
Abstract
Background and Aims:
Enteric fever is an acute febrile illness with fever caused by Salmonella species. The diagnosis is confirmed through culture testing. Absolute eosinopenia is a characteristic finding in enteric fever, and a high eosinophil count can effectively exclude this diagnosis.
Materials and Methods:
A retrospective observational study was conducted in our tertiary care hospital over 2 years involving 67 patients. Age, gender, complete blood count, liver function test, renal function test, and positive blood culture for Salmonella typhi/Paratyphi were collected from electronic health records. Statistics were presented with mean ± SD and frequency (percentage) for the continuous and categorical factors, respectively. All the statistical analysis was carried out using SPSS (IBM, 28.0).
Results:
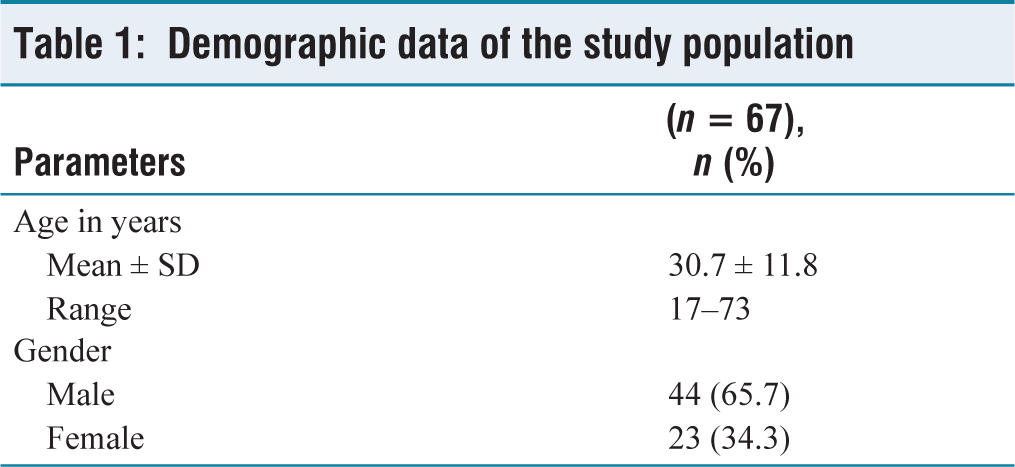
Of the 67 blood culture-positive patients, 53 had absolute eosinopenia. An average age of 30.7 ± 11.8 years, with ages ranging from 17 to 73 years. Other findings include elevated liver enzymes.
Conclusion:
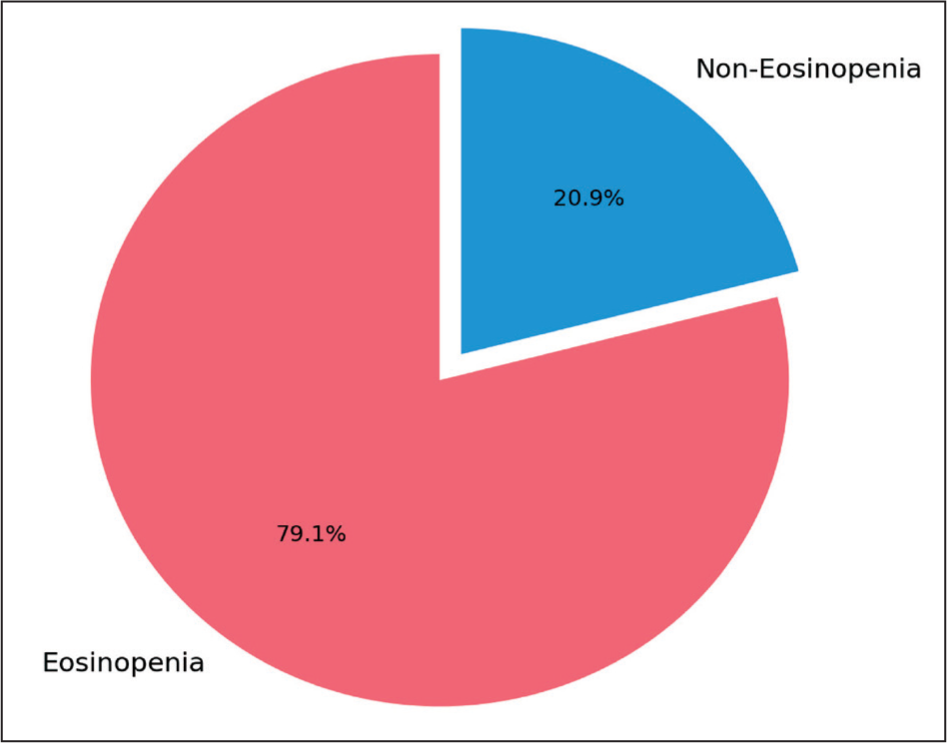
The strong correlation between enteric fever and absolute eosinopenia is demonstrated by this study, highlighting its potential as a quick and affordable diagnostic tool. Absolute eosinopenia was present in 79.1% of the study’s patients, which supports the usefulness of this metric in clinical practice, especially in environments with limited resources.
Introduction
Enteric fever, comprising typhoid and paratyphoid fever, is a severe systemic infection primarily transmitted through contaminated food and water.[1] It is caused by the bacteria Salmonella enterica subspecies enterica serovars Typhi and Paratyphi A, B or C, which are human-specific pathogens.[1] Enteric fever persists as a major public health challenge in numerous developing countries, particularly in Southeast Asia, including India.[2]
Symptoms of enteric fever vary from mild constitutional issues to severe complications affecting multiple organs. Common symptoms include fever, vomiting, diarrhoea, abdominal pain, cough, headache, and fatigue. The nonspecific nature of these symptoms, especially in endemic areas, makes clinical diagnosis challenging.[2]
The gold standard methods for diagnosing enteric fever include cultures of blood, urine, stool, or bone marrow to detect Salmonella, with blood culture being the most commonly employed.[1] However, these tests often produce delayed results due to the time needed for bacterial growth, which reduces their utility in early disease management.[1] As a result, there is a need for a reliable, affordable, and rapid marker for the early diagnosis of enteric fever.[2] A consistent feature of enteric fever is absolute eosinopenia, whereas a high eosinophil count can rule out the condition.[3] Eosinopenia in enteric fever results from multiple mechanisms.[1]
The lipopolysaccharide (LPS) endotoxin of Salmonella Typhi, through activation of TNF-alpha and associated inflammatory pathways, leads to suppression of bone marrow activity.[1] This results in the characteristic leukopenia and neutropenia seen in typhoid fever.[1] Since eosinophil production is especially vulnerable to such hematopoietic suppression, their numbers drop significantly.[1] Furthermore, systemic inflammation may cause eosinophils to be sequestered in tissues, and elevated cortisol levels during illness further inhibit their generation and survival.[1]
Recent studies have highlighted eosinopenia, characterised by an absolute eosinophil count of zero, as a frequent finding in enteric fevers.[2] Absolute eosinopenia is observed in approximately 70%–80% of cases.[4] While its presence can aid in diagnosing enteric fever, it does not distinguish it from other acute bacterial or viral infections.[4]
Materials and Methods
This study was conducted in our tertiary care hospital over 2 years. It was a hospital-based retrospective observational study. The objective of the study is to find the prevalence of eosinopenia in blood culture-proven enteric fever patients. This study includes adults (aged above 18 years) diagnosed with enteric fever by positive blood culture for Salmonella typhi/Paratyphi. Epidemiological, demographic, clinical, baseline blood work and outcome data will be extracted from electronic health records using a standard data collection form. Data to be collected includes age at diagnosis, gender, complete blood count, Liver function test, Renal function test, and positive blood culture for Salmonella typhi/Paratyphi. Informed consent was waived due to the retrospective nature of the study. However, patient data was anonymised and treated with strict confidentiality.
Statistical Analysis
Summary statistics were presented with mean ± SD and frequency (percentage) for the continuous and categorical factors, respectively. The median (IQR) was presented while the data was skewed. Chi-Square/Fisher’s exact test was used to determine the association between two independent categorical factors. P < .05 is considered statistical significance. All the statistical analysis was carried out using SPSS (IBM, 28.0).
Results
The study involved 67 participants, with ages ranging from 17 to 73 years and an average age of 30.7 ± 11.8 years. The gender distribution was predominantly male (65.7%), with females accounting for 34.3% [Figure 1], as shown in Table 1
Bar chart showing the percentage of male and female patients in the enteric fever group
Demographic data of the study population
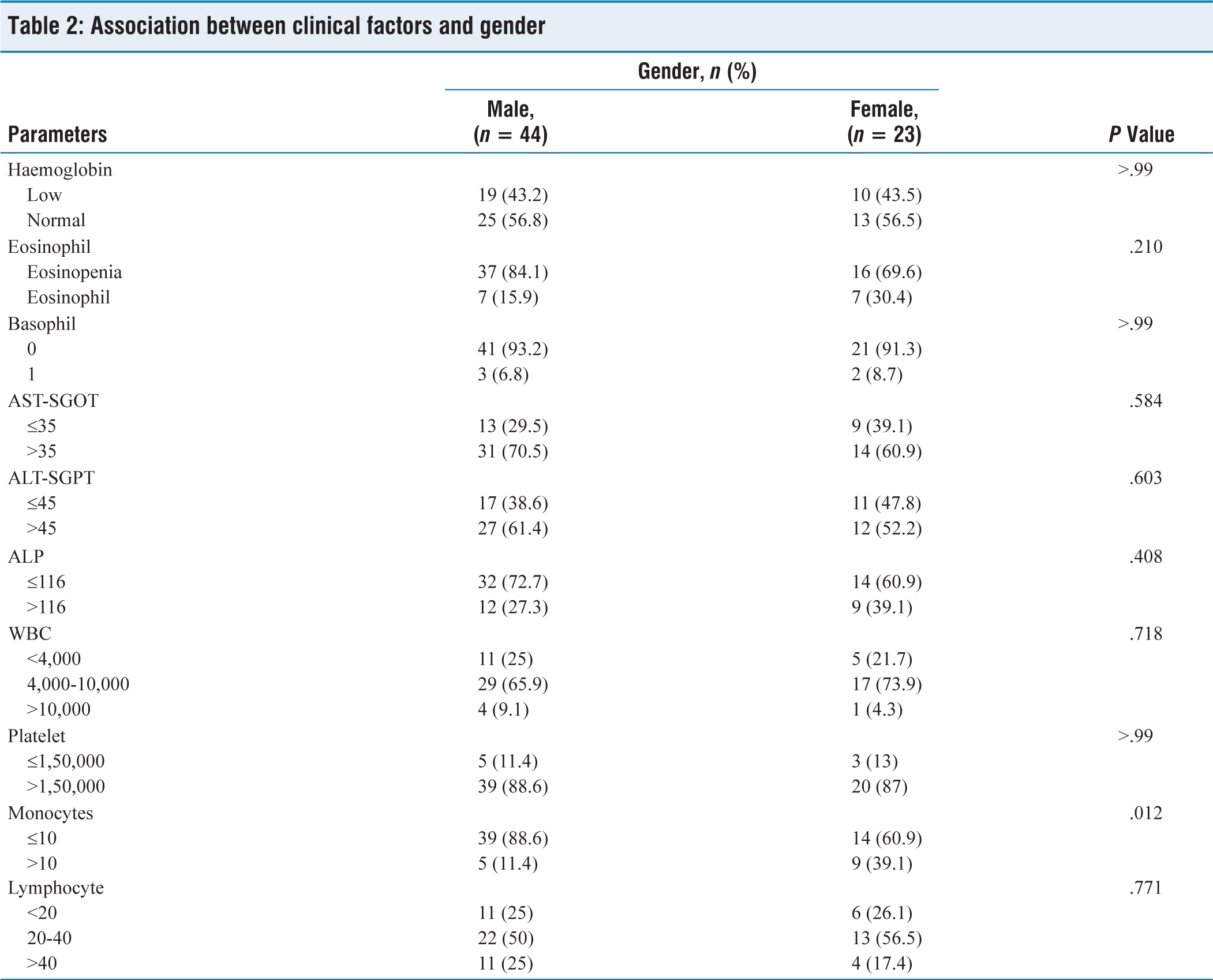
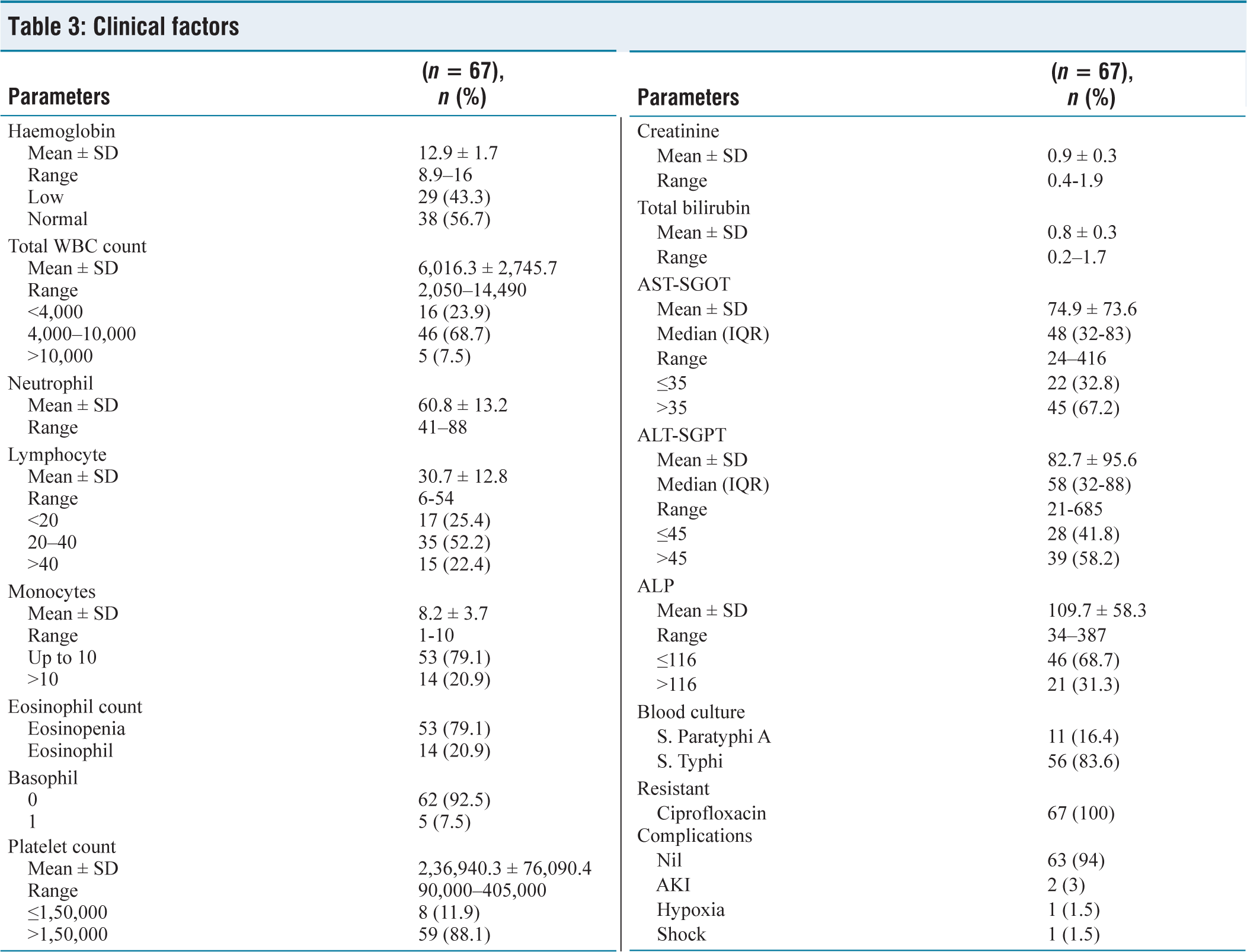
Leucopenia was observed in 23.9% (n = 16). Monocytosis was observed in 20.9% (n = 14). Absolute eosinopenia was observed in 79.1% (n = 53) [Figure 2]. Thrombocytopenia was observed in 11.9% (n = 8), as shown in Table 2.
Distribution of eosinopenia in enteric fever
Association between clinical factors and gender
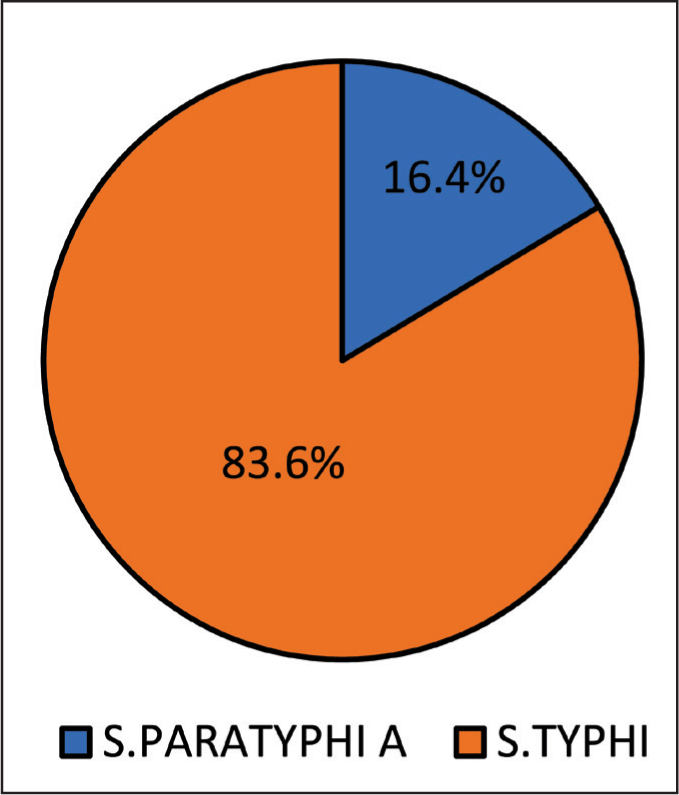
Liver Enzymes: AST and ALT were elevated in the majority, with AST >35 in 67.2% and ALT > 45 in 58.2%. S. Typhi was the predominant strain (83.6%), while S. Paratyphi A was identified in 16.4% [Figure 3]. All isolates showed resistance to ciprofloxacin. 94% of participants had no complications, while 3% experienced acute kidney injury (AKI), 1.5% hypoxia, and 1.5% shock, as shown in Table 3.
Pie chart showing positivity for Salmonella typhi and Salmonella paratyphi in blood cultures
Clinical factors
Discussion
A total of 67 patients with blood culture-proven enteric fever were admitted to the hospital from January 2023 to December 2024. The main objective of this study is to find the prevalence of eosinopenia in enteric fever patients.
Absolute eosinopenia, that is, an absolute eosinophil count of 0 cells/mm3 or an eosinophil percentage of 0, was seen in 53 (79.1%) of the total patients. Our study findings indicate that absolute eosinopenia may be an effective diagnostic marker for enteric fever. Our findings parallel those of a previous study by Gandhi A. and Darshan A., who reported absolute eosinopenia in 93.3% of enteric fever patients.[1] Similarly, Vijayalakshmi Mallaya B found absolute eosinopenia in 93.9% of their enteric fever patients.[2]
Comparison with Serological Tests
Recent studies, including Panigrahi et al. (Cureus, 2025), have demonstrated that absolute eosinopenia (AEC = 0 cells/μL) has a high specificity (91.3%) and a positive predictive value of 83.7%, which is comparable or superior to TyphiDot IgM (specificity 93.8%, PPV 84.8%). Although eosinopenia shows slightly lower sensitivity than TyphiDot (45.6% vs. 35.4%), its early appearance in the febrile phase and rapid availability make it a valuable adjunct in early diagnosis. However, eosinopenia should not be considered a replacement for serological tests but rather an adjunct marker—especially useful where serological kits are unavailable or in early stages before seroconversion occurs.[5]
As our study was retrospective, the precise timing of the eosinophil drop in relation to symptom onset was not available.
Conclusion
This study demonstrates a strong correlation between absolute eosinopenia and enteric fever. In clinical practice, eosinopenia can serve as a cost-effective and rapid screening tool for diagnosing infections, especially in resource-limited settings.
Footnotes
Acknowledgements
The authors acknowledge Dr Venkatachalam, Director of Medical Services; Dr Muralidharan M, Director of Medical Education; and Mr Lokesh, Biostatistician, Ms Shivashankari Apollo Hospitals, Chennai, Tamil Nadu, for their constant support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The institutional ethical committee approved the protocol (AMH-C-S-024/03-25, MARCH 2025). The Institutional Ethics Committees approved the study protocol. Informed consent was waived off due to the retrospective nature of the study.
Informed consent
As this is a retrospective study using existing data, informed consent from individual patients will not be obtained. However, patient data will be anonymised and treated with strict confidentiality.
Credit author statement
SS participated in literature review, data acquisition, data analysis, interpretation, manuscript writing.
SA participated in conceptualization, methodology, supervision, validation, manuscript editing.
All authors read and approved the final manuscript.
Data availability
The data supporting the findings of this article is not publicly available. Questions about the data can be directed to the corresponding author.
Use of artificial intelligence
No AI assisted tools were used in the writing or editing of this manuscript.