
Abstract
Background:
Artificial intelligence (AI) is transforming surgical gastroenterology by enabling data-driven precision across the preoperative, intraoperative and postoperative continuum. This review aims to synthesise recent advances and evaluate the clinical applicability of AI-powered platforms in gastrointestinal (GI) surgery.
Objectives:
To provide a comprehensive overview of AI integration in surgical gastroenterology between 2015 and 2025, focusing on predictive analytics, intraoperative guidance, postoperative surveillance, implementation challenges and the Indian context.
Methods:
A narrative review was conducted using the PubMed, Scopus and Web of Science databases. Studies published between January 2015 and May 2025 were included. AI domains covered include machine learning (ML), deep learning (DL), natural language processing (NLP), computer vision and augmented reality (AR). Only peer-reviewed, English-language articles relevant to surgical GI practice were selected.
Results:
AI models have demonstrated superior accuracy over traditional scoring systems in predicting anastomotic leaks (ALs), readmissions and postoperative liver failure. Intraoperatively, real-time computer vision platforms enable anatomical recognition, tool tracking and perfusion analysis. Postoperative monitoring systems, such as FluidAI and MySurgeryRisk, provide early complication alerts through multimodal data integration. Despite the promise, challenges persist, including data heterogeneity, limited external validation, algorithmic bias and regulatory ambiguity. A tailored roadmap for Indian healthcare outlines priorities in dataset development, ethics frameworks and capacity building.
Conclusion:
AI is poised to augment decision-making and improve outcomes in surgical gastroenterology. Its successful adoption depends on equitable data access, transparent algorithms and surgeon-led innovation, particularly in resource-diverse settings such as India.
Keywords
Introduction
Over the last decade, artificial intelligence (AI) has transformed from an experimental novelty into a disruptive force in surgical gastroenterology. Complex gastrointestinal (GI) surgeries, ranging from colorectal resections to hepatopancreatic procedures, demand intricate decision-making across the preoperative, intraoperative and postoperative continuum. Traditional clinical tools, including risk calculators and scoring systems, often rely on linear statistical models and a limited array of variables, rendering them inadequate in the face of nonlinear patient data and dynamic intraoperative environments.[1,2]
AI, encompassing machine learning (ML), deep learning (DL), natural language processing (NLP) and computer vision, offers an unprecedented ability to process high-dimensional data streams from clinical records, imaging, operative videos and sensor-based feeds.[3,4] By learning complex, multivariate associations, AI-driven algorithms can predict surgical outcomes, support intraoperative navigation, personalise postoperative surveillance and even assist in surgical training.[5,6] For instance, AI models have demonstrated superior accuracy in forecasting anastomotic leaks (ALs) and postoperative complications compared to conventional methods, while augmented reality (AR) and real-time video analytics now facilitate anatomical guidance and instrument tracking in real-time.[7,8]
Despite its promise, the integration of AI into surgical gastroenterology faces several challenges, including data heterogeneity, lack of external validation, ethical considerations and regulatory ambiguity.[9] Additionally, questions remain regarding the interpretability and generalisability of AI-driven skill assessment models in real-world surgical education settings.[10] Nonetheless, the rapidly expanding body of high-quality evidence signals a paradigm shift toward data-informed, algorithm-enhanced GI surgery.
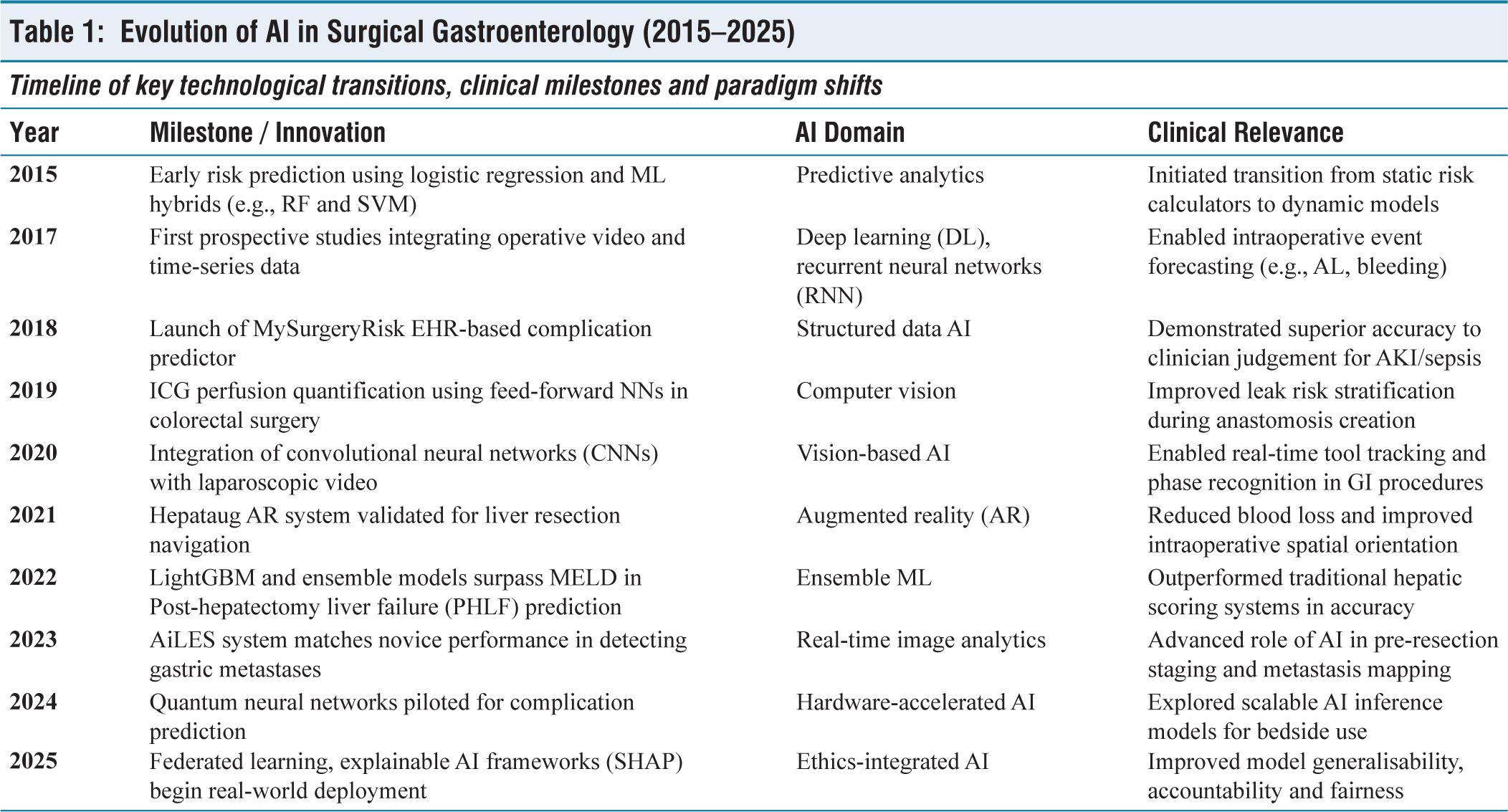
A timeline of key milestones highlighting the transformation of AI in surgical gastroenterology over the last decade is summarised in Table 1.
Evolution of AI in Surgical Gastroenterology (2015–2025)
This narrative review aims to synthesise key developments in AI applications for surgical gastroenterology between 2015 and 2025.
We examine five pivotal domains: (a) Predictive analytics for perioperative decision-making, (b) intraoperative AI for navigation and decision support, (c) postoperative complication monitoring, (d) AI-enhanced surgical education and (e) translational challenges and future directions. By critically evaluating both the technological evolution and clinical validation of these innovations, we offer a consolidated reference point for clinicians, researchers and policymakers navigating the AI-enabled surgical frontier.
Methods
This narrative review was conducted in accordance with the scale for the assessment of narrative review articles (SANRA) guidelines. A literature search was performed using PubMed, Scopus and Web of Science databases to identify relevant publications from January 2015 to May 2025. Search terms included combinations of ‘AI,’ ‘ML,’ ‘DL,’ ‘computer vision,’ ‘surgical gastroenterology,’ ‘predictive analytics’ and ‘AR’. Only peer-reviewed, English-language studies were considered. Reference screening and inclusion prioritisation were guided by clinical relevance, technical rigour and surgical applicability.
Predictive Analytics in Surgical Gastroenterology
The preoperative and perioperative phases in GI surgery are fraught with uncertainty, ranging from patient selection to predicting complications. AI, particularly ML and DL, has enabled a shift from static risk stratification to dynamic, individualised prognostication. AI-driven models now utilise multidimensional datasets including laboratory trends, operative timings, radiomics and sensor data to estimate postoperative outcomes with increasing precision.
In colorectal surgery, the prediction of AL has been a cornerstone application. A multicentre analysis of AI models, including random forests and neural networks, reported area under the receiver operating characteristic curve (AUROC) up to 0.83 across institutional datasets, though external validation often revealed performance drops, highlighting the challenge of model generalisability.[11] AI models integrating auto-selection of circular stapler types and perfusion maps using indocyanine green (ICG) with feed-forward neural networks improved AL prediction accuracy to an AUROC of 0.774 by incorporating real-time operative features.[12]
Beyond binary outcome forecasting, AI is being used for unsupervised clustering of postoperative complications. A meta-analysis of 38 studies between 2015 and 2022 found that ML methods improved mean area under the curve (AUC) by 0.07 compared to traditional regression-based models for endpoints such as 30-day readmission and postoperative ileus.[13] For example, a support vector machine (SVM) model using postoperative day three C-reactive protein (CRP), length of stay and creatinine levels achieved an AUROC of 0.784 for readmission, outperforming conventional multilayer perceptrons.[14]
In gastric cancer surgery, hybrid convolutional neural network (CNN)-Transformer models have demonstrated 90% accuracy in recognising surgical phases, enabling predictive guidance for intraoperative events such as vessel control or stapler deployment.[15] Similarly, in pancreatic surgery, gradient boosting methods have surpassed logistic regression in predicting futile pancreaticoduodenectomy, defined as death within 12 months, achieving an AUROC of 0.689 versus 0.679.[16] Clinically relevant postoperative pancreatic fistulas have also been predicted using ensemble radiomics and DL models with an AUROC of 0.759.[17]
Hepatic procedures have witnessed a parallel evolution. A LightGBM-based risk model developed on 935 patients achieved an AUROC of 0.812 (95% CI, 0.791–0.853) in predicting post-hepatectomy liver failure, outperforming model for end-stage liver disease (MELD) and albumin-bilirubin index (ALBI) scores.[18] Meanwhile, DL models analysing surveillance imaging and laboratory data have achieved concordance indices as high as 0.83 for five-year hepatocellular carcinoma (HCC) recurrence, well above traditional Cox models.[19]
In bariatric surgery, SVMs leveraging perioperative laboratory parameters have shown promise in forecasting 30-day readmission, reaching an AUROC of 0.784 in large-scale US datasets.[20]
A comparative overview of organ-specific AI models, including outcomes, algorithmic performance and validation status, is provided in Table 2.
Representative predictive AI models in GI surgery (2015–2025)
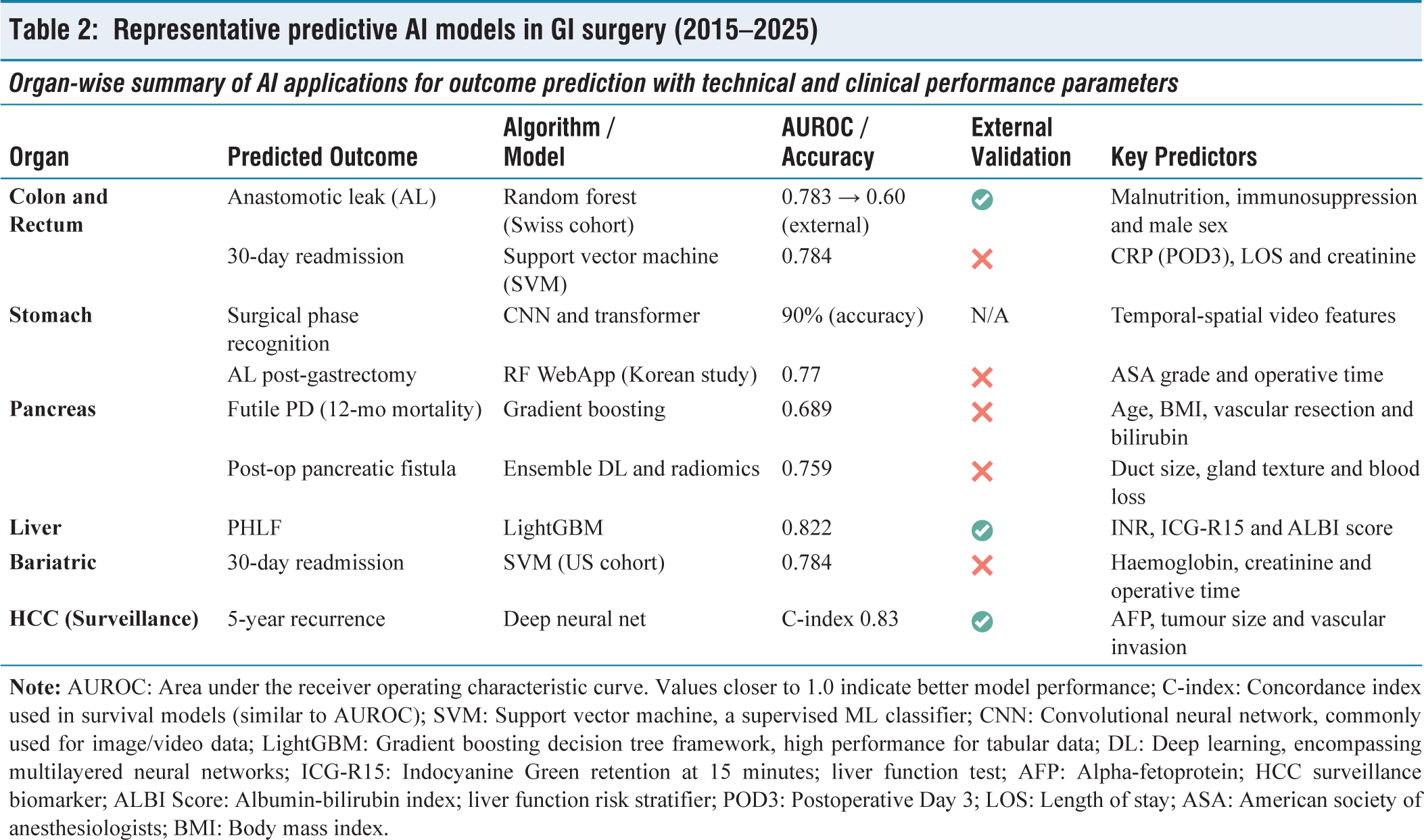
These advances underscore AI’s transition from theoretical modelling to clinical toolkits. Yet, a common limitation remains the lack of multicentre validation, which often leads to reduced accuracy outside the development cohort. Bridging this gap will be key to translating predictive analytics into daily surgical decision-making.
Intraoperative AI and Computer Vision in GI Surgery
The intraoperative environment presents a high-stakes, time-critical landscape where real-time decision-making can significantly alter outcomes. AI, particularly computer vision and AR, is increasingly being deployed in GI surgery to enhance anatomical recognition, optimise tool handling and support surgical judgement. These systems leverage live video, sensor fusion and trained neural networks to provide immediate actionable insights within the sterile field.
In hepatic surgery, AR platforms such as Hepataug overlay 3D tumour reconstructions onto the surgeon’s laparoscopic view. In one validation, physics-based deformation mapping using red-green-blue plus depth camera input (RGB-D) sensors achieved a mean projection error of just 9.2 mm, compared to 29.4 mm with traditional laparoscope-axis alignment.[6] The clinical relevance of these overlays is underscored by reductions in transfusion rates and operative time.[21]
AR’s utility has also been explored in pancreaticoduodenectomy, where systems such as augmented reality–assisted autonomic nerve segmentation (AR-ANS) enabled manual 3D holographic reconstructions to assist with margin identification and vascular orientation. A pilot study found AR integration correlated with a 35% reduction in intraoperative blood loss, although quantitative error metrics were not uniformly reported.[22]
In colorectal surgery, perfusion assessment is an established predictor of anastomotic integrity. A quantitative AI model analysing ICG fluorescence angiography enabled accurate perfusion classification and leak prediction, marking a significant advance in intraoperative assessment.[23]
Autonomic nerve preservation during pelvic dissection is another domain where AI has proven advantageous. DL-based segmentation of nerve plexuses during laparoscopic colorectal surgery achieved a Dice coefficient of 0.56, with earlier recognition than the operating surgeon in 50% of reviewed cases.[24]
Tool tracking and segmentation have also advanced, with AI platforms capable of recognising multiple instruments and actions in real-time surgical video. A 2,024 systematic review summarised these efforts, emphasising improved detection accuracy, real-time processing and validation across real-world datasets.[25]
Fluorescence-based perfusion evaluation has now reached randomised trial validation. In the Indocyanine Green–Enhanced Colorectal Angiography Trial (ICG-COLORAL) trial, AI-enhanced fluorescence imaging significantly reduced the rate of ALs in colorectal surgery by improving intraoperative tissue viability assessment.[26]
Meanwhile, platforms such as AI laparoscopic exploration system (AiLES) have shown promise in metastasis detection during gastric staging laparoscopy, matching novice performance while operating at 11 frames per second.[27]
In robotic surgery, total tool motion extracted from console data correlates strongly with surgical efficiency, with Pearson coefficients of −0.72 in simulation environments.[28] CNNs trained on kinematic profiles distinguish expert from novice performance with >97% accuracy, offering potential for standardised, automated skill assessment.
Final, reinforcement learning (RL) is emerging for semi-autonomous tasks. Systems optimised through RL have demonstrated reduced force application and enhanced accuracy in robotic suturing, hinting at the future of intelligent surgical automation.[29]
The major intraoperative AI systems in current surgical practice, along with their modalities, functionality and technical performance, are outlined in Table 3.
Intraoperative AI systems in gastrointestinal surgery
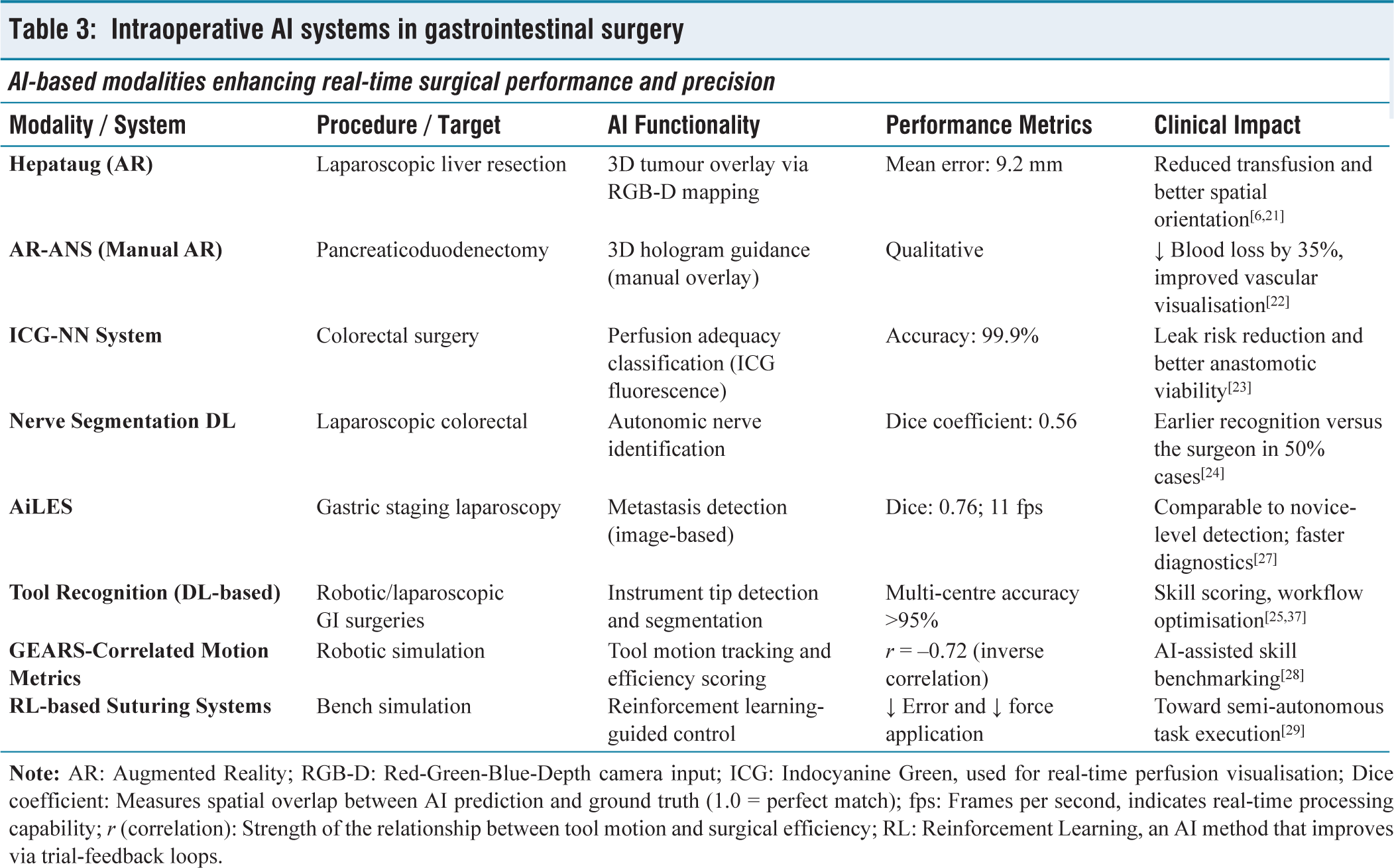
These innovations collectively suggest that intraoperative AI is rapidly evolving from an assistive modality to a context-aware co-surgeon, redefining precision in GI s urgery.
Postoperative Monitoring and ‘Surgomics’
The postoperative phase remains one of the most unpredictable and resource-intensive components of GI surgery. Traditional surveillance protocols often rely on clinical suspicion, delayed imaging or reactive laboratory markers. AI introduces a proactive paradigm, where continuous data streams from surgical drains, vital signs and electronic health records (EHR) are leveraged to forecast complications such as ALs, surgical site infections and multi-organ dysfunction.
Among the most innovative tools is the FluidAI Stream™ platform, which integrates biochemical analysis of drain effluent with ML algorithms to flag ALs up to six days before clinical signs emerge. This early warning system has enabled both pre-emptive interventions and expedited discharge in low-risk patients.[30]
Complementing biochemical analysis is an EHR-integrated AI platform developed by Xu et al. which has shown AUROCs exceeding 0.85 for predicting sepsis, acute kidney injury and respiratory failure in postoperative patients.[31] By continuously updating predictions based on real-time data, such systems embody the emerging field of ‘surgomics’, the extraction of high-dimensional phenotypes from perioperative environments.
Quantum neural networks are being trialled for postoperative complication forecasting, offering comparable accuracy to classical models but with improved computational efficiency and adaptability.[32] Though still in early-stage validation, they may enable bedside-level AI deployment using compact, edge-optimised hardware.
Multisensor integration is also advancing. Systems combining drain chemistry, thermal imaging and wearable biosensors have been shown to identify early signs of sepsis or wound dehiscence within 48 hours of surgery, well before standard monitoring would trigger concern.[33] These platforms rely on feature fusion, where structured (laboratories, vitals) and unstructured data (free-text progress notes) are combined through DL to improve predictive power.[33,35]
A prospective study by Nema and Vachhani demonstrated that integrating EHR data streams with NLP of operative notes improved the accuracy of predicting readmissions and delayed complications in pancreatic surgery.[34] In parallel, AI-powered video analytics have also been used to flag intraoperative events predictive of postoperative complications, offering another layer of surveillance based on real-time behaviour analysis.[35]
Importantly, AI not only detects deviations but helps define ‘normal’ recovery. A recent study mapped ideal postoperative trajectories across various GI procedures, creating dynamic baselines against which individual recovery curves could be compared. When embedded in clinical workflows, these baselines provided early alerts for outliers, prompting targeted follow-up.[36] Recent advancements in real-time laparoscopic video analysis further emphasise the role of DL in instrument tracking, activity recognition and anomaly prediction.[37,38]
Despite the promise, implementation remains limited by data silos, inconsistent documentation practices and privacy concerns. However, with the rise of federated learning models and real-time data interoperability standards, these barriers are gradually being eroded. Meanwhile, deep RL continues to evolve as a method for optimising postoperative pathways and autonomous clinical decision support systems.[39]
Collectively, AI-enabled postoperative monitoring transforms passive recovery into active surveillance, enabling earlier rescue, personalised follow-up and data-informed discharge planning.
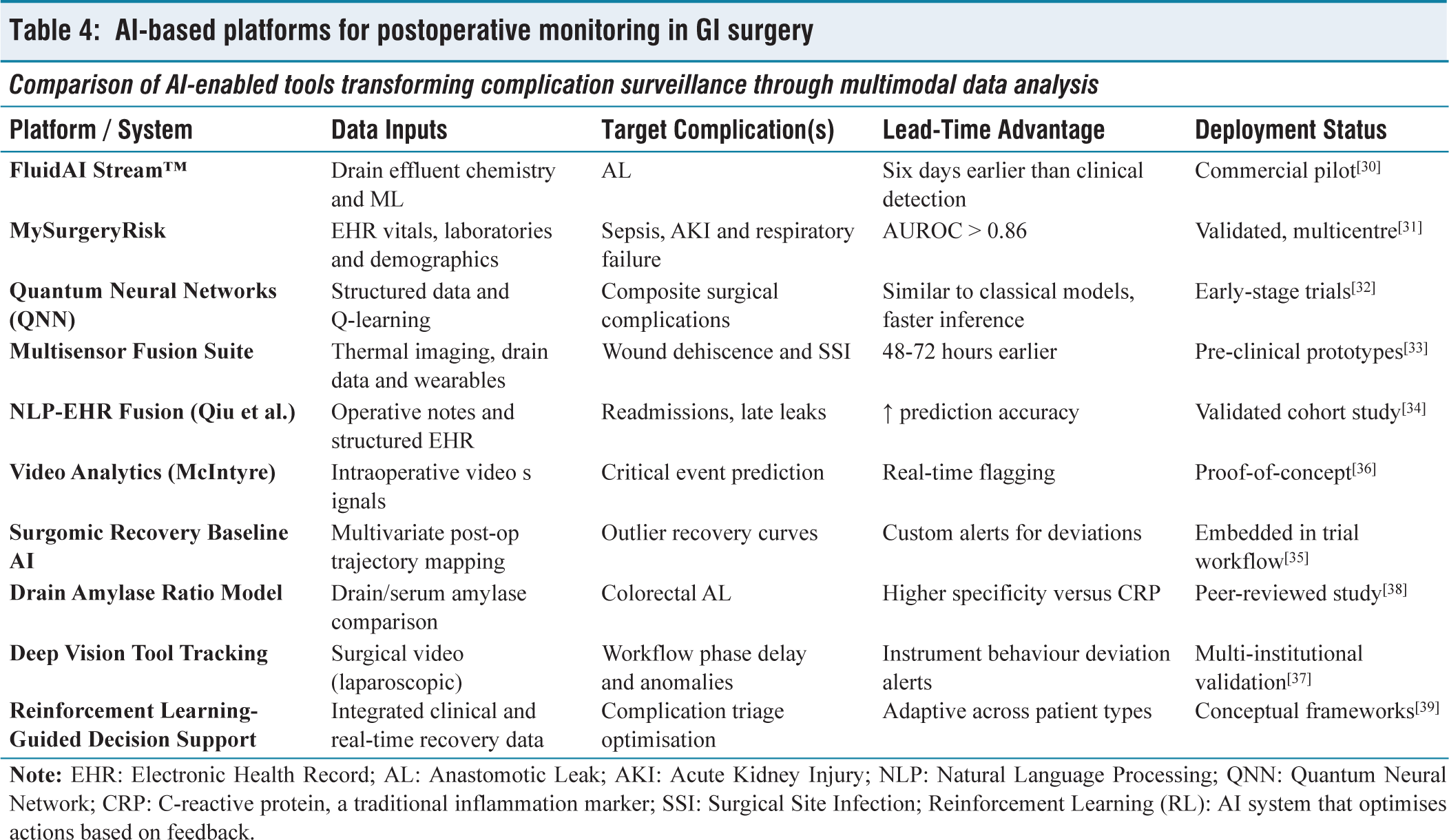
A summary of AI platforms enhancing postoperative surveillance, their data sources, clinical targets and readiness levels is presented in Table 4.
AI-based platforms for postoperative monitoring in GI surgery
Implementation Challenges, Ethical Considerations and Regulatory Frameworks
Despite the accelerating momentum of AI in GI surgery, real-world implementation faces formidable challenges. These span from technical constraints and legal ambiguities to ethical dilemmas and regulatory inertia. As AI transitions from prototype to clinical co-pilot, addressing these barriers is essential for safe equitable integration.
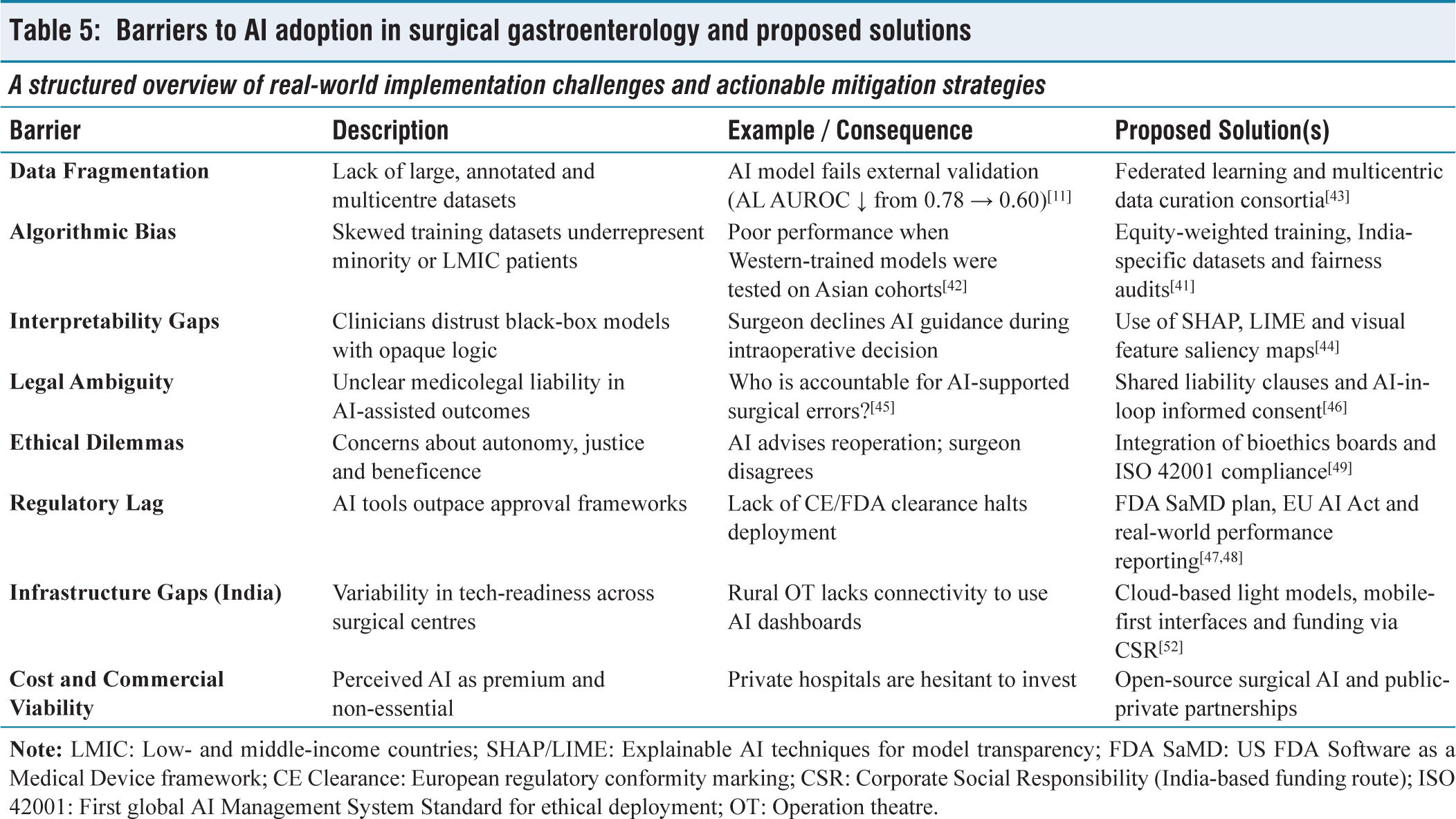
Data heterogeneity and quality remain major obstacles. Surgical datasets are often institution-specific, poorly annotated and fragmented across information silos. External validation of AI models remains rare; a review of 98 surgical AI studies found that only 27% underwent out-of-sample testing.[40] Consequently, many algorithms suffer from performance decay when deployed outside their training context.
Bias and fairness concerns are intrinsic to AI models. When training data underrepresents certain demographics, such as patients with atypical anatomy, low-resource settings or rare complications, models may perpetuate healthcare disparities.[41] For instance, performance drops have been observed when AI tools trained in high-income Western centres are tested on Asian or African cohorts.[42] Federated learning has emerged as a viable strategy to mitigate bias, enabling model training across institutions without centralised data sharing.[43]
Interpretability is another key barrier to clinician trust. Black-box models often fail to provide an understandable rationale for their predictions. Recent developments in explainable AI (XAI) frameworks, such as SHapley Additive exPlanations (SHAP) and local interpretable model-agnostic explanations (LIME), allow for feature importance mapping, but remain underutilised in surgical AI studies.[44] Transparency is particularly vital in high-risk scenarios such as resection planning or complication triage.
Legal liability and accountability are unresolved. If an AI-assisted decision leads to harm, determining responsibility, whether surgeon, institution or algorithm developer, remains unclear. Current medicolegal frameworks do not yet account for partial or shared autonomy in surgical tasks.[45] Proposed solutions include audit trails, traceable model decisions and shared responsibility clauses in informed consent.[46]
Regulatory clarity is gradually evolving. In 2021, the US FDA released an action plan for AI-based software as a medical device (SaMD), emphasising real-world performance monitoring, transparency and algorithm retraining protocols.[47] Similarly, the European Union’s (EU’s) Medical Device Regulation and upcoming AI Act are introducing classification tiers and audit mandates for high-risk AI systems.[48]
Final, ethical principles such as autonomy, justice and beneficence must remain central. AI models that recommend reoperation, palliative pathways or early discharge carry significant moral weight. Embedding bioethical oversight into model development and deployment through frameworks such as the International Organization for Standardization / International Electrotechnical Commission (ISO/IEC) 42001 AI governance standard will be essential.[49]
A strategic matrix of current implementation barriers in surgical AI, along with real-world examples and mitigation pathways, is compiled in Table 5.
Barriers to AI adoption in surgical gastroenterology and proposed solutions
To ensure responsible adoption, GI surgeons must evolve into informed AI consumers. This includes advocating for transparent algorithms, contributing to multicentre datasets and participating in the co-design of surgical AI systems that reflect real-world complexity.
Future Directions and the Indian Context
As AI systems continue to mature, their role in surgical gastroenterology will expand from decision support to collaborative execution. Multimodal ‘digital twins’, integrating imaging, operative video, sensor data and outcomes, are poised to simulate patient-specific pathways and optimise intraoperative choices.[50] RL, based microtasks, such as camera navigation or suction control, are already demonstrating reduced surgeon workload in simulation environments.[51]
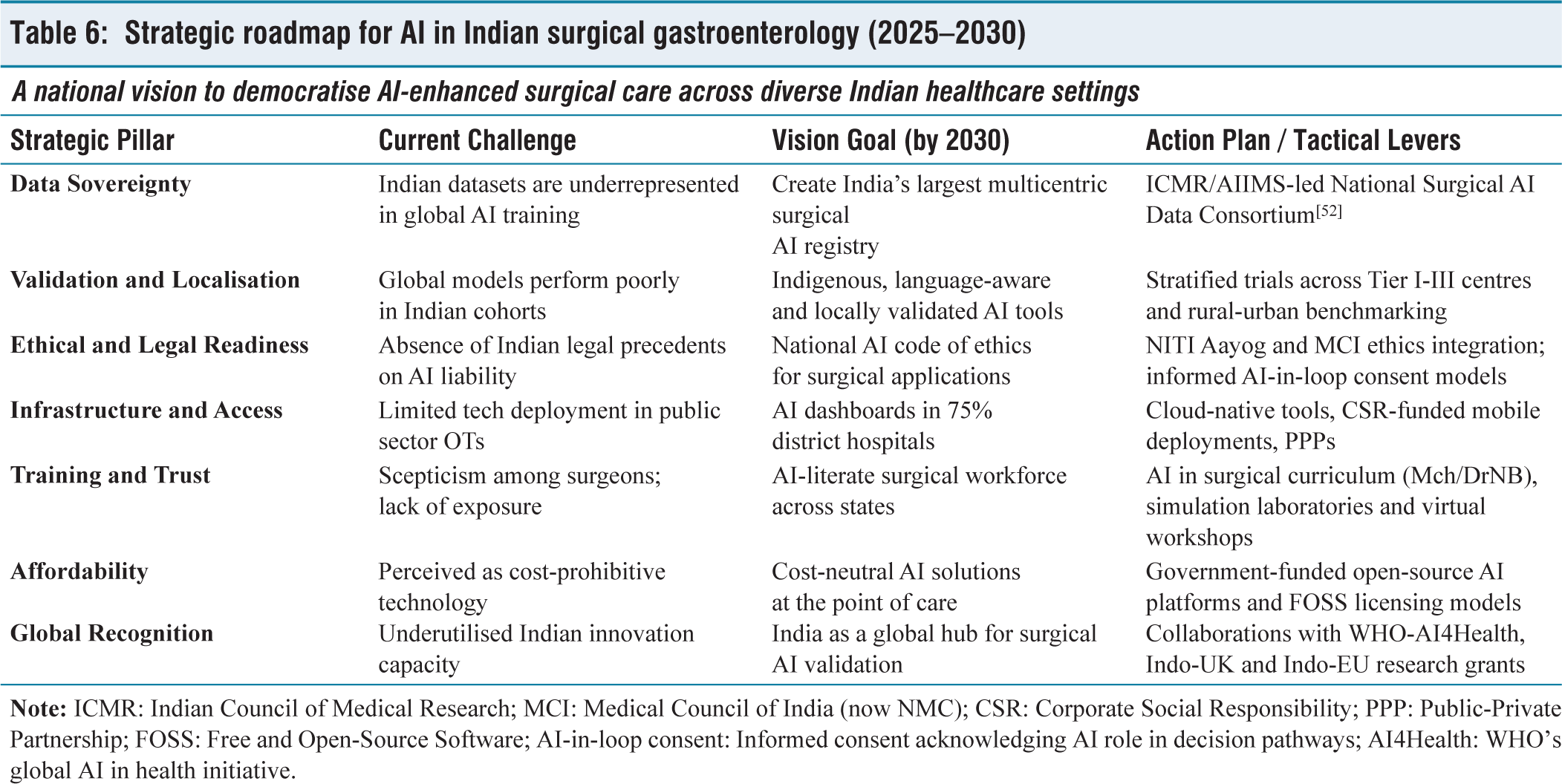
In India, AI holds transformative promise. High surgical volumes, limited specialist density and infrastructural constraints make the case for AI-assisted triage, navigation and surveillance particularly compelling. However, Indian data is underrepresented in global training cohorts, risking poor generalisability. Strategic priorities include building annotated datasets reflective of Indian practice, validating AI models across public and private institutions and ensuring affordability and accessibility.[52]
Several nascent initiatives in India underscore the growing national interest in AI-driven surgical innovation. The AIIMS-ICMR Surgical AI Consortium, launched in 2023, aims to create the country’s first multicentric annotated video repository for training computer vision models in laparoscopic and robotic procedures. Separately, the IISc-Bangalore and National Institute of Mental Health and Neurosciences (NIMHANS) collaboration has developed DL-based tools for real-time intraoperative phase recognition, currently being tested in hepatobiliary surgeries. In the private sector, Apollo Hospitals has piloted AI-based operative risk prediction tools integrated into its EHR system across multiple tertiary centres. Notably, the Department of Science and Technology under its ‘National Mission on Interdisciplinary Cyber-Physical Systems’ has prioritised surgical robotics and medical AI as focus verticals, offering funding to early-stage start-ups and academic incubators. These efforts collectively represent a foundational shift toward building India’s indigenous AI infrastructure for surgical gastroenterology.
A forward-looking roadmap outlining India-specific priorities and actionable strategies for scaling AI in surgical gastroenterology is provided in Table 6.
Strategic roadmap for AI in Indian surgical gastroenterology (2025–2030)
The future lies not in man versus machine but in synergy. Equipping Indian surgical teams with context-aware validated and interpretable AI tools can democratise excellence, reduce variability and improve surgical outcomes nationwide.
Limitations of this Review
As a narrative review, this manuscript is inherently limited by the potential for reviewer bias in literature selection and thematic emphasis. Unlike systematic reviews or meta-analyses, it does not follow a preferred reporting items for systematic reviews and meta-analyses (PRISMA)-guided protocol or employ formal risk-of-bias tools across studies. Instead, it prioritises clinical relevance, technological maturity and diversity of applications to provide a broad yet practical overview. While this approach enhances accessibility and scope, it may overlook certain granular comparisons or emerging models not yet widely cited. Readers are encouraged to interpret findings within this context.
Key Takeaways for Surgical Gastroenterologists
AI can forecast complications such as ALs, up to six days earlier than standard clinical detection using biochemical and ML integration platforms such as FluidAI Stream™.[30]
Real-time intraoperative guidance systems including Hepataug for liver resection and Indocyanine Green–Based Neural Network (ICG-NN) for perfusion quantification are increasingly accurate and clinically validated.[21,23]
XAI tools, such as SHAP and LIME, are essential for enhancing model transparency and clinician trust during surgical decision-making.[44]
India’s AI roadmap requires federated learning frameworks, open-source deployment models and integration of AI into surgical training curricula to achieve equitable national scalability.[43,52]
Surgeons should engage with AI tools not as rivals but as decision-enhancing allies, empowering workflow efficiency, precision and patient-specific personalisation.[40]
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
This manuscript is a narrative review based on previously published literature. No human participants, animals or patient data were involved. Therefore, ethical approval and informed consent were not required.
Credit author statement
Dr. Supreet Kumar (Guarantor): Conceived the review concept and title; supervised the entire manuscript development; performed advanced literature synthesis and structured critical appraisal across all six domains of AI integration; led drafting of the Introduction, Methods, Indian roadmap and Final Summary; coordinated manuscript structure, table development and SANRA guideline adherence; finalised references and ensured AI and plagiarism-safe narrative integrity.
Dr. Rigved Gupta: Led the drafting and refinement of Section 3 (Intraoperative AI and Computer Vision); contributed expert input on laparoscopic AR systems and real-time perfusion analytics; supervised ![]() design; provided critical feedback on technical performance metrics, validation frameworks and workflow feasibility; reviewed final version for surgical accuracy.
design; provided critical feedback on technical performance metrics, validation frameworks and workflow feasibility; reviewed final version for surgical accuracy.
Dr. Aishwarya Bhalerao: Conducted initial literature searches across PubMed and Scopus; compiled reference library (2015–2025); co-drafted Sections 1 and 2 with emphasis on predictive analytics and ML algorithms; designed Tables 1 and ![]() ; ensured chronological citation structure; supported figure/table integration and Vancouver-style referencing.
; ensured chronological citation structure; supported figure/table integration and Vancouver-style referencing.
Dr. Sonam Gupta: Co-authored Section 4 (Postoperative Monitoring and Surgomics); contributed a detailed review of early warning platforms and EHR-integrated algorithms; assisted in mapping SHAP/LIME XAI frameworks; revised Section 5 on interpretability and ethics; verified AI platform deployment examples.
Dr. Vivek Tandon: Reviewed all manuscript sections for clinical congruency and surgical applicability; provided expert input on real-world limitations, ethical implementation hurdles and medicolegal implications; oversaw final editing of Tables 4 and ![]() ; served as senior reviewer ensuring translational and academic accuracy.
; served as senior reviewer ensuring translational and academic accuracy.
Dr. Deepak Govil: Provided departmental oversight and mentorship throughout the manuscript process; contributed strategic insights on future AI deployment in Indian tertiary care; reviewed and approved ![]() (India-specific roadmap); critically appraised the manuscript from a policy and leadership standpoint; approved the final version for submission.
(India-specific roadmap); critically appraised the manuscript from a policy and leadership standpoint; approved the final version for submission.
All authors have made substantial contributions to the conception, drafting, critical revision and final approval of the manuscript. Detailed individual contributions are listed on the title page.
Data availability
No new datasets were generated or analysed for this narrative review. All data supporting the conclusions are derived from published literature, duly cited in the references.
Use of artificial intelligence
All intellectual decisions, critical appraisals and final drafting were conducted by the authors themselves. The content has been reviewed to ensure originality, human authorship and compliance with anti-plagiarism and AI detection standards.
Informed consent
Not applicable, as this article is a narrative review and does not involve patient data or direct participation.
Guarantor
Dr. Supreet Kumar (