
Abstract
Background and Aims:
Hydatid cysts in the liver generally remain asymptomatic for years. However, they may rarely enlarge and spontaneously rupture, leading to anaphylaxis and the dissemination of the cyst into the abdominal, pleural, or biliary tract.
Methods:
Our patient was a middle-aged male who presented with a dual complication of an intrahepatic hydatid cyst rupturing into the inferior vena cava causing pulmonary embolism, and simultaneously rupturing into the pleural cavity, causing hydropneumothorax.
Results:
The patient was managed with antiprotozoals, anticoagulants and intercostal drain insertion for hydropneumothorax.
Conclusion:
Cyst rupture is a critical complication of a hydatid cyst. However, this unique presentation of a hepatic hydatid cyst needs awareness and attention from the medical fraternity for its early identification and optimal management.
Introduction
A hydatid cyst is a helminthic infection resulting from the metacestode stage of the dog tapeworm, Echinococcus granulosus.[1] Liver hydatids can remain symptom-free for 10 to 15 years. The natural history may be affected by complications such as rupture, anaphylactic shock, and some uncommon but serious complications like pulmonary embolism.[2] There are three types of hydatid cyst rupture: contained rupture (within the liver parenchyma, occurring in 1%–5% of cases), direct rupture into the peritoneal or pleural cavity (observed in 1%–16% of cases), and communicating rupture (where the cyst connects with bile or vascular ducts or the bronchial tree).[3] The cardiovascular complications related to hydatid cysts range from 0.02% to 2%.[4] We present a unique case where the hydatid cyst burst directly into the pleural cavity and the inferior vena cava (IVC).
Case Presentation
A middle-aged male presented with a new onset of productive cough and shortness of breath for 10 days. There was no history of fever, chest pain, palpitations, pedal oedema, decreased urine output, jaundice, weight loss or haemoptysis. On examination, the patient had tachycardia with a pulse rate of 135/min, with tachypnoea and SpO2 of 82% under room air. On examination, there was decreased air entry in the left-sided mammary and inframammary region, with mild tenderness in the right hypochondriac region. The rest of the systemic examination was unremarkable.
Chest radiography showed left-sided hydropneumothorax for which an intercoastal drain was inserted immediately. Laboratory reports revealed microcytic hypochromic anemia (Hemoglobin-9.5 g/dl) with neutrophilic leucocytosis (TLC-18,000/µL). Total eosinophil count was 920 cells/µL. Alkaline phosphatase (610 U/L) was raised with normal bilirubin levels. Pleural fluid analysis showed an exudative pleural effusion that was neutrophil predominant. Culture of pleural fluid showed no microbial growth. Sputum culture also showed normal microbial flora. Pleural fluid and sputum cartridge based nucleic acid amplification test turned out negative. His purified protein derivative skin test and fundus examination for choroid tubercles were negative. Viral serologies for human immunodeficiency virus and hepatitis were negative. Meanwhile, the patient was managed with broad-spectrum antibiotics and oxygen support.
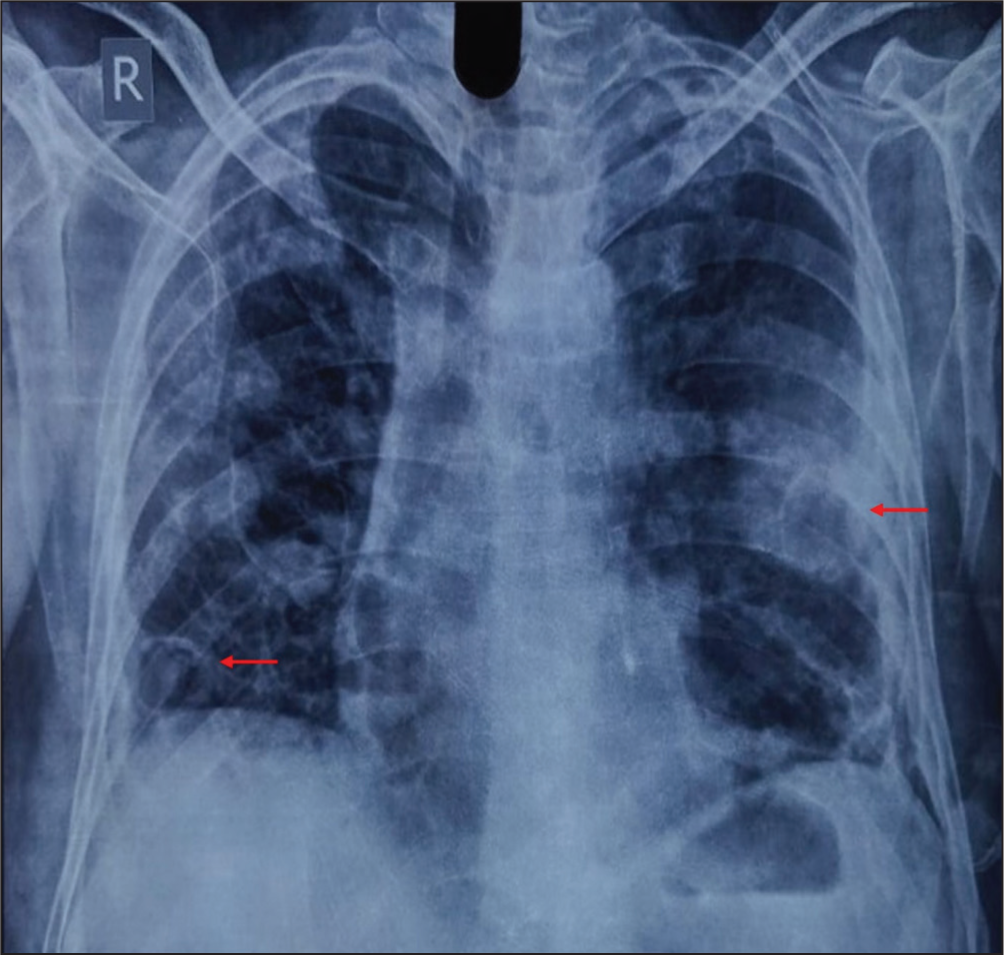
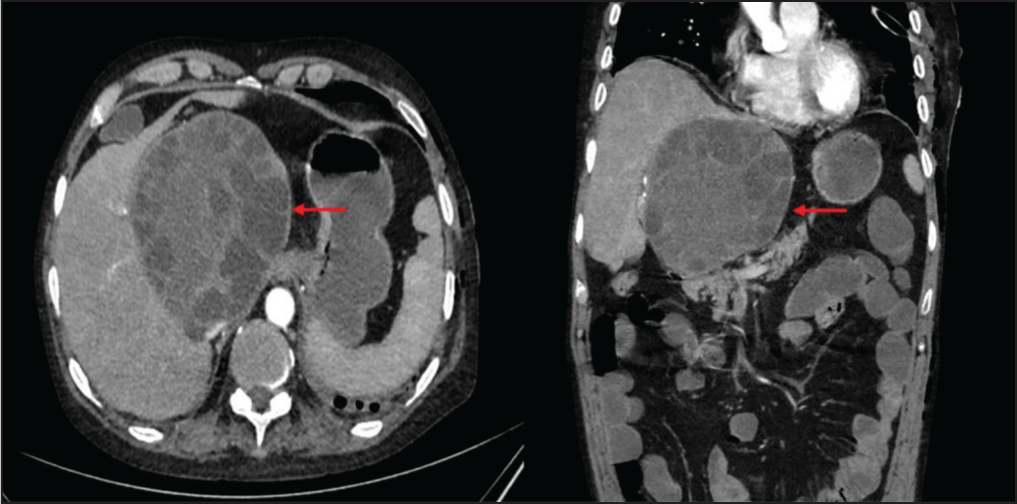
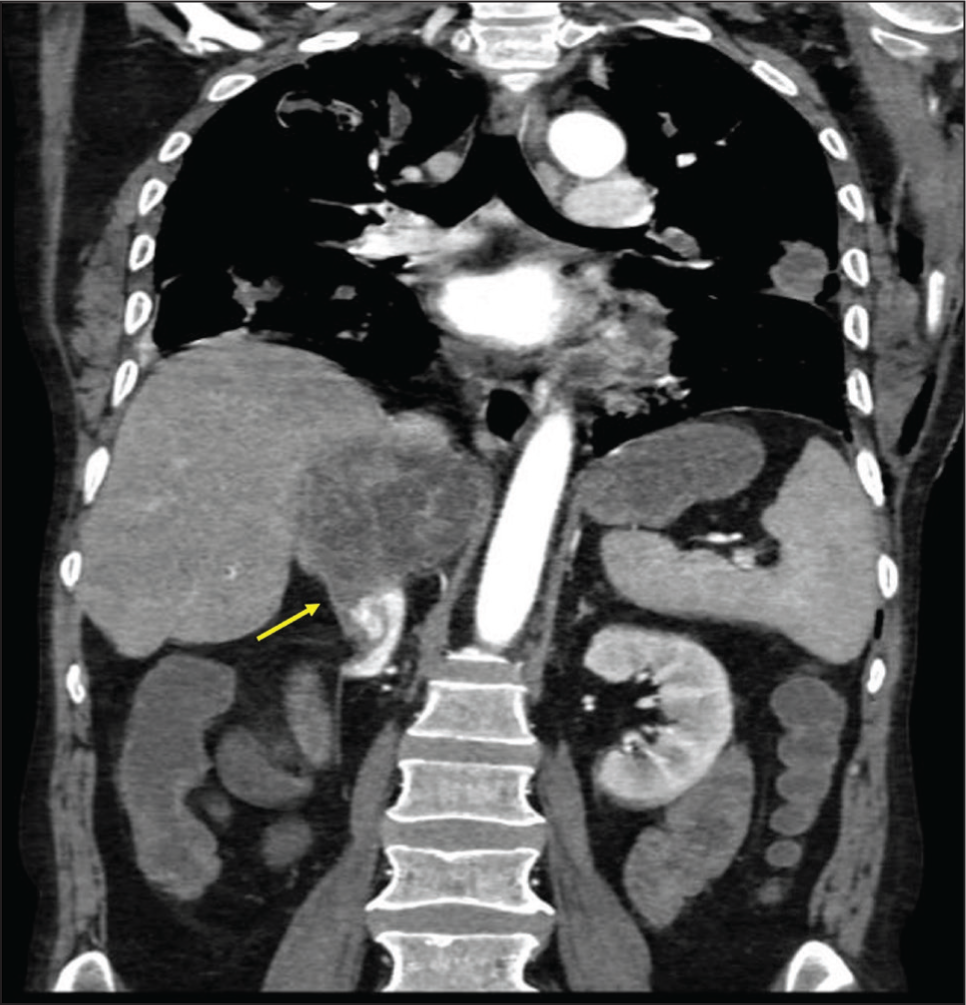
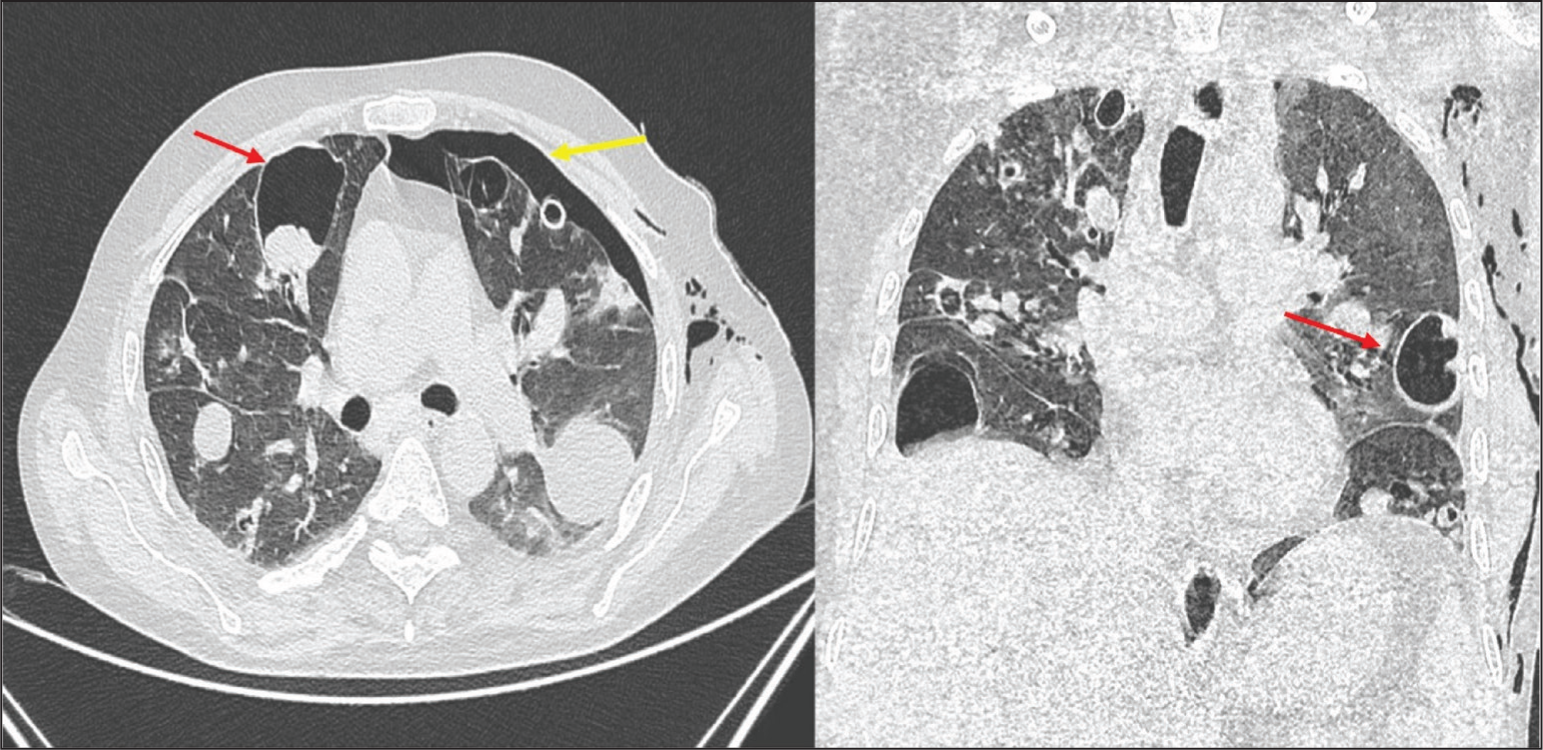
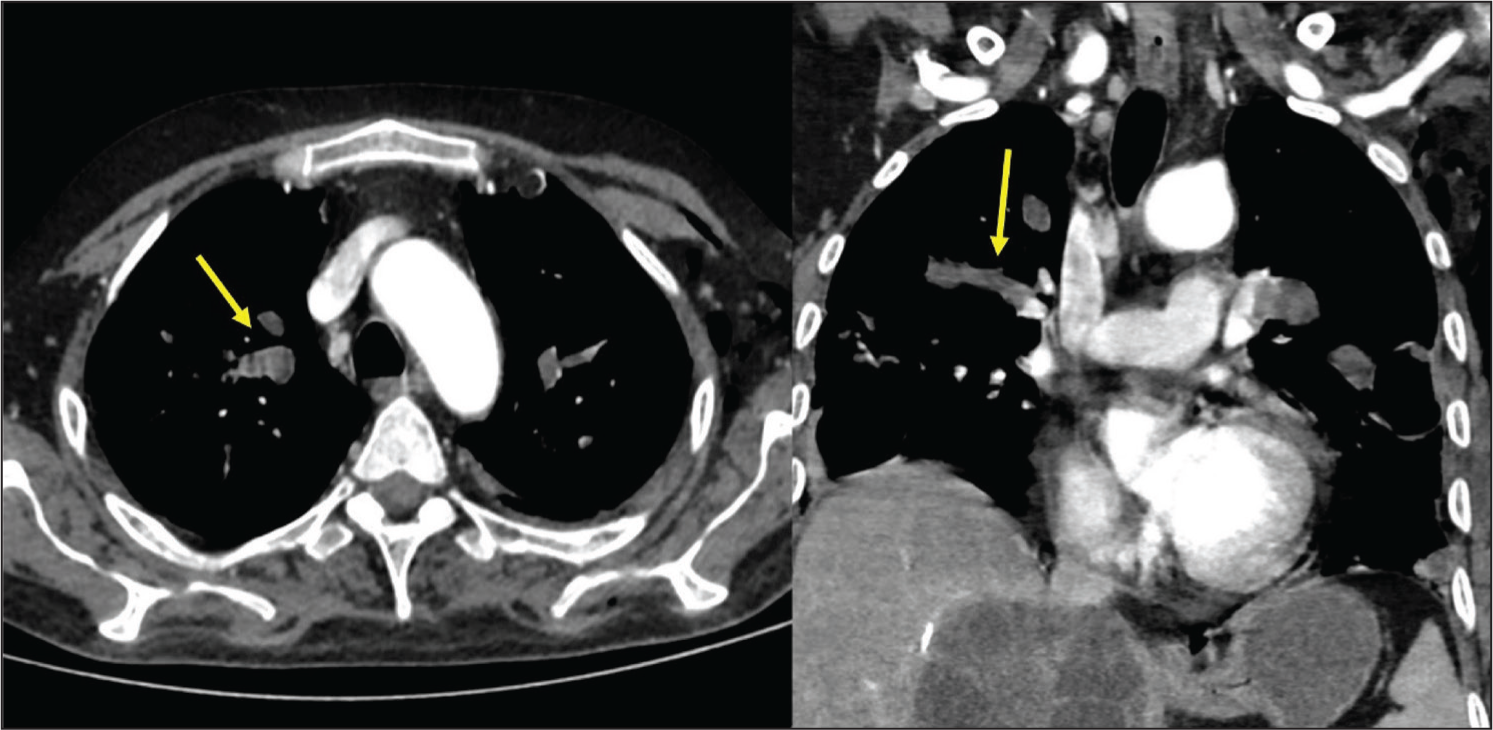
After the thoracostomy, a repeat chest radiography showed multiple cavities in the lung [Figure 1]. Ultrasonography of the abdomen showed a heterogenous hypoechoic lesion measuring 9 cm × 8 cm in the right lobe of the liver. The possibility of either a ruptured hydatid cyst or an amoebic liver abscess was kept. Amoebic serology IgG for Entamoeba Histolytica came out to be negative whereas Echinococcus IgG antibody levels measured using an enzyme-linked immunosorbent assay test were elevated. Later, contrast enhanced computed tomography (CT) of chest and abdomen and CT pulmonary angiography showed hepatic hydatid cyst measuring 11 cm × 10 cm [Figure 2] with one of the daughter cysts bulging through the posterior wall of the cyst into intrahepatic IVC seen as filing defect indicating rupture [Figure 3] and multiple cystic lesions in lungs [Figure 4]. Also, there was an intraluminal filling defect in the segmental and subsegmental branches of bilateral pulmonary arteries on indicative of pulmonary embolism due to disseminated hydatid cysts [Figure 5]. Venous doppler of bilateral lower limbs ruled out deep vein thrombosis. Hypercoagulable workup including protein C, protein S, antithrombin III and homocysteine levels turned out normal. Transesophageal echocardiography did not reveal any intracardiac hydatid cysts.
Chest radiograph PA view showing multiple cavities (red arrows) in the lung
Axial and coronal soft tissue computed tomography scan shows a well-defined round partially exophytic hypodense cyst (red arrows) in IV a and VIII segment of liver showing multiple variable-sized thin-walled daughter cysts within. No evidence of any solid components seen
Coronal section of CT angiography showing one of the daughter cysts is seen bulging through the posterior wall of the cyst into intra-hepatic IVC (yellow arrow) with its resultant attenuation in the caliber
Axial and coronal lung window of computed tomography shows multiple variable sized cystic lesions (red arrows) in the bilateral lung parenchyma showing air fluid level within them and left moderate hydropneumothorax (yellow arrow)
Axial and coronal CTPA images shows sub-segmental branches of bilateral pulmonary artery show dilatation and intra-luminal filling defect (yellow arrows) suggestive of pulmonary thromboembolism
After confirmation of diagnosis of ruptured hydatid cyst with pulmonary embolism, a cardio-thoracic opinion was sought and surgery was planned but the patient refused the procedure. Considering his wishes, he was started on medical treatment with albendazole 400mg twice daily and rivaroxaban 15 mg twice a day. The intercostal drain was removed once the pneumothorax had resolved. During follow-up at three weeks, his compliance with anti-protozoal therapy was ensured. At this time, he was advised to continue rivaroxaban at 20 mg once a day for a total of three months. However, in the next week, he developed another episode of acute breathlessness requiring emergency rehospitalisation and was diagnosed with recurrent massive pulmonary thromboembolism. Despite an immediate thrombolysis in the medical emergency, he succumbed to the illness.
Discussion
Cyst rupture is a very serious problem in hydatid cyst and the development of new symptoms or worsening of the existing symptoms are the clues indicating rupture. Pulmonary embolism is a very rare complication of hepatic hydatid cyst rupture.[4] It most commonly occurs when one of the daughter cysts ruptures into the IVC, travelling through the right atrium and ventricle into the pulmonary artery. A similar case is reported in the literature where a 58-year-old female presented with chest pain and shortness of breath and was diagnosed with a ruptured hydatid cyst into the IVC with pulmonary embolism.[5] The pulmonary embolism in a hydatid cyst carries a very poor prognosis and surgery remains the treatment of choice. Thrombectomy is usually done but carries a very high postoperative mortality. Surgery can also be complicated by aneurysm, new embolus formation, anaphylactic shock, or hydatid dispersion to other tissue or organs. Medical therapy is not very effective however, it can be used if there are contraindications to surgery or a high risk of hydatid fluid leakage during surgery.
Another very unusual complication of hydatid cyst is hydropneumothorax, which can occur secondary to rupture of hepatic or lung hydatid cyst into the pleura. It occurs in 2%–4% of cases.[6] It carries high morbidity and mortality secondary to the high risk of anaphylactic shock. Superinfection is a common complication of a ruptured cyst and an air-fluid level is an important sign of superinfection. Most cases of hydropneumothorax have been attributed to the rupture of a lung hydatid cyst in the literature.[6] We could not come across any case report of hepatic hydatid cyst complicated by hydropneumothorax. Management involves tube thoracostomy or thoracotomy or video-assisted thoracoscopic surgery (VATS) to remove cyst remnants. Pleurectomy or decortication may be needed if significant pleural involvement is present.
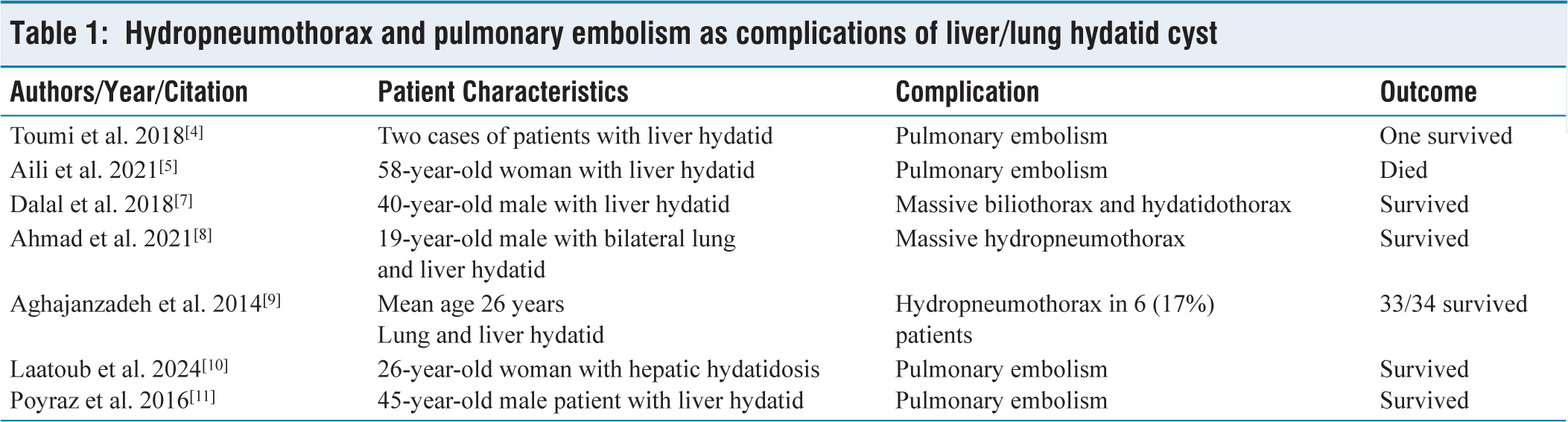
Patients presenting with both hepatic and lung hydatid cyst are managed through a single session transthoracic approach in which initially surgical intervention is performed for the cyst in the lung then hepatic hydatid cysts are approached through a radial incision in the diaphragm. The cysts are managed through various techniques including enucleation, peri cystectomy, and removal of intact hydatid cyst after needle aspiration or lobectomy of the lung. Table 1 lists some case reports of these two uncommon complications of ruptured liver/ lung cysts.
Hydropneumothorax and pulmonary embolism as complications of liver/lung hydatid cyst
Hydatid disease is widely distributed across India as influenced by animal husbandry practices, close human-animal contact, sanitation, and cultural factors. Historically, some states have reported some of the highest prevalence of human hydatid disease. These include Kashmir Valley, Andhra Pradesh, Tamil Nadu, Southern Rajasthan, Northern Chhattisgarh, Gujarat and South Maharashtra.[12] Ongoing efforts are crucial for effective management and prevention of this disease.
Our case was very unique and complex as the hepatic hydatid cyst ruptured simultaneously into the pleural cavity, leading to hydropneumothorax with dissemination of the cyst into the lung parenchyma and pulmonary embolism. This type of case has never been reported in the literature and is probably the first of its kind.
Conclusion
Cyst rupture is a critical complication of a hydatid cyst, often indicated by the emergence of new symptoms or the worsening of existing ones. Pulmonary embolism in hydatid disease is a serious complication that occurs when a hydatid cyst ruptures into the bloodstream, leading to embolisation of cystic material into the pulmonary circulation. This may lead to pulmonary infarction, secondary infection, and potential right heart failure. Hydropneumothorax is another rare complication that occurs when a pulmonary hydatid cyst ruptures into the pleural space. It has the potential to cause secondary infection, leading to empyema.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
A proper written consent is present, which was obtained from the patient’s relative for the use of the data related to this case.
Informed consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient’s relative has given consent for images and other clinical information to be reported in the journal. Patient’s relative understands that the patient’s name and initials will not be published and due efforts have been made to conceal the identity, but anonymity cannot be guaranteed.
Credit author statement
All the authors have made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data. All the authors have been involved in drafting the manuscript or revising it critically for important intellectual content and have given final approval of the version to be published. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content. The corresponding author takes responsibility for the article during the submission and review process.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Use of artificial intelligence
The authors declare that the manuscript has not been written using the AI generate.