
Abstract
Background:
The term ascites refers to the presence of excessive pathological fluid in peritoneal cavity. The term spontaneous bacterial peritonitis (SBP) is defined as the infection of ascitic fluid without any evidence of intra-abdominal, surgically treatable cause of infection. The importance of early detection of SBP is must as it develops in about 10%–30% patients and has high mortality rates.
Aims and Objectives:
To study diagnostic significance of ascitic fluid Lactate Dehydrogenase (LDH) levels in evaluation of SBP in patients with liver cirrhosis and to find a correlation between ascitic fluid LDH and serum LDH in SBP and non-SBP cirrhotic patients.
Materials and Methods:
This is a cross-sectional observational study done at the Department of Medicine, Sri Guru Ram Das Institute of Medical Sciences and Research, Sri Amritsar, where 152 subjects were taken and were divided into SBP (n = 45) and non-SBP group (n = 107). Ascitic fluid analysis (diagnostic paracentesis) was done, and samples were sent for cytology, biochemistry and culture sensitivity.
Results:
It was observed that ascitic fluid LDH in patients with SBP had median (IQR) value of 308 U/L (233–641) as compared to 102 U/L (83–124) in non-SBP group (P < .01). The median (IQR) of ascitic fluid LDH to Serum LDH was 1.2 (0.74–1.96) in the SBP group as compared to 0.35 (0.27–0.46) in the non-SBP group (P < .01).
Conclusion:
The results of our study suggest that ascitic fluid LDH and ascitic fluid LDH to serum LDH ratio can be used as a diagnostic marker for SBP in patients with cirrhosis of liver.
Introduction
Excessive pathological fluid in the peritoneal cavity is referred to as ascites. Many diseases can lead to the formation of free fluid in the peritoneal cavity, most commonly being the portal hypertension caused by cirrhosis (80%). The first sign of decompensation in a patient with cirrhosis is ascites, and mortality in decompensated liver disease increases and it is usually from complications such as spontaneous bacterial peritonitis (SBP) and hepatorenal syndrome. Mortality is usually between 15% in a year to 44% in 5 years.[1] Various mechanisms for ascites include portal hypertension, splanchnic vasodilation and hyperdynamic circulation, hypoalbuminemia and percolation of hepatic lymph in the peritoneal cavity.
The infection of ascitic fluid without any indication of an intra-abdominal, surgically curable cause of infection is known as SBP, a term that Harold Conn first used in the early 1970s.[2–4] About 10%–30% of individuals develop SBP, which has an estimated 20% in-hospital death risk among ascites patients who have been monitored for a year.[5,6] The most common organisms that cause SBP are gram-negative bacteria, and they include Escherichia coli and Klebsiella pneumoniae; however, in recent years, there has been a marked shift in the prevalence of patients with SBP due to gram-positive cocci, including Streptococcus pneumoniae, the Staphylococcus spp, and the Enterococcus spp.[7] The occurrence of SBP is associated with: ascitic fluid total protein less than 1 g/dL, total bilirubin greater than 2.5 mg/dL, variceal haemorrhage and a history of previous SBP, malnutrition and proton pump inhibitors.
Aims and Objectives
To evaluate the diagnostic value of Ascitic fluid Lactate dehydrogenase (LDH) levels in the diagnosis of SBP in patients with hepatic cirrhosis with ascites.
To correlate the levels of ascitic fluid LDH with serum LDH levels in patients with SBP and non-SBP related cirrhosis.
Materials and Methods
This is a cross-sectional observational study done at tertiary care centre in which 152 subjects were taken and were divided into the SBP and non-SBP groups.
Study period: July 2023 to February 2025.
Inclusion Criteria
All patients between 18 and 65 years with cirrhosis of liver with ascites as diagnosed clinically and radiologically.
Exclusion Criteria
Patients who were known cases of malignancy.
Patients with vascular diseases such as [Polyarteritis nodosa, Eosinophilic granulomatosis with polyangiitis (Churg-Strauss vasculitis), Granulomatosis with polyangiitis [Wegener’s], Behçet’s syndrome, Sarcoidosis].
Patients who were already on oral or IV antibiotics prior to admission were excluded from the study.
Patients having evidence of haemolytic anaemia with jaundice.
Pregnant women and those who have recently given birth (after 6 months from birth).
Methods
Patients with a diagnosed case of cirrhosis of liver, either clinically or radiologically (USG or C.T. abdomen), were taken, and these patients were subjected to ascitic fluid analysis (diagnostic paracentesis), before giving antibiotics. All the patients underwent paracentesis within 24 hours of admission, prior to antibiotic administration and ascitic fluid was collected in three sterile containers.
Ascitic fluid was sent in a sterile container for culture and sensitivity.
Ascitic fluid was sent to the biochemistry lab for biochemical examination (including total proteins, albumin and LDH levels)
Ascitic fluid was sent to pathology lab for cytological evaluation.
Other relevant blood investigations were also done, including serum LDH, CBC (complete blood count), LFT (including proteins), PTI, electrolytes, RFT, viral markers, and upper GI endoscopy.
CPS (Child Pugh Score) and MELD-Na scoring were done for all patients falling into either in SBP or non-SBP group.
Statistical Analysis
The data of this study were systematically organised, entered into a Microsoft Excel file and statistical analysis was performed by Statistical Package for Social Sciences version 26, to infer conclusions. Categorical data were expressed as numbers and percentages and were compared by Chi-square test. Parametric data were presented as Mean ± SD and analysed using Student t-test. Some of the data were not normally distributed. In response to these findings, a non-parametric test was applied, and the data were summarised using the median and interquartile range. To find the difference in the two groups, Mann-Whitney U test was applied. Pearson correlation was used to determine the correlation between fluid LDH with serum LDH and fluid/serum LDH. Statistical significance was defined by a value of P < .05 as significant, while P ≤ .001 was considered highly significant.
Results
A total of 152 subjects with cirrhosis of liver with ascites were taken, out of which 45 subjects fell into SBP category and 107 subjects fell into non-SBP category. Maximum subjects belongs to 41–50 years age, which accounts for 53 cases (34.9% of the total population). It was followed by subjects in 51–60 years age group, representing 41 cases (27% of the total population) and 31–40 years age group with 28 cases (making up 18.4%). Individuals aged 61 and older account for 25 cases (16.4% of the total population) while those aged 30 and younger account for only 5 cases, representing 3.3% of the total population. Similar results were seen in both SBP and non-SBP categories. Out of 45 individuals having SBP, 5 were female (11.11%) and 40 were male (88.89%). Conversely, of the 107 subjects without SBP, 16 were female (14.95%) and 91 were male (85.05%).
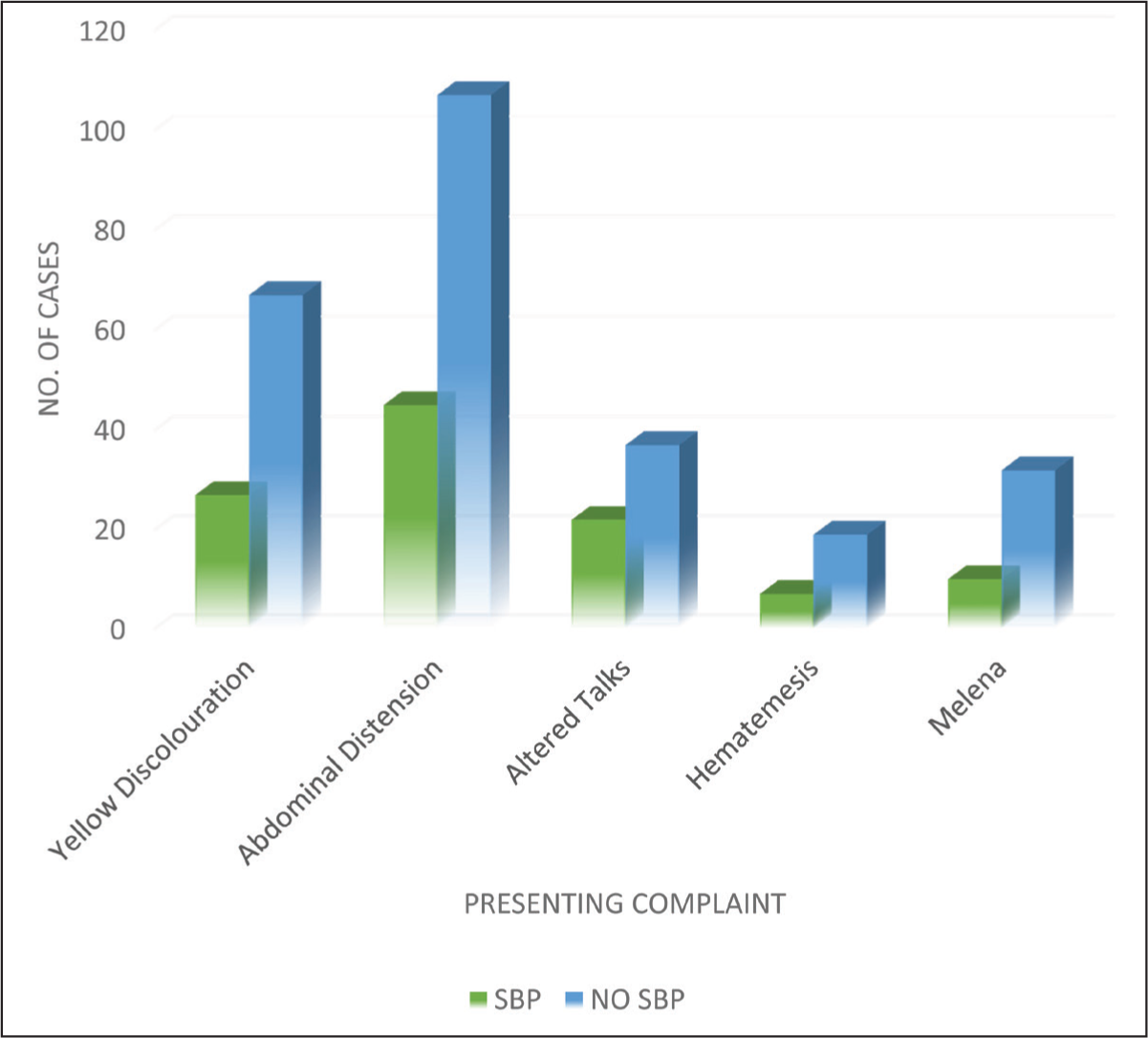
Clinically, yellow discolouration affected 94 subjects, with 27 subjects (28.72%) having SBP and 67 subjects (71.3%) in those who did not have SBP. Abdominal distension was present in all the subjects. Altered talks were present in 59 individuals, amongst which 22 subjects (37.29%) had SBP while 37 (62.7%) subjects did not have SBP. Melena and hematemesis show the lowest numbers of 42 (27.6%) and 26 (17.1%) cases, respectively [Figure 1].
Distribution of study subjects according to presenting complaints
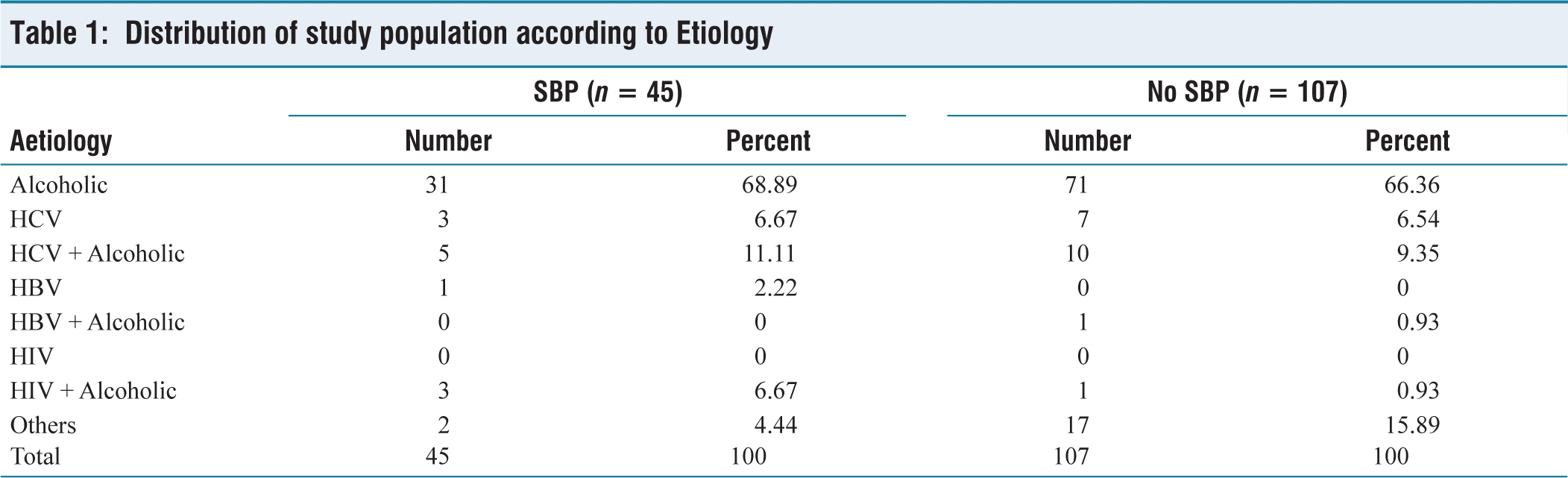
Alcohol (68.89%, n = 31 in SBP group and 66.36%, n = 71 in non-SBP group) was the most common etiological factor among the subjects followed by subjects who were alcoholic and had chronic hepatitis C (11.11%, n = 5 in SBP group and 9.35%, n = 10 in non-SBP group), followed by chronic hepatitis C (6.67%, n = 3 in SBP group and 6.54%, n = 7 in non-SBP group) [Table 1].
Distribution of study population according to Etiology
Liver function tests were deranged in majority of subjects. 38 subjects from SBP category (84.44%) and 81 subjects from non-SBP category (75.70%) had hyperbilirubinemia. In SBP category, 64.44% (n = 29) and 62.62% (n = 67) subjects had hyponatremia (sodium levels <135 mEq/L) and hypernatremia (sodium levels >145 mEq/L) was seen in very few subjects (6.67%, n = 3 in SBP and 0.94%, n = 1 in non-SBP). In the SBP group, 51.11% (n = 23) subjects had low platelet count and 31.78% (n = 34) subjects from non-SBP group had low platelet count. Out of total, 134 patients had hypoalbuminemia. In SBP group, 91.11% (n = 41) subjects had hypoalbuminemia and 86.91% (n = 93) subjects from non-SBP group had hypoalbuminemia.
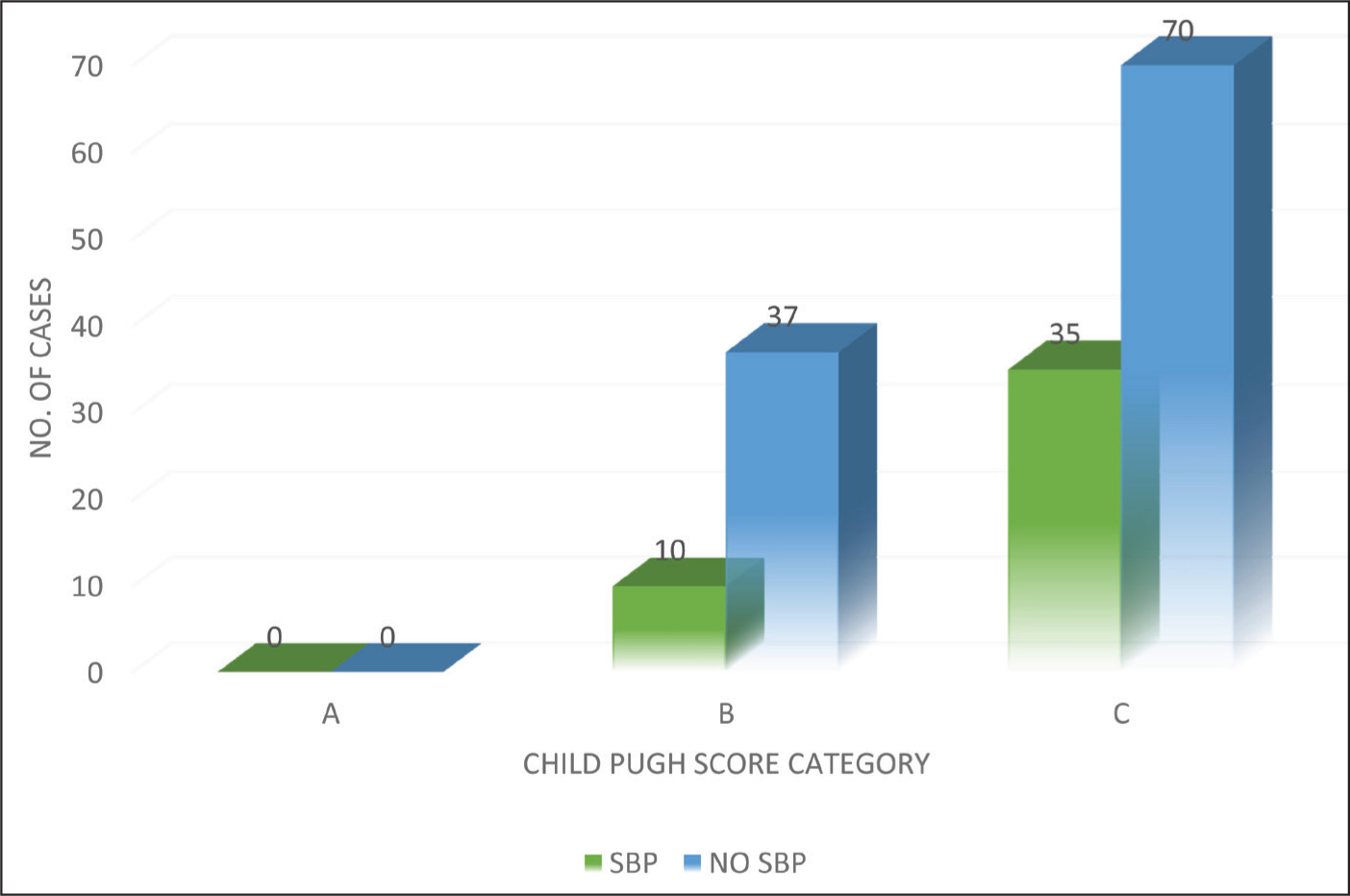
22 subjects (48.89%) from SBP group and 43 subjects (40.19%) from non-SBP group had splenomegaly. 3 subjects (6.66%) from SBP category and 12 subjects (11.22%) from non-SBP category do not have oesophageal varices, 17 subjects (37.78%) from SBP category and 59 subjects (55.14%) from non-SBP category had oesophageal small varices, 25 subjects (55.56 %) from SBP category and 36 subjects (33.64%) from non-SBP category had large oesophageal varices. Among 45 subjects with SBP, 10 subjects (22.22%) fall in CPS class B, and 35 subjects (77.78%) fall in CPS class C, indicating severe liver dysfunction. In contrast, among the 107 subjects without SBP, 37 subjects (34.58%) fall in CPS class B, and 70 subjects (65.42%) fall in CPS class C. No individuals fall CPS class A in both SBP and non-SBP group [Figure 2].
Distribution of study population according to Child Pugh score in liver cirrhosis
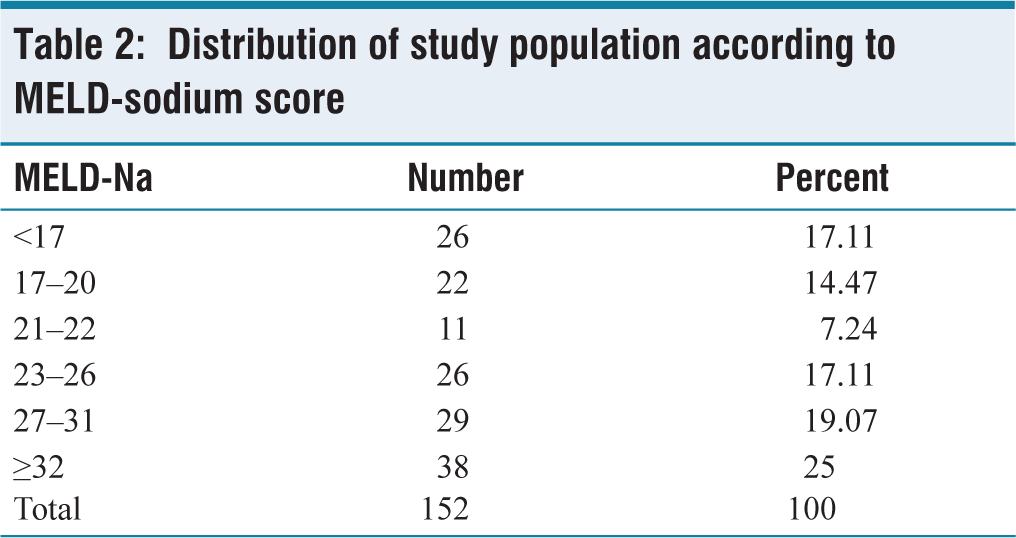
On the basis of MELD-Na scoring, 25% (n = 38) subjects had MELD-Na score of ≥32, suggesting severe liver disease, 19.07% (n = 29) subjects had MELD-Na score of 27–31. The scores <17 and 23–26 account for each 17.11% (n = 26) of the sample, whereas 22% (n = 14.47) and 11% (n = 7.24) had MELD-Na scores ranging from 17–20 and 21–22, respectively [Table 2].
Distribution of study population according to MELD-sodium score
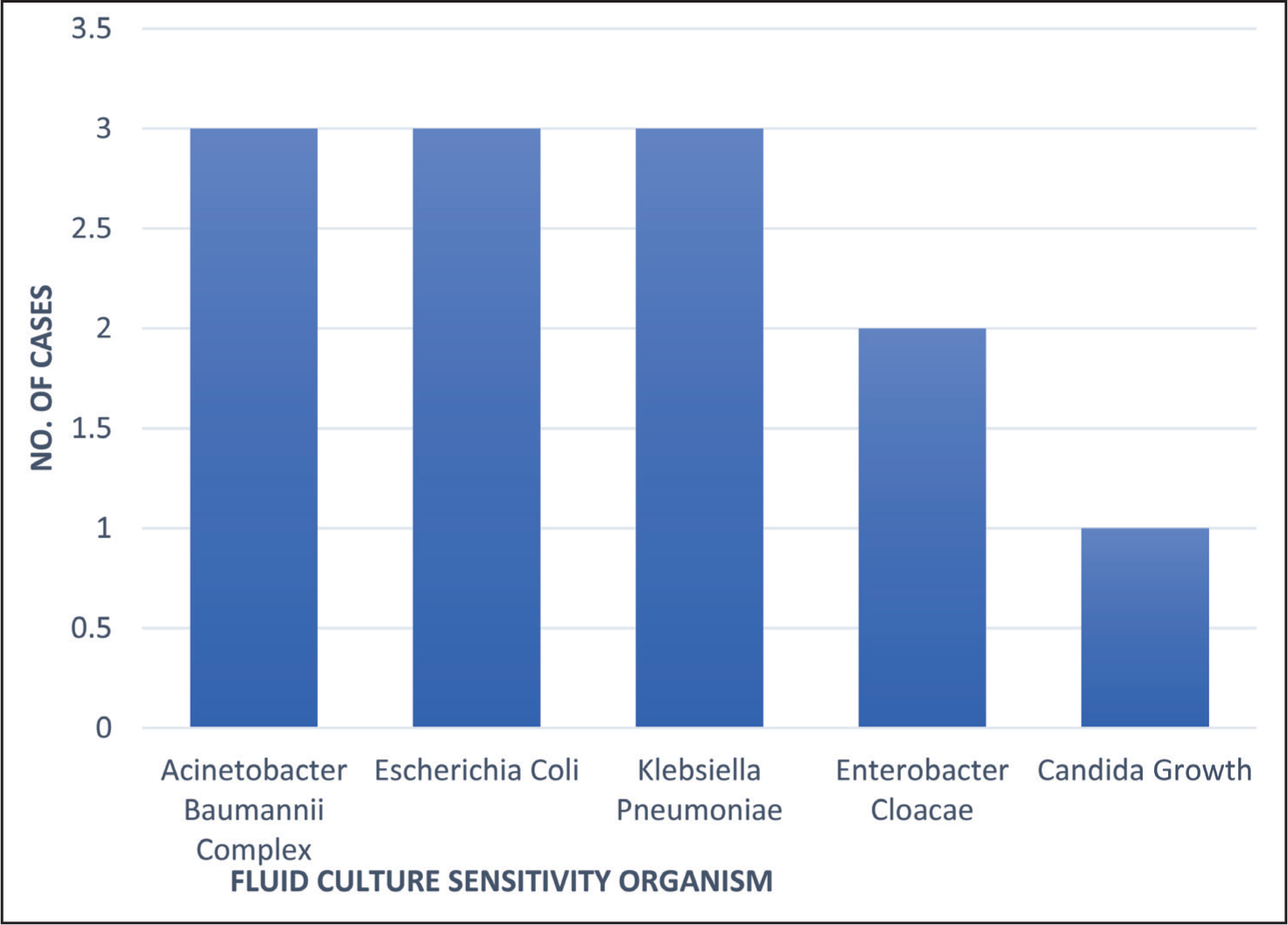
Out of the 45 SBP-positive cases, 33 subjects (73.3%) fulfil cytology criteria (Culture-negative neutrocytic ascites) while 6 subjects (13.33%) have positive growth in culture (Monomicrobial non-neutrocytic bacterascites), and another 6 subjects (13.33%) fulfil both culture and cytology criteria. None of the subject follows polymicrobial bacterascites (PMNA) criteria. Out of them, total of 12 cases (26.66%) showed growth in their fluid culture. Among the cases with positive cultures, Acinetobacter baumannii complex, E. coli, K. pneumoniae were positive each in 3 cases (25%) each, while Enterobacter Cloacae was positive in 2 cases (16.67%), and Candida growth was found in 1 case (18.33%). This suggests that while most SBP-positive individuals did not show microbial growth, the cases that did have growth were primarily associated with bacterial pathogens like Acinetobacter, E. coli, and Klebsiella and Candida being a less frequent cause [Figure 3].
Distribution of study population according to fluid culture sensitivity
The median (IQR) ascitic fluid LDH in SBP patients was 308 U/L (233–641) versus 102 U/L (83–124) for no-SBP group (P < .01). The Ascitic fluid LDH to Serum LDH ratio was higher in SBP as compared to non-SBP group. The median (IQR) Ascitic fluid LDH to Serum LDH was 1.2 (0.74–1.96) in SBP group and 0.35(0.27–0.46) in the non-SBP (P < .01) [Table 3].
Comparison of median (IQR) values of LDH in SBP and non-SBP patients

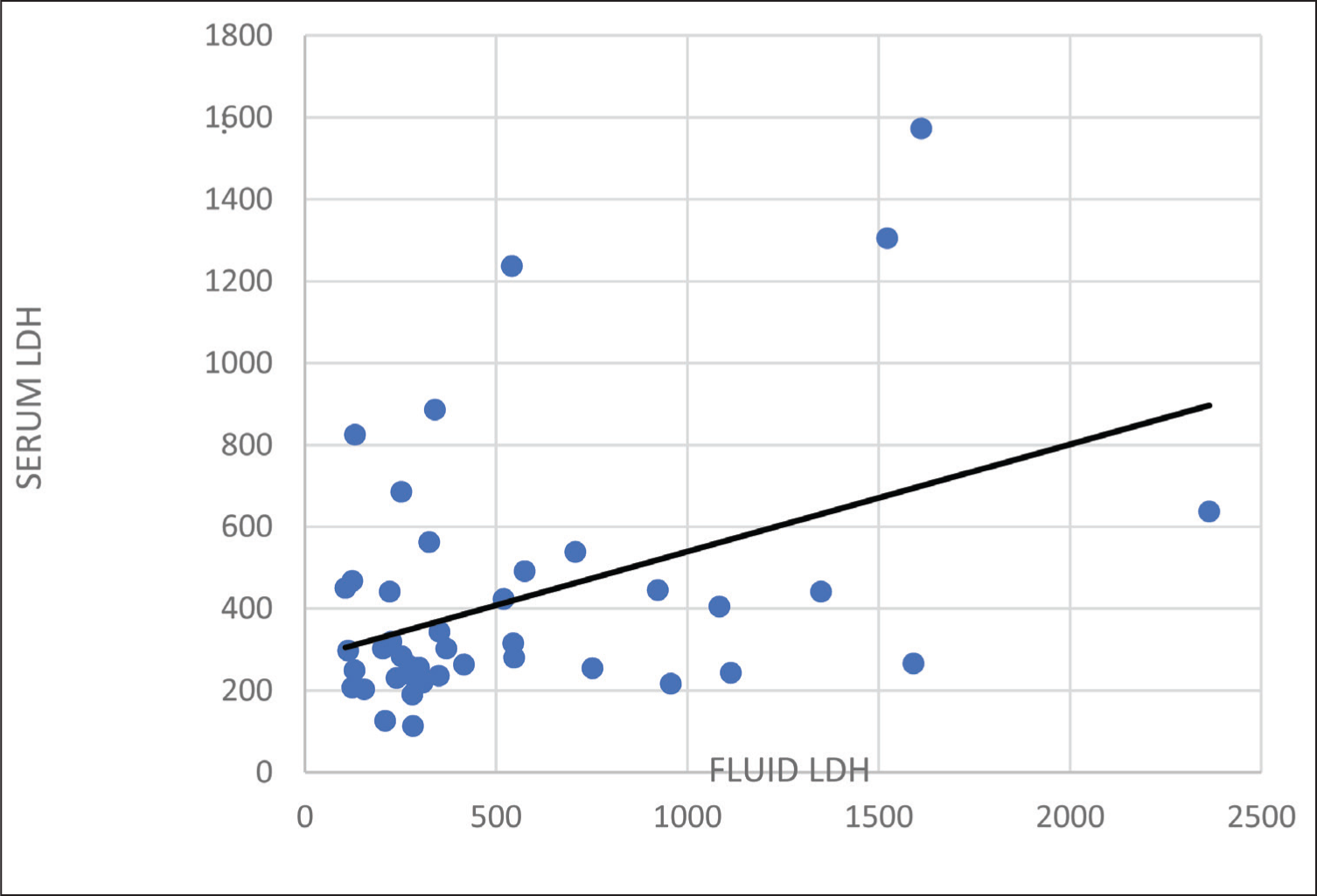
Figure 4 shows that there is a moderate positive correlation between serum LDH and fluid LDH (r = 0.420), which is statistically significant (P = .004), suggests that as serum LDH increases, fluid LDH also tends to increase.
Correlation between fluid LDH and serum LDH in patients with liver cirrhosis
Discussion
LDH is an enzyme used in conversion of pyruvate to lactate and is a marker of tissue damage in the body. SBP occurs due to translocation of bacteria from intestine. Gut bacteria can cross intestinal wall, enter into lymphatics, seeding and proliferating in peritoneum. As there are high mortality rates in patients with SBP, so early and correct diagnosis is of utmost importance. In this study, 152 subjects were taken, out of which 45 subjects had SBP (12 of them were culture positive) and 107 were non-SBP subjects. Ascitic fluid analysis was done in all of these subjects.
In the study done by S Sandhya et al.[8] (2021), it was found that patients with SBP had significantly raised ascitic fluid LDH (P = .001). The median (IQR) in SBP group was 201 IU/L (118–921.5) as compared to 74 IU/L (48 128) in non-SBP group. The ratio of ascitic fluid LDH to serum LDH was also significantly high in the SBP group. The median (IQR) of ascitic fluid LDH to serum LDH ratio was 0.50 (0.31–1.11) in the SBP group as compared to 0.24 (0.15–0.42) in the non-SBP group (P < .001). In 2015, El Motasem et al.[9] revealed group B patients (SBP group) exposed a significantly high ascites inflammatory response than group A (non-SBP group) established by additional ascitic fluid LDH (IU/L) (185.06 ± 58.39 IU/L vs. 84.37 ± 33.65 IU/L mean ± SD, respectively, P < .001). In 2012, Kamal et al.[10] found that LDH levels of ascitic fluid were pointedly higher in patients of group I (SBP group) with mean value of 208.733 ± 52.340 as compared to the patients in group II (non-SBP group) with mean value of 147.733 ± 49.264. Mortada et al.[11] in their study reported that out of 30 patients of ascites, 13 had SBP and the ascitic fluid LDH was significantly higher in this group as compared to the non-SBP group (P < .002). Khan et al.[12] noted statistically significant difference in levels of ascitic fluid LDH in SBP group (239.81 ± 159.26) as compared to non-SBP group (65.47 ± 28.75). Ascitic fluid LDH/serum LDH ratio for SBP was 0.65 ± 0.21 and for non-SBP was 0.18 ± 0.12 (P < .001). Amany Talaat et al.[13] noted that ascitic fluid LDH level was significantly higher in patients of SBP (group I) as compared to those in non-SBP group (group II) (P of .003). Touny et al.[14] described that out of 41 cirrhotic patients with ascitic fluid, 5 cases fulfilled the criteria for SBP. Three of these five had culture-positive neutrocytic ascites, and two were negative for culture, but cytology criteria were positive. In the SBP group, the ratio of ascitic fluid LDH to serum LDH > 0.75 as compared with < 0.58 in non-SBP group. In comparison to other studies, higher ascitic fluid LDH levels and a greater ratio of fluid LDH/serum LDH were observed in patients with SBP than those who did not have SBP.
In 2012, Kamal et al.[10] revealed in their study that out of 15 patients, there were five patients with negative culture (CNNA); ten were culture positive. Of these 10 positive cultures, 8 (i.e., 80%) were caused by Gram-negative Enterobacteriaceae (five E. coli and three K. pneumoniae) and 2 (i.e., 20%) by Gram-positive cocci (one Staphylococcus aureus and one S. pneumoniae). In the study by Ning et al.[15] Gram-negative bacteria accounted for 68.1% of all pathogens. The pathogens responsible for this were E. coli (n = 267, 40.7%), Streptococcus spp. (n = 110, 16.8%), Klebsiella spp. (n = 87, 13.3%), Enterococcus spp. (n = 66, 10.1%), coagulase-positive staphylococci (n = 25, 3.8%), Enterobacter spp. (n = 20, 3.0%), and Acinetobacter spp. (n = 18, 2.7%).
Conclusion
Ascitic fluid LDH had higher median (IQR) in patients with SBP than in those without it. The result from our study suggested that the Ascitic Fluid LDH and Ascitic Fluid LDH to Serum LDH ratio can be used as biochemical test for the SBP in patients with liver cirrhosis. From this study, it can be seen that, in order to make an early and prompt diagnosis for SBP, routine ascitic fluid LDH and ascitic fluid LDH to Serum LDH ratio can be done (as for bacteriological identification we still need to wait 2–3 days for the culture reports, and there is inter-observer variation in cytological investigation) and early treatment can be started so that the length of hospital stay may be reduced, and mortality rates among such patients might also drop.
Limitations
The current study had certain limitations.
The investigation was conducted at a single location. To understand the diversity of this biochemical marker in individuals of different races, ethnicities, and geographic locations, we will require multicentric studies in the future that involve patients from various geographic locations.
Since the sample size was small, additional research with a bigger sample size is required to validate our findings.
Because of financial concerns, additional testing (such as a liver biopsy or fibro scan) was not performed in cases where there was no cause for cirrhosis.
Footnotes
Acknowledgements
First, I thank Almighty, my professor and associate professor Dr Surinder K. Salwan and Dr Jasmine Kaur and my parents S. Maninderpal Singh and Mrs. Parmjit Kaur, my brother S. Arshdeep Singh, who has been continuous source of inspiration and motivation for me. Without them, I could never have reached this current level of success. I owe a special thanks to my seniors Dr Manavdeep Kaur, Dr Parul Khanna, Dr Rishabh Rikhye, Dr Sukhjit Kaur, Dr Mehak Kaleka. Their encouragement and moral support have been my driving force.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The study carried out in this manuscript is approved by the institutional ethics committee, Sri Guru Ramdas Institute of Medical Sciences & Research (SGRDIMSR), Amritsar, Punjab. (SGRD/IEC/2023-215).
Informed consent
All patients were informed and informed consent was taken.
Credit author statement
Dr Gagandeep Singh prepared the first draft, data collection, data analysis, manuscript review and editing.
Dr Jasmine Kaur, Dr Surinder K. Salwan, Dr Punita Sharma supervised, provided overall guidance, finalized the study.
All authors read and gave final approval of the version to be submitted.
Data availability
Data are available within manuscript.
Use of artificial intelligence
Not used.