
Abstract
Introduction:
Different surgical procedures in otorhinolaryngology are done to address the narrowing of upper aerodigestive path in case of stenosis or stricture. The postoperative complications, such as scarring or stenosis, can occur in the upper airway and oesophagus. The alkylating antineoplastic antibiotic mitomycin-C (MMC), which is an aminoglycoside is an additional treatment option to prevent scarring or stenosis.
Methods:
A comprehensive review of literature from databases such as Scopus, PubMed, Medline, and Google Scholar was conducted to analyse the role of MMC in otorhinolaryngological surgical procedures.
Results:
The stricture or stenosis of the upper aerodigestive tract can result in significant morbidity and often pose challenge in life. Endoscopic airway dilation for treating laryngotracheal stenosis can provide short-term improvement, but it is often associated with long-term recurrence. Recently, the use of MMC has been investigated as an additional treatment to help reduce scar tissue formation.
Conclusion:
MMC regulates wound healing and inhibits scarring or stenosis formation by preventing fibroblast proliferation and the production of extracellular matrix proteins. MMC application has been shown to be safe in animal and human studies. It has been proposed that applying MMC during endoscopic dilatation and laser surgery can improve the results, however, this has not been thoroughly investigated.
Introduction
Synechia is the most common complication following otorhinolaryngology surgical procedures.[1] There are several materials used to reduce the incidence of synechia, including Mitomycin C (MMC).[2] Many surgical procedures in otorhinolaryngology address stricture of the aerodigestive path. Furthermore, the postoperative complications can occur due to scarring or restenosis.[1] The morbidity from severe aerodigestive tract stenosis might be severe and frequently difficult for otorhinolaryngologists to treat. MMC has been investigated as a further therapeutic approach in recent years to lessen the development of scar tissues.[2] Streptomyces caespitosus is the source of the anti-tumour antibiotic MMC. MMC’s anti-tumour action stems from its ability to impede DNA replication, which leads to cell death.[3] MMC shows inhibition of fibroblastic proliferation in vivo and vitro. Topical application of MMC is useful as an adjunct in reducing cicatricial scarring of the airways. MMC is being utilised as an adjuvant in a variety of surgical procedures in the field of otorhinolaryngology, including myringotomy, functional endoscopic sinus surgery, laryngotracheal reconstructive management, and surgery for choanal atresia.[4] The purpose of the review is to discuss the role of MMC in different otorhinolaryngological procedures and its impact on the output.
Methods of Literature Search
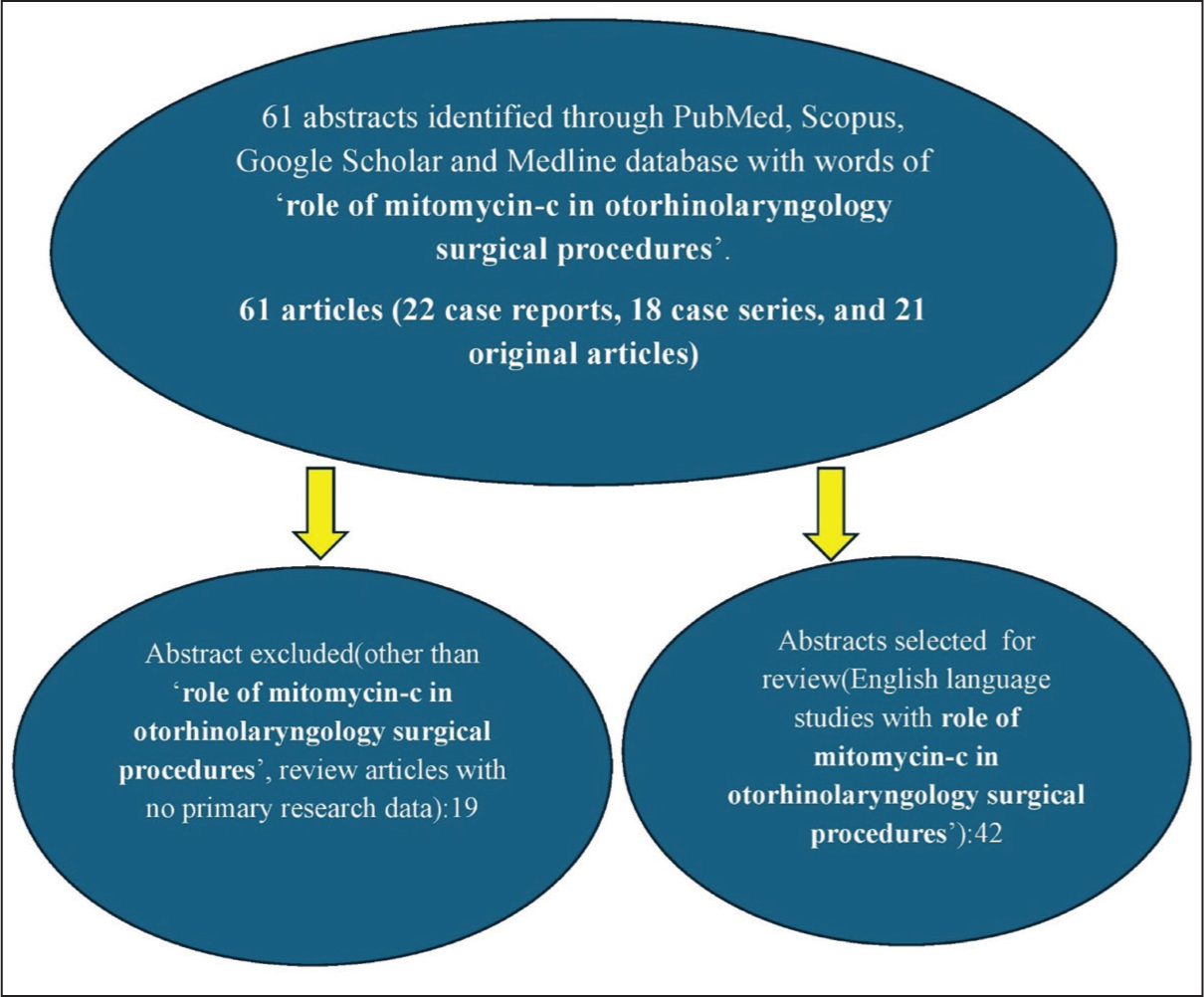
We conducted a search for research articles on the role of MMC in otorhinolaryngological procedures using various methods. The process began with searching online databases such as Scopus, PubMed, Medline, and Google Scholar. A search strategy was created based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. The search approach found published article abstracts, and citations were used to manually find more research publications. The suitability of observational studies, comparative studies, case series, case reports, and randomised controlled trials for inclusion in this review was evaluated. A total of 61 articles (22 case reports, 18 case series, and 21 original articles) were found across various databases, with 42 being included in this review [Figure 1]. This article examines the aspects of role of MMC in otorhinolaryngology procedures. This review article discusses the history of MMC and its role in laryngotracheal stenosis, choanal atresia, endoscopic dacryocystorhinostomy (DCR), myringotomy, esophageal atresia, endoscopic sinus surgery, and the toxicity of MMC.
Methods of literature search
History
In 1955, researchers in Japan discovered mitomycin from samples of bacterium Streptomyces caespitosus.[5] According to one study, a brief exposure to MMC causes corneal epithelial cells to generate proteins and other substances that accelerate the clearance of debris in a paracrine manner and enlist resident epithelial and immune cells as well as stromal fibroblasts to support regenerative and cause no fibrotic wound healing.[6] In 1963, MMC was first used topically as an adjuvant treatment for pterygium which reduce relapse rates from 89% to 2.3%.[7] The antifibrotic action of MMC has been observed by various authors. MMC is helpful to reduce the scarring and fibrosis formation in laryngotracheal stenosis and other otolaryngological procedures to prevent scarring and stenosis because this medication has been used successfully with no adverse effect for more than 40 years in pterygium and glaucoma procedures. MMC has an excellent success rate when utilised in glaucoma filtration surgery to maintain trabecular patency. It results in a decrease in fibroblasts’ capacity to multiply. Both in vitro and in vivo, it has been observed that MMC mostly inhibits fibroblastic proliferation while permitting epithelial development.[8]
Mitomycin-C
MMC is an aminoglycoside antibiotic that has alkylating anticancer effects. It prevents fibroblast and epithelial cells from proliferating and acts against all cells, regardless of the stage of the cell cycle. It affects the healing process by specifically preventing mitosis and protein synthesis by stopping DNA replication. MMC is an alkylating antineoplastic antibiotic that is an aminoglycoside. It is produced by the fungus Streptomyces caespitosus. It works against all cells, independent of the stage of the cell cycle, and prevents the fibroblast and epithelial cells from replicating. It affects the healing process by specifically stopping DNA replication and preventing mitosis and protein synthesis. MMC is an alkylating antineoplastic antibiotic that is an aminoglycoside. The fungus Streptomyces caespitosus produces it. It works against all cells, independent of the stage of the cell cycle, and prevents the fibroblast and epithelial cells from replicating. The antineoplastic drug MMC has been seen to reduce the incidence of scar tissue. It has been shown to reduce the proliferation of the fibroblast and its activity, which can decrease the formation of scar.[9] It affects the healing process by specifically blocking DNA replication and inhibiting protein synthesis and mitosis. MMC mostly treats carcinoma of lung (non-small cell) and resistant malignancies of the stomach, colon, cervix, rectum, and bladder by interfering with the M phase of cell division. However, MMC specifically prevents fibroblasts from proliferating in tissue culture. Otorhinolaryngological experience with MMC encompasses cases of subglottic stenosis, laryngeal web, choanal atresia, laryngotracheal stenosis, bronchial lumen stenosis, oesophageal luminal stenosis, stenosis of hypopharynx and DCR.[10] According to one study, MMC may delay the recurrence of symptomatic stenosis in most patients, but it does not prevent it.[11] The anti-proliferative properties of MMC are at 0.04 mg/ml and in higher dosages, provide cytocidal effects.[12]
Doses of MMC
The mucosa’s raw surface is covered with pledget soaked in diluted MMC (0.5 mg/ml), and the forceps is used to provide direct pressure. Pressure is applied for two minutes, until the mucosa blanches.[13] This procedure can be repeated circumferentially along the luminal airway until all the mucosa is treated. Haemostasis should be secured before the application of MMC.
Laryngotracheal Stenosis
Diseases at the airway, such as laryngotracheal tract requires multiple surgical procedures to control the formation of inflammatory tissues like cicatrical scar, with granulation tissue being an important post-operative complication.[14] Despite advancement in the treatment of laryngotracheal stenosis, formation of cicatrix and stenosis recurrence is the primary reason of failure.[15] The most common cause of laryngotracheal stenosis is damage to the mucosal and/or cartilaginous tissues of the laryngotracheal tract. This frequently results in cicatrix development, ulceration, and stenosis. Numerous endoscopic procedures, such as cryosurgery, dilation, and micro-cauterisation, have been reported.[16]
To keep a patent airway, several endoscopic surgical procedures may be required. Laryngotracheal stenosis is treated mostly with endoscopic CO2 laser therapy with rigid dilatation.[17] Resection of the stenotic segment and end-to-end anastomosis are the two surgical procedures that effectively treat laryngotracheal stenosis. However, not all patients with laryngotracheal stenosis are amenable to undertake this surgical procedure, so effective endoscopic treatment is done for laryngotracheal stenosis. Although the stenotic region is dilated during endoscopic treatment, restenosis may result from wound healing. MMC is given locally to slow down or even stop the proliferation of fibroblasts. MMC possesses both antineoplastic and antiproliferative properties. Its clinical use as a regulator of the wound healing response stems from its ability to decrease fibroblast growth both in vitro and in vivo.[18]
Choanal Atresia
A rare deformity called choanal atresia causes upper airway blockage in newborns and infants.[19] Females are more likely than males to have it, and it is more frequently unilateral and right-sided than bilateral.[20] The transnasal endoscopic approach is an ideal technique for getting good surgical filed and allows bone resection with minimal injury to the surrounding mucosa and vital structures.[21] After surgery, there is a high chance of restenosis, ranging from 9% to 36%.[22] The use of postoperative stenting for variable periods may help prevent restenosis. Soft surgical stenting material is found to have higher surgical success than non-flexible material.[23] MMC enhances the surgical outcome of choanal atresia and greatly lowers the rate of restenosis without causing any problems.[24] MMC (1 mg/ml) is often applied at the nasopharyngeal orifice for 3–5 minutes to prevent restenosis and no stents are required. Children with Coloboma of the eye, Heart defects, Atresia of the nasal choanae, Retardation of growth, Genital abnormalities, and Ear abnormalities (CHARGE) syndrome and bilateral or bony atresia are believed to have a higher risk of restenosis. MMC is an antiproliferative substance that stops growth to prevent stenosis from recurring. This may cause inhibition to from scar tissue and reduce the rate of restenosis. The neochoana is tailored by the pathology encountered. Balloon dilation, Hegar dilators, and micro-debridement are used to remove the atretic bony plate.
Endoscopic Dacryocystorhinostomy
For individuals with epiphora caused by primary acquired occlusion of the nasolacrimal duct, DCR is the preferred surgical approach. Treatment for secondary to nasolacrimal duct occlusion is provided by DCR. DCR can be carried out endonasally or externally. With a 95% success rate in primary instances, endoscopic DCR is a well-established treatment for chronic dacryocystitis.[25] During the postoperative healing process of endo DCR, scarring can further reduce the ostium size.[26] Topical application of MMC at the site of ostium inhibits circumosteal fibrous tissue growth and scarring. One study showed that application of MMC to the osteotomy location is safe and effective in increasing the success rate of surgery in primary external DCR and revision endo-DCR, but it does not offer any significant benefit in case of primary endo-DCR.[27] Another study found that while there was one instance of turbine-septal synechia development in the non-MMC group, there were no problems in the MMC group. The MMC group’s success rate was 99.2%, compared to the control group’s 89.6%, and the difference was statistically significant.[28]
Myringotomy
When treating otitis media with effusion, a ventilation tube can be useful.[29] Other indications for middle ear ventilation tubes include gentamycin therapy in Meniere’s disease, hyperbaric oxygen therapy, retraction pockets, acute otitis media with complications, chronic hypoventilation of the middle ear cleft, retraction pockets, topical corticosteroids, and acute otitis media with complications or facial nerve palsy.[30,31] The closure of human tympanostomy ventilation opening is delayed by use of MMC and radiofrequency. The presence of an inflamed tympanic membrane appears to increase the effectiveness of MMC. When combined with adenoidectomy, the radiofrequency aided MMC improved tympanostomy is a safe, accurate, and economical surgery that offers a feasible therapeutic option for recurrent otitis media and secretory otitis media.[32]
Nasal and Sinus Surgery
Refractory chronic rhinosinusitis is best treated with functional endoscopic sinus surgery. The cause for failure of the functional endoscopic sinus surgery is synechia formation which again results in recurrence of the disease.[33] Preserving the sinonasal mucosa during surgery, taking good care of the surgical wounds, and seeking outpatient care as soon as adhesion is noticed are the best ways to stop synechia formation.[33] In spite of these measures, some surgeons cause injury to the sinonasal mucosa and improper postoperative care leads to synechia development. Up to 36% of cases of synechia, the most frequent complication after sinonasal surgery, have been reported.[34] Various materials, including Merocele, Floseal, Sepragel, and hyaluronic acid, have been tested to lessen the difficulties. MMC is also an important material used to prevent postoperative fibrosis. MMC’s antiproliferative action on human fibroblasts can control scarring and stop the development of excessive fibrosis. A single five minutes topical treatment of MMC has antiproliferative effects lasting up to 36 hours.[35] When MMC is quickly administered to human mucosa, it enhances fibroblast death and decreases fibroblast multiplication.[36] For individuals having functional endoscopic sinus surgery, MMC effectively prevents postoperative synechia.[37]
Compared to a 2% recurrence in the absence of MMC application, recurrence is avoided when MMC is applied in the maxillary sinus at the location of the antrochoanal polyp’s origin after endoscopic excision.[38] Although the precise etiopathogenesis of antrochoanal polyps is still unclear, MMC’s ability to prevent their recurrence may be due to its ability to block DNA synthesis, which inhibits cell migration and mitosis and lowers the rate of cell proliferation, especially at the polyp’s origin site.[38,39]
Esophageal Stenosis
Oesophageal stenosis commonly occurs as a result of stenosis brought on by radiation or caustic damage, or stricture at an anastomosis point. The physical or chemical trauma at the mucosal lining of the oesophagus causes fibrosis and stenosis during the healing process.[40] The stenosis of the lumen of oesophagus manifests obstruction to the food bolus and causes dysphagia. MMC is helpful to reduce the number of dilations needed for strictures of the oesophagus, regardless of cause. A study showed that repeated use of MMC causes softening of the stricture, facilitating the easier passage of dilators earlier in the process.[35] In this study, the authors administered the MMC for two minutes at the lowest dose (0.1 mg/ml).
Toxicity of MMC
MMC has various topical usages in otolaryngologists, including laryngotracheal surgery, endoscopic sinus surgery, and choanal atresia to minimise or even prevent post-operative synechia and stenosis. Although no evidence of MMC toxicity has been reported in otorhinolaryngology and ophthalmologic literature have shown serious, vision impairment complications due to topical application of MMC. The complications of MMC are thought to be caused by local toxicity due to buildup of fibrinous material at the surgical site, which necessitates immediate airway intervention due to partial airway blockage.[41] MMC is simple to use without posing any additional risks to patients. There have been no instances of bleeding, infection, crusts, or granulations forming while using it. By applying MMC topically, the recurrence rate is reduced without endangering the patient or requiring additional tools or specialised training. Thus, the MMC can be used safely and successfully.[42]
Conclusion
The cicatrix formation and recurrence of stenosis are important morbidities even after performing advanced treatment for the upper aerodigestive area. Sometimes patients require multiple endoscopic surgical procedures to achieve a successful outcome in the airway and upper digestive tract. MMC has been applied as an adjunctive therapy in different otorhinolaryngological procedures, such as airway, oesophageal, sinonasal, and ontological procedures. Its topical application minimises scar tissue formation postoperatively. MMC appears to be both economical and safe for endoscopic airway surgery.
Footnotes
Acknowledgements
The acknowledgements for this review are extended to those who have previously contributed to and conducted research on the same topic. This recognition acknowledges the existing body of work and the collective efforts of researchers in the field. The author expresses gratitude to those who contributed to the development and execution of this research, acknowledging their invaluable support and collaboration. AI plagiarism detection tools were employed to ensure the authenticity of the acknowledgements and avoid any instances of plagiarism.
Consent for publication
The article adheres to ethical principles rooted in the Declaration of Helsinki.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Given that this is a literature-based study, it is important to note that strict adherence to ethical principles and guidelines was not required. The research primarily involved the examination of existing literature and did not directly involve human subjects.
Informed consent
Not applicable.
Credit author statement
Santosh Kumar Swain contributed to concept, literature search, data acquisition, manuscript preparation, manuscript editing and approval of the final version to be published.
Use of artificial intelligence
Not applicable.
Data availability
Santosh Kumar Swain, the author, maintains a commitment to transparency in presenting data in this literature-based study. All information and findings shared in this work are authentic and accurately represent the research conducted. Any potential conflicts of interest have been meticulously disclosed to ensure transparency.