longevity of prostheses. One of the enduring debates in TKA design pertains to the geometry and conformity of the tibial polyethylene insert, which plays a central role in knee kinematics, implant stability and wear characteristics.[1,2]
In conventional posterior-stabilised (PS) designs, the posterior cruciate ligament (PCL) is resected and substituted by a polyethylene post-cam mechanism to provide posterior stability. However, this mechanism is associated with higher mechanical stresses and potential complications, including post-wear, breakage and mid-flexion instability.[3,4] Conversely, cruciate-retaining (CR) implants preserve the PCL, relying on native ligamentous stability. In some clinical scenarios, the PCL may be attenuated or functionally inadequate, necessitating alternative approaches without reverting to PS designs.[5]
Deep-dish or ultracongruent tibial polyethylene inserts have emerged as a viable alternative in primary TKA, particularly in cases with questionable PCL function. These inserts offer increased anterior-posterior conformity, resisting translation and mimicking the stabilising role of the PCL. Importantly, deep-dish inserts avoid the need for post-cam engagement, potentially reducing wear-related complications while maintaining kinematic fidelity.[6,7]
Although recent meta-analyses have provided comparative data, particularly supporting the safety and effectiveness of deep-dish inserts, clinical consensus remains variable and further high-quality prospective studies are needed to confirm their long-term benefits in diverse populations.[8]
There is growing evidence supporting the use of deep-dish polyethylene inserts in TKA. Multiple studies have demonstrated comparable outcomes in terms of range of motion (ROM), Knee Society Scores (KSSs) and implant survival, with some suggesting lower complication rates and reduced need for revision.[6,9] While earlier literature included many retrospective studies, there is now a growing body of prospective evidence evaluating ultracongruent inserts, including randomised and non-randomised trials reporting favourable clinical and functional outcomes.[4,9] Moreover, there is variability in surgeon preferences and institutional protocols regarding the use of deep-dish polyethylene inserts in primary TKA, often guided more by anecdotal experience than by robust clinical evidence.[10]
The present study hypothesises that the use of deep-dish congruent tibial polyethylene inserts in primary TKA yields favourable short-term clinical and functional outcomes, with low complication rates, high patient satisfaction and consistent knee stability. We posit that this insert design can safely and effectively substitute for PS or CR systems in selected patients, especially where PCL retention is uncertain but post-cam articulation is undesirable.
The clinical relevance of this study lies in its prospective design and its focus on the short-term efficacy of deep-dish inserts in routine primary TKA practice. By evaluating outcomes using validated measures such as the KSS, Oxford Knee Score (OKS) and ROM assessments, this study contributes meaningful data to guide implant selection and surgical decision-making. In addition, identifying the early complication profile and functional improvements helps refine patient counselling and expectations postoperatively.
Given the increasing adoption of deep-dish tibial inserts in modern TKA, there is an urgent need for well-conducted clinical studies that quantify their performance in real-world settings. This study, by focusing on homogenous patient groups and a consistent surgical technique, offers valuable insights into whether deep-dish polyethylene can bridge the gap between stability and longevity without the mechanical complexities of PS systems.
While Deep-dish polyethylene inserts are increasingly adopted worldwide, there is a lack of prospective clinical data, particularly from the Indian subcontinent, evaluating their functional outcomes in routine primary TKA practice. This study aims to address that gap through a focused short-term outcome analysis.
Patients and Methods
This prospective observational study was conducted at a tertiary care academic medical centre in South India between January 2020 and June 2024. Institutional ethical clearance was obtained before patient recruitment (IEC No: IEC/2020/Ortho/34) and informed written consent was secured from all participants.
A priori sample size estimation was performed using G*Power software (version X.X, University of Düsseldorf, Germany). To detect a mean difference of 8 points in the OKS, with a standard deviation of 5.6, using a paired t-test with an alpha level of 0.05 and a power of 80%, the required sample size was calculated to be approximately 15 patients. Our final sample of 42 patients (44 knees) exceeded this requirement, providing adequate statistical power to detect clinically meaningful changes in functional outcomes.
A total of 42 patients (44 knees) undergoing primary TKA with a posterior cruciate-substituting femoral component and deep-dish congruent tibial polyethylene insert were enrolled. All procedures were performed by experienced arthroplasty surgeons using a standardised medial parapatellar approach, with cemented fixation of all components.
Patients were eligible for inclusion if they were between 50 and 80 years of age, presented with advanced primary OA of the knee and were scheduled for primary TKA. Intraoperatively, all included patients had either a functionally incompetent or surgically resected PCL. Only those willing to comply with the rehabilitation protocol and attend follow-up appointments were considered.
Patients were excluded if they had a diagnosis of inflammatory arthritis, secondary OA (such as post-traumatic or post-septic arthritis) or any prior major surgery on the affected knee. Additional exclusion criteria included the presence of neuromuscular disorders affecting limb function, as well as any intraoperative requirement for constrained or hinged implants.
The study cohort consisted of 28 female and 14 male patients, with a mean age of 66.2 years (range, 54–79 years). The mean body mass index was 27.6 kg/m². All cases were diagnosed with bilateral OA; however, only staged unilateral procedures were included in the final analysis to maintain cohort uniformity.
Clinical Assessment and Follow-up
All patients underwent detailed clinical evaluation both preoperatively and postoperatively. Functional outcomes were assessed using the KSS and the OKS validated scoring systems for knee arthroplasty outcomes.[11,12] ROM was measured using a standard goniometer. Radiographic assessment was performed with weight-bearing anteroposterior and lateral radiographs to evaluate implant alignment and joint line restoration.
Postoperative assessments were conducted at 6 weeks, 3 months, 6 months and 12 months, with documentation of clinical progress, functional scores and any complications including infection, instability, thromboembolic events or need for revision. All patients followed a standard rehabilitation protocol with immediate postoperative mobilisation under physiotherapy guidance.
The surgical technique involved resection of the attenuated PCL, followed by the implantation of a PS femoral component and a congruent deep-dish tibial polyethylene insert. The patella was denervated but not resurfaced. Cement fixation was used for both femoral and tibial components.
Statistical Analysis
Data were compiled using Microsoft Excel and analysed with IBM SPSS Statistics, version 26.0 (IBM Corp., Armonk, NY). Continuous variables such as KSS, OKS and ROM were expressed as mean ± standard deviation. Comparisons between preoperative and postoperative values were performed using paired t-tests and a P value < .05 was considered statistically significant.
The study adhered to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational research. All procedures were conducted in laminar airflow operating theatres to minimise the risk of surgical site infections. Perioperative antibiotic prophylaxis and postoperative thromboprophylaxis were administered in accordance with the institutional protocol, which aligns with current evidence-based guidelines for infection prevention and venous thromboembolism prophylaxis.[13]
Results
A total of 42 patients (44 knees) who underwent primary TKA using deep-dish congruent polyethylene inserts were followed for a minimum of 12 months. The mean follow-up duration was 15.2 ± 2.8 months (range, 12–20 months).
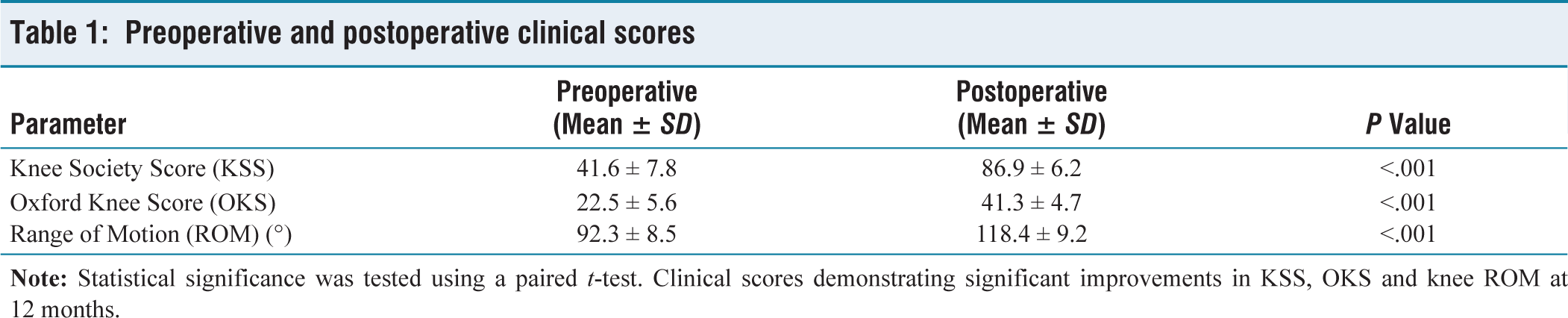
At final follow-up, significant improvements were observed in all clinical and functional parameters. The mean KSS improved from 41.6 ± 7.8 preoperatively to 86.9 ± 6.2 postoperatively (P < .001) and the OKS improved from 22.5 ± 5.6 to 41.3 ± 4.7 (P < .001). The mean knee flexion increased from 92. ± 8.5° preoperatively to 118.4 ± 9.2° postoperatively (P < .001).
The comparison of preoperative and postoperative functional scores is summarised in Table 1, demonstrating statistically significant improvements in KSS, OKS and ROM at the final follow-up (P < .001 for all).
Preoperative and postoperative clinical scores
Subgroup analysis revealed that patients under the age of 65 had slightly higher postoperative KSS and OKS scores compared to older patients, though the difference was not statistically significant (P = .08). Gender-based comparisons showed no significant difference in outcomes between male and female patients (P = .42).
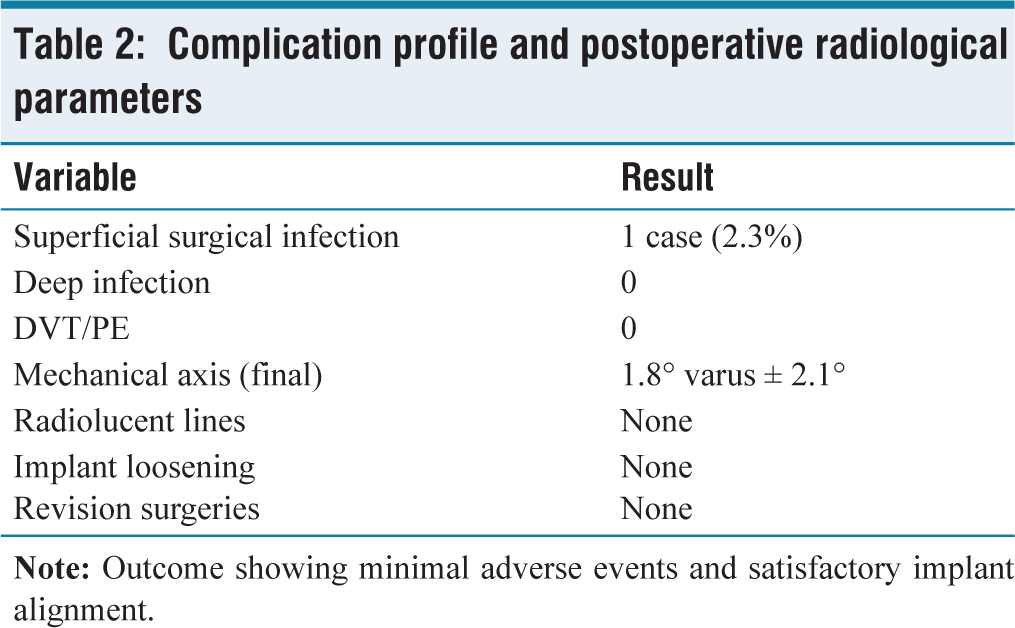
Radiographic evaluation demonstrated satisfactory alignment and component positioning in all cases. There were no cases of radiolucent lines or loosening at 1 year. No significant alterations in joint line level were observed postoperatively and tibiofemoral alignment was restored to a mean mechanical axis deviation of 1.8 ± 2.1° varus.
Postoperative complications were minimal. One patient (2.3%) developed a superficial surgical site infection, managed successfully with antibiotics and dressings. There were no cases of deep infection, instability, deep vein thrombosis or revision surgery during the study period. Postoperative radiographic assessments and complications are detailed in Table 2, showing satisfactory alignment in all cases and a low incidence of minor adverse events.
Complication profile and postoperative radiological parameters
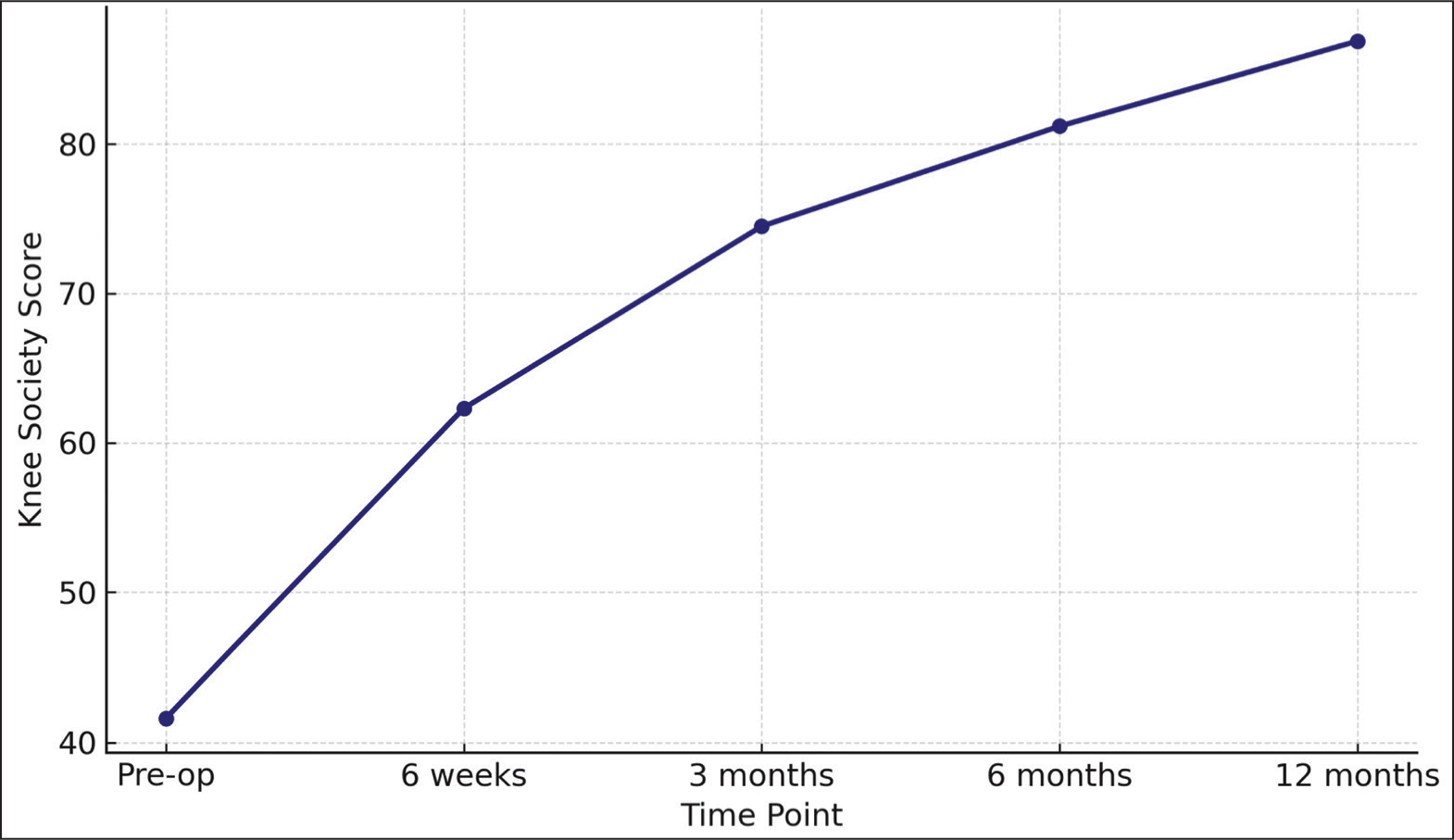
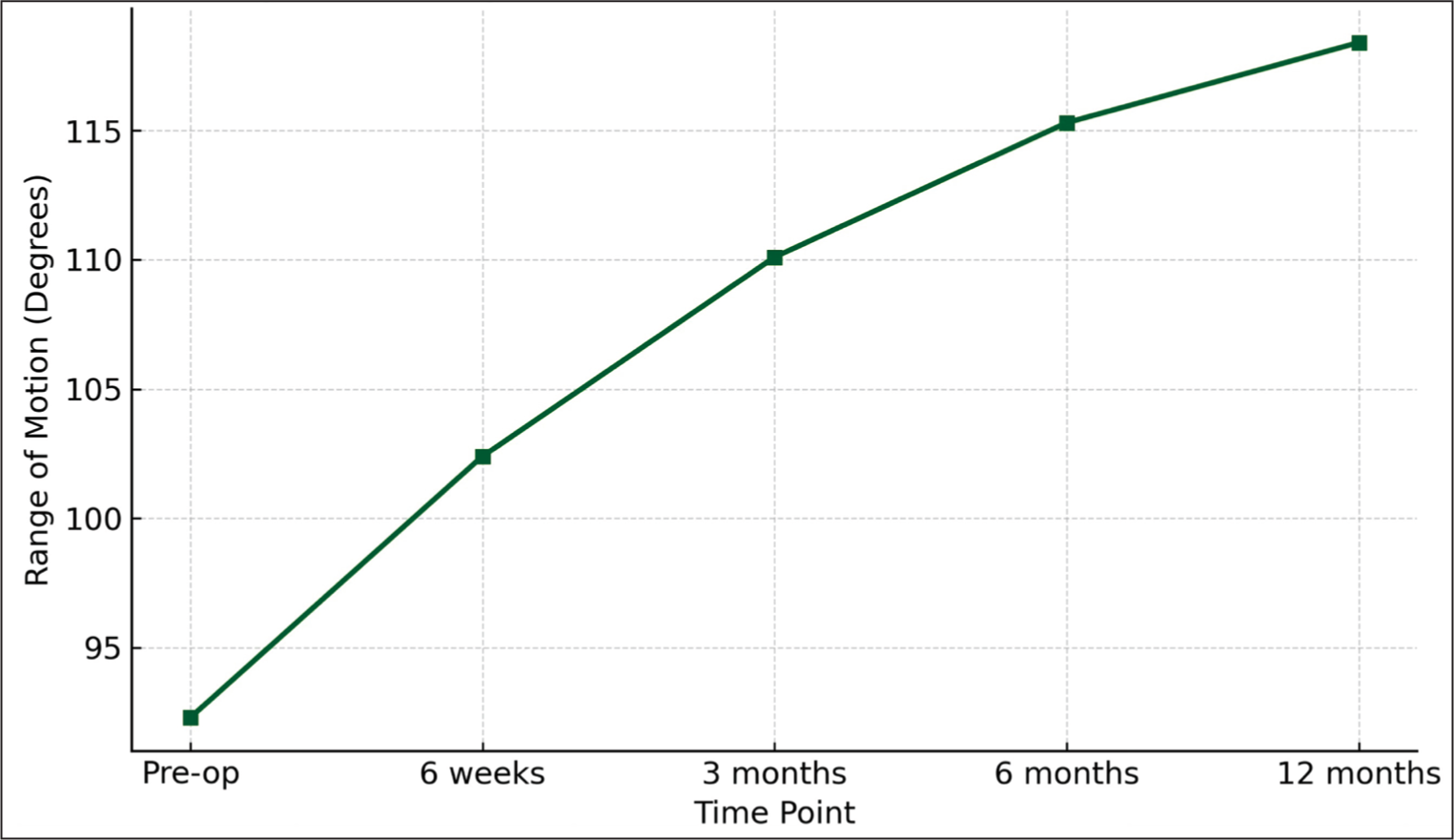
Serial follow-up at 6 weeks, 3 months, 6 months and 12 months showed a steady progression in function and ROM. The trajectory of mean KSS and knee flexion over time is depicted in Figures 1 and 2, respectively.
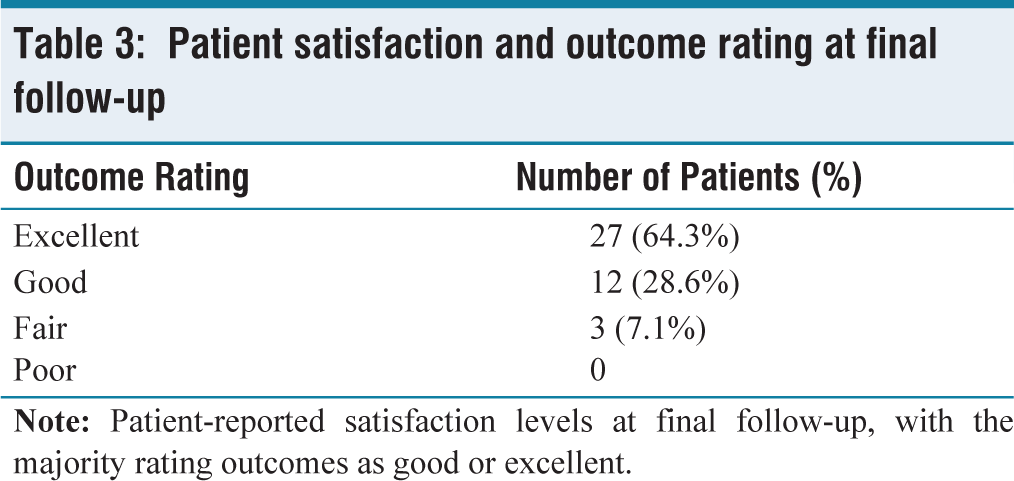
The majority of patients (39 out of 42 or 92.9%) rated their surgical outcome as either ‘excellent’ or ‘good’ and reported satisfaction with knee function during activities of daily living. Three patients rated their result as ‘fair,’ citing residual discomfort during stair climbing, although their objective scores remained within satisfactory limits. Patient-reported satisfaction outcomes at 12 months are presented in Table 3, with the majority (92.9%) rating their functional outcome as good or excellent.
Patient satisfaction and outcome rating at final follow-up
These results highlight the value of deep-dish polyethylene inserts in achieving favourable short-term functional outcomes, high levels of patient satisfaction and a low incidence of complications in primary TKA, especially where PCL integrity is compromised.
Discussion
TKA remains the gold standard treatment for end-stage OA, offering substantial pain relief and improved function.[14,15] However, optimising implant design to enhance joint stability and longevity remains a key focus. The deep-dish congruent tibial polyethylene component, designed to improve conformity and constrain instability, particularly in cases of PCL insufficiency, has shown biomechanical promise.[16,17] Although studies by Lützner et al.[4] and Wenzel et al.[6] have contributed valuable prospective and meta-analytic data on the functional outcomes and safety of ultracongruent inserts, additional high-quality research is required to establish their long-term durability across diverse patient populations.
This prospective study aimed to elucidate the short-term clinical and functional results of this implant design in primary TKA. Our findings demonstrated significant improvements in KSS and OKS, increasing from mean preoperative values of 41.6 and 22.5 to 86.9 and 41.3, respectively, at 12 months (P < .001).
Our results align with prospective findings by Lützner et al.[4] who reported equivalent outcomes between ultracongruent and PS inserts in a randomised controlled trial, as well as Carlson et al.[9] who demonstrated superior 2-year functional outcomes using ultracongruent inserts compared to CR and PS designs.
Similarly, knee flexion improved significantly from 92.3° to 118.4°, consistent with literature suggesting that increased conformity does not impede postoperative ROM.[18,19]
High patient satisfaction rates (92.9% rating outcomes as good or excellent) underscore the clinical relevance of these objective improvements. Patient satisfaction post-TKA is multifactorial, often influenced by pain relief, functional recovery and stability.[20] The deep-dish design likely contributes to improved subjective outcomes through enhanced anteroposterior and mediolateral stability, as supported by biomechanical studies demonstrating reduced laxity and wear with congruent inserts.[21,22]
When compared to other implant designs, particularly PS and CR components, our data suggest that deep-dish polyethylene inserts may offer distinct advantages. Biomechanical studies, such as that by Grupp et al.[23], suggest that non-congruent designs may be prone to increased polyethylene wear and altered kinematics, which are established factors associated with instability and revision in clinical settings, whereas our study found no radiographic evidence of implant loosening or radiolucent lines, supporting improved mechanical stability. [24] Additionally, complication rates in our cohort were low, with only a single superficial infection and no deep infections or thromboembolic events, which compares favourably with large joint registry data.[25,26]
Statistical analysis confirmed that the improvements in clinical scores and ROM were highly significant (P < .001), affirming the implant’s efficacy. The consistency of outcomes across age and gender subgroups suggests broad applicability, though larger studies are warranted to explore these variables further. Importantly, the postoperative functional scores exceed minimal clinically important difference (MCID) thresholds reported in recent meta-analyses, reinforcing the clinical benefit of this design.[27]
Furthermore, the improvements observed in patient-reported outcomes such as the OKS (mean increase of 18.8 points) and KSS exceeded the MCID thresholds reported in the literature, indicating that these statistically significant changes were also clinically meaningful from the patient’s perspective.[27]
Our study’s strengths include its prospective design, standardised follow-up schedule and comprehensive outcome assessment encompassing clinical, functional and radiological parameters. Unlike retrospective or registry-based studies that often lack uniformity, our serial assessments at 6 weeks, 3 months, 6 months and 12 months provide a detailed recovery trajectory. Furthermore, focusing on a homogeneous patient group receiving the same deep-dish polyethylene implant reduces confounding factors commonly encountered in comparative studies.
Although the use of deep-dish polyethylene inserts is not novel and has been well established in various implant systems, our study adds value by presenting prospective clinical outcome data from a real-world setting using a consistent technique. Such evidence is especially relevant in regions where literature is sparse and implant selection remains guided largely by anecdotal experience rather than published outcomes.
This study has certain limitations that merit consideration. The follow-up duration of approximately 1 year is relatively short and may not capture long-term implant survival, late-onset complications such as aseptic loosening or osteolysis or the progression of polyethylene wear, issues that typically emerge after 5 years.[28] Although the sample size of 42 patients (44 knees) was determined through a priori power analysis and proved adequate for detecting significant differences in key functional outcomes such as OKS, it remains modest. This restricts the ability to identify rare complications or conduct robust subgroup and multivariate analyses. Furthermore, the absence of a control group using alternative polyethylene insert designs limits direct comparative insights into the relative clinical and economic advantages. Future research involving larger, multicentre cohorts with extended follow-up periods is necessary to confirm and build upon the present findings.
Future investigations should focus on extended follow-up to evaluate implant durability and wear characteristics through radiostereometric analysis or advanced imaging. Multicentre randomised controlled trials comparing deep-dish inserts with other designs would further clarify their relative benefits and limitations. Additionally, patient-reported outcome measures could be supplemented with gait analysis and biomechanical assessments to elucidate functional differences more objectively.
In conclusion, this study provides consistent early evidence that primary TKA with deep-dish congruent tibial polyethylene components results in encouraging short-term clinical and functional outcomes, high patient satisfaction and minimal complications. The implant’s design features appear to enhance stability without compromising ROM, potentially reducing polyethylene wear and revision risk. While longer-term data are essential, these findings support the use of deep-dish polyethylene inserts as a valuable option in modern knee arthroplasty practice.
Conclusion
This study demonstrates that the use of deep-dish congruent tibial polyethylene components in primary TKA yields significant short-term improvements in clinical function, ROM and patient satisfaction, with minimal complications. The implant’s enhanced conformity appears to provide superior joint stability without compromising mobility, potentially reducing polyethylene wear and risk of early revision. Deep-dish polyethylene inserts may represent a promising option in contemporary knee arthroplasty practice, contributing to improved patient outcomes and implant longevity. However, these findings are encouraging; future randomised controlled trials and comparative studies with larger sample sizes and longer follow-up are essential to validate these early outcomes and establish long-term efficacy and durability.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The approval was granted by the Institutional Ethical Committee at Government Medical College Kozhikode with approval number IEC/2020/Ortho/34.
Informed consent
Informed written consent was obtained from all participants in their native language.
Credit author statement
Data Curation: Collected and maintained clinical, radiological and functional data. Investigation: Actively participated in surgeries, postoperative follow-up and documentation. Writing, Original Draft: Drafted the manuscript, including methods, results and preliminary discussion. Project Administration: Coordinated ethical approvals, patient consent and regulatory documentation.
Supervision: Provided overall scientific and clinical oversight. Methodology: Designed surgical technique standardisation and follow-up protocol. Validation: Independently reviewed data and verified analytical interpretations. Writing, Review and Editing: Substantively revised the manuscript for intellectual and scientific accuracy. Final Approval: Reviewed and approved the final manuscript and is accountable for all aspects of the study.
Conceptualisation: Formulated the study hypothesis and defined study objectives. Investigation: Supported surgical execution and intraoperative documentation. Data Validation: Verified radiographic measurements and cross-checked functional scores. Literature Review: Conducted a comparative review of prior studies for inclusion in the discussion. Writing Support: Assisted in editing the introduction and discussion sections.
Software and Statistical Support: Supported SPSS-based data entry and repeated measures analysis. Referencing: Formatted citations and ensured compliance with Vancouver style. Visualisation: Generated data graphs and assisted with figure design and formatting.
All authors meet the ICMJE authorship criteria. They have read and approved the final manuscript, contributed meaningfully to the work and agreed to be accountable for all aspects of the manuscript. The authors declare that the manuscript is original, has not been previously published and is not under consideration elsewhere.
Data availability
The data that support the findings of this study are not publicly available due to restrictions imposed by the institutional ethical review board/committee. They may be available from the corresponding author upon reasonable request and with permission from the institutional ethics committee.
Use of artificial intelligence
We confirm that Artificial Intelligence (AI) tools, including ChatGPT (OpenAI), were used to assist in language refinement, grammar correction and formatting of the manuscript. However, all clinical content, interpretation of data, analysis and conclusions were entirely conceived, validated and approved by the authors. The authors take full responsibility for the integrity, originality and accuracy of the scientific content.
No AI tools were used for data analysis, data generation or in the writing of patient-related clinical observations or results.