
Abstract
Background:
The dissipated overuse of antibiotics plays a major role in the emergence of antibiotic resistance. Empirical antibiotic therapies are often guided by local endemic patterns, which are not widely documented in many areas, including our study region. This research aims to assess local antibiotic resistance patterns and promote awareness of antimicrobial stewardship practices.
Methods:
An institutional-level cross-sectional observational study was carried out involving patients admitted to general medicine wards with suspected systemic bacterial infections. The study examined in-hospital mortality and extended hospital stays in connection with various patient characteristics and antibiotic-related factors. Data analysis was performed using descriptive statistics and binary logistic regression. Adjusted odds ratios (AOR) with 95% confidence intervals were calculated, with statistical significance set at P < .05.
Results:
Pneumonia was identified as the most prevalent condition, accounting for 26.1% of cases. The combination of piperacillin and tazobactam emerged as the most frequently used antibiotic regimen, administered in 40.9% of cases. Prolonged antibiotic usage (OR = 5.74) and immunocompromised status (OR = 3.18) were significantly associated with adverse hospital outcomes, including extended length of stay and higher mortality rates.
Conclusion:
Empirical antibiotic use was largely appropriate, though instances of misuse highlight the need for improved stewardship. Prolonged antibiotic use and immunocompromised status were linked to worse outcomes, underlining the importance of policy-driven antimicrobial oversight and localised prescribing guidelines to combat resistance and improve hospital care quality.
Keywords
Introduction
Antibiotics are a cornerstone of modern medical practice. The increasing prevalence of systemic bacterial infections in healthcare settings poses significant challenges for patient management and outcomes. Antibiotics have revolutionised the treatment of these infections, yet their misuse and overuse have led to alarming rates of antibiotic resistance, complicating clinical practices and threatening public health.[1] Prescribing antibiotics inappropriately can harm patients and lead to the growth of resistant bacteria, which can cause more severe illnesses leading to higher death rates.[1,2]
In the United States, antimicrobial resistance (AMR) leads to 2.8 million infections every year, contributing to 35,000 deaths and costing the economy around $55 billion.[2] In Europe, antibiotic-resistant infections lead to around 25,000 deaths annually imposing an economic burden of approximately €1.5 billion. Acknowledging the seriousness of this issue, the World Health Organization (WHO) has highlighted AMR as a major global public health threat, driving significant morbidity, mortality and rising healthcare costs. Antibiotic-resistant pathogens are becoming an increasingly difficult challenge to treat.[3]
The use of antibiotics is guided by presenting symptoms and often adjusted based on culture sensitivity reports to minimise microbial resistance to empirical antibiotics. Patient outcomes serve as key indicators of hospital service quality. While antibiotic resistance is a worldwide concern, it manifests as a local challenge where endemic bacteria frequently show resistance to commonly used drugs.[4–6] Indiscriminate antibiotic use contributes to resistance and increases healthcare costs, particularly in resource-limited settings.[7] Identifying predictors of hospital outcomes and understanding antibiotic use patterns can guide rational prescriptions, optimise resource allocation and aid in the development of effective antibiotic use optimisation strategies. In tertiary care teaching healthcare institution, where complex cases are common, understanding the patterns of antibiotic usage and their impact on hospital outcomes is critical.[8] This study aims to evaluate the current practices of antibiotic use in individuals suspected of having systemic bacterial infections, with an emphasis on determining factors that affect clinical outcomes.
Materials and Methods
A two-month cross-sectional observational study was carried out at a tertiary care teaching hospital, from August 19, 2022 to October 18, 2022. The study included all individuals hospitalised in the adult internal medicine wards with suspected systemic bacterial infections throughout the specified period. A similar study conducted in Ethiopia involved 369 patients with systemic bacterial infections over three months.[9] Taking into consideration a 95% confidence interval (CI) and a P value of .05, a sample size of 385 participants was estimated for the two-month study. The final study population consisted of 379 patients, reflecting the hospital’s average daily admission of 70–80 individuals in the internal medicine department. A complete enumeration was done encompassing all patients suspected of having systemic bacterial infections and admitted to the internal medicine ward throughout the study period.
Inclusion Criteria
The study included patients aged 18 years and above who were admitted under the care of adult internal medicine team with suspected systemic bacterial infections and provided their consent to participate.
Exclusion Criteria
Participants were excluded if they had been on antibacterial therapy for less than 72 hours, were younger than 18 years or were receiving anti-mycobacterial drugs, local antibacterial agents or preventive antibacterial therapies.
Study Technique
The dependent variables in this study were in-hospital mortality and extended hospitalisation duration. Independent variables included socio-demographic characteristics (such as age and sex), illness-related factors (e.g., infection type and immunocompromised status), drug-related factors (e.g., types of antibiotics used, modifications to initial treatment and antibiotic metrics) and quality indicators assessing treatment suitability.
Data Collection Process
Patients presenting with or developing systemic bacterial infections (excluding mycobacterial infections) during their hospital stay were closely monitored. Information gathering for new admissions and ongoing follow-up updates was conducted regularly through patient chart reviews and consultations with attending physicians. Information such as demographic details, admission and suspected infection diagnoses, laboratory procedures performed (e.g., cultures and Gram staining) and the dates of laboratory reports were meticulously recorded. Additionally, data on antibiotics given, subsequent modifications to antibiotic regimens and the relevant start and adjustment dates were systematically documented. Microsoft Excel was used to organise data in spreadsheet format.
Statistical Analysis
The data were analysed using SPSS version 29.0 for Windows. Descriptive statistics along with binary logistic regression methods were employed in the analysis. Variables with a P value ≤ .05 in univariate models were considered in the multivariable logistic regression to adjust for potential confounders. Adjusted odds ratios (AOR) with 95% CIs were estimated, and statistical significance was determined at P < .05.
Ethical Considerations
The study was conducted following approval from the Institutional Ethics Committee (IEC). Since data collection relied mainly on patient charts, informed consent was obtained from those patients who agreed to participate in the study. To ensure confidentiality, patient and prescriber identifiers, including names, were not recorded.
Operational Definitions
Antibiotic days: The number of days a patient was administered systemic antibiotics.
Prolonged length of stay: A patient was in hospital ward for >14 days.
Antibiotic metrics: Addresses the following information about an antibiotic (a) number of days used, (b) use of other antibiotics with that antibiotic, (c) change of the antibiotic.
Appropriateness of therapy: It is based on (a) cultural sensitivity (CS) report available for the patient (b) continuation of the same therapy.
Results
The mean age among the patients was 45.5 ± 18.4 years (range: 18–84), with males comprising 51.2% of the study population. Approximately 35.6% of patients had completed secondary-level education. Among the participants, 49.6% were Muslim, followed by 46.2% who were Hindu. The 30–44-year age group accounted for 30.9% of the patients.
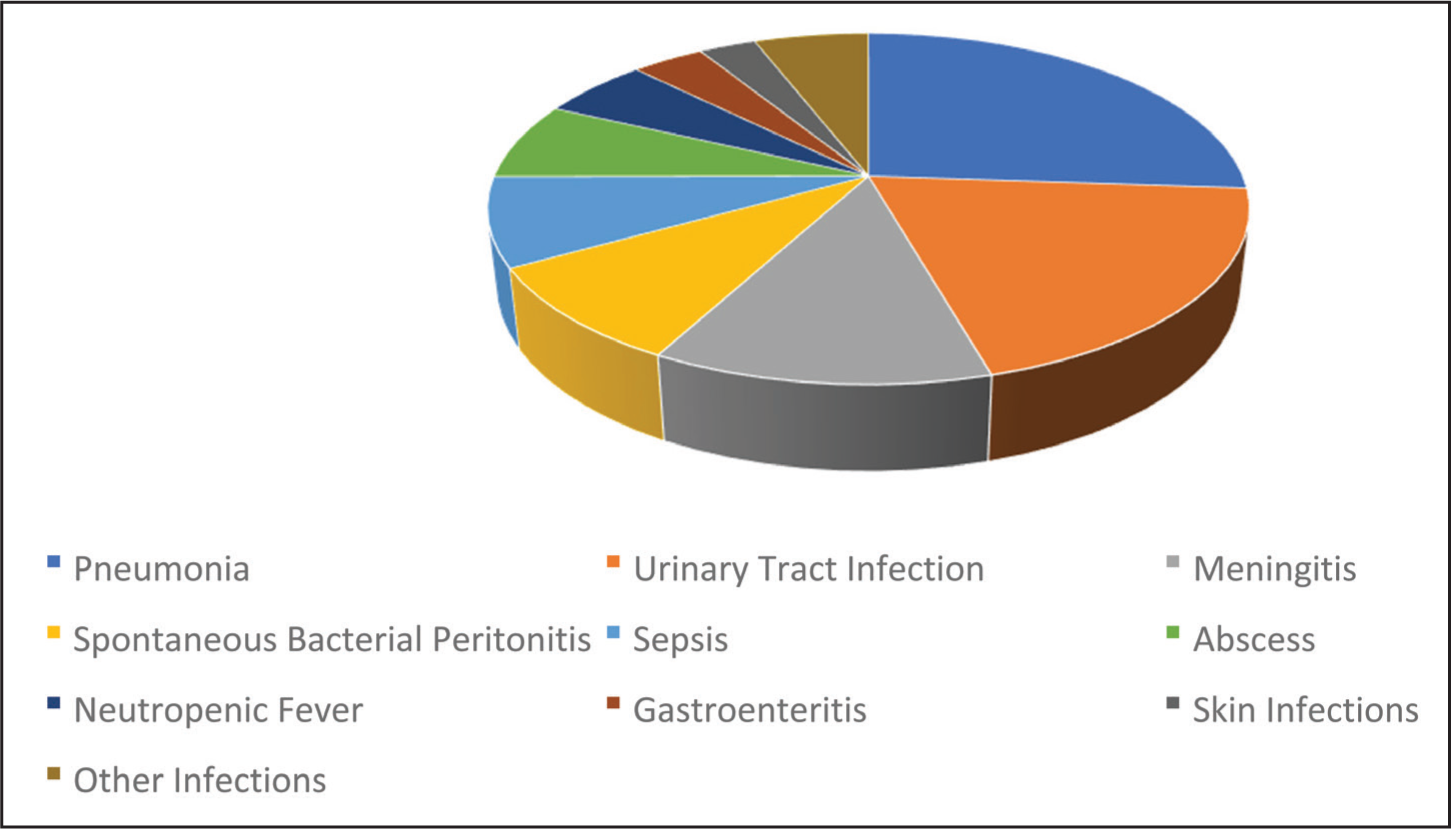
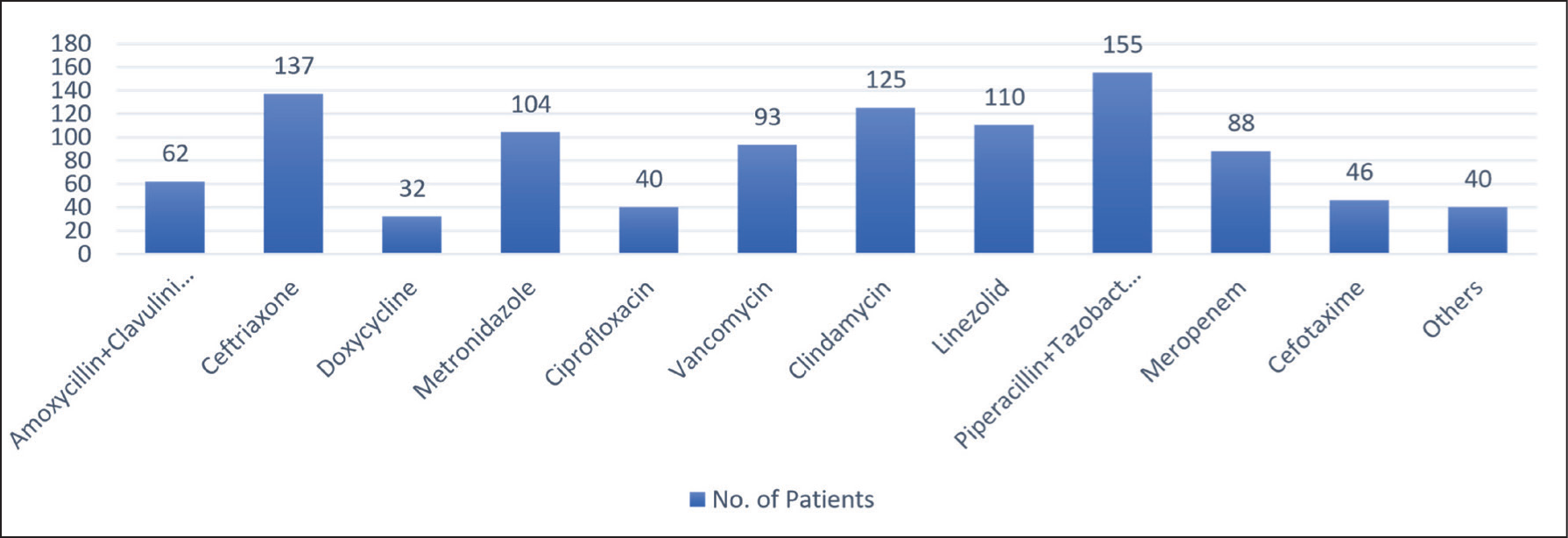
Pneumonia was the most prevalent primary infection diagnosis, observed in 26.1% of cases, followed by urinary tract infections, which accounted for 19.5% of cases [Figure 1]. The most frequently prescribed antibiotics were a combination of piperacillin and tazobactam (40.9%), followed by ceftriaxone (36.1%) and clindamycin (33%) [Figure 2]. When grouped by class, cephalosporins (47.3%), anti-anaerobic agents (38%) and glycopeptides (vancomycin only) (24.9%) were the most commonly used drug classes. Patients received one to three courses of antibiotics, averaging two or more courses per patient, and were typically prescribed two antibiotics simultaneously. The duration of antibiotic use was 9.6 ± 6.75 days, with a median of 8 days.
Distribution of primary infection diagnosis
Uses of antibiotics in medicine wards
Empirical therapy was initiated in all patients (100%). Adjustments based on CS reports were made in 23.5% of patients. CS reports were obtained prior to antibiotic initiation in 50.4% of admitted patients. Gram-positive and gram-negative organisms were covered in 68.3% of cases. Throughout treatment, single antibiotics were used for 16.9% of patients, two antibiotics for 53.6% and three or more antibiotics for 29.6%. The in-hospital mortality rate among patients with systemic bacterial infections was 28.8%. The mean duration of hospitalisation was 9.63 ± 6.75 days (range: 3–31).
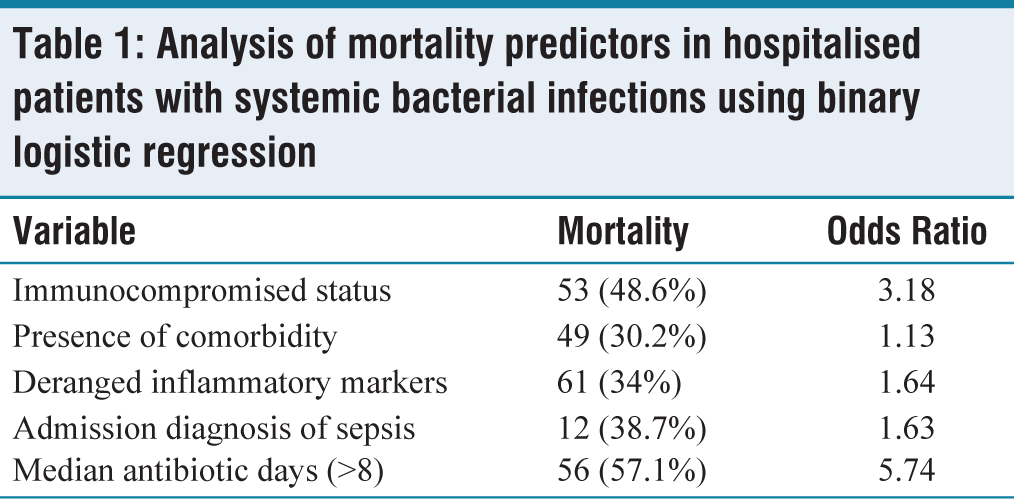
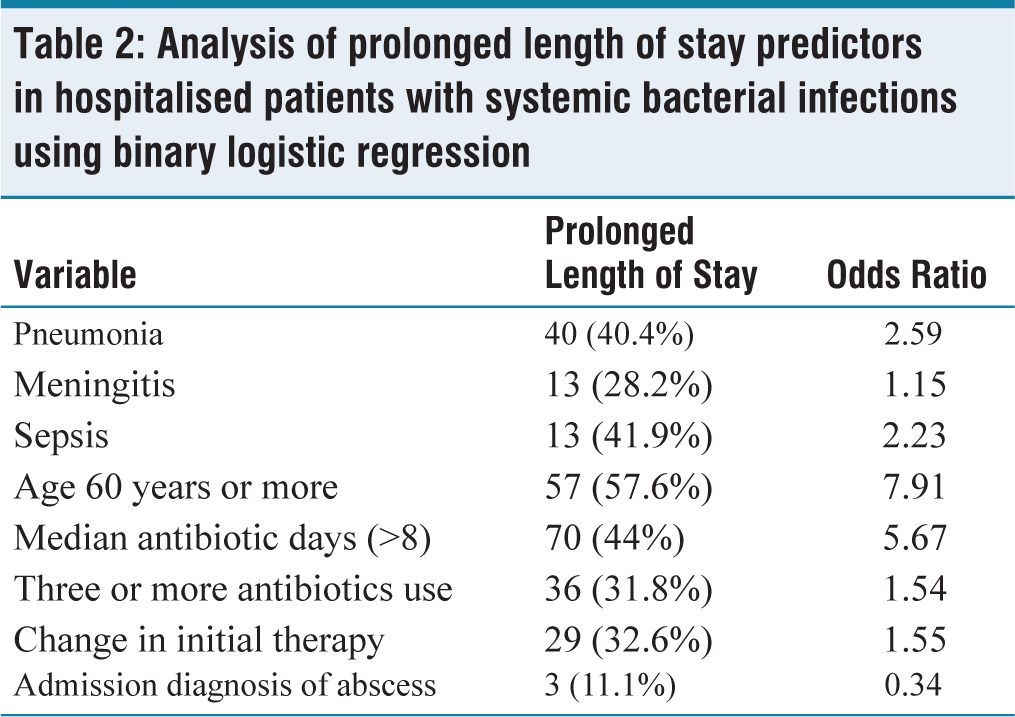
Negative predictors of in-hospital mortality included immunocompromised status, comorbidities, deranged inflammatory markers, antibiotic duration exceeding eight days and an admission diagnosis of sepsis [Table 1]. Prolonged hospital stays were associated with diagnoses of pneumonia, sepsis and meningitis, as well as age over 60 years. Other contributing factors included median antibiotic days (>8), changes to initial therapy and concurrent use of three or more antibiotics. Conversely, admission diagnoses of abscesses were negatively associated with prolonged stays [Table 2].
Analysis of mortality predictors in hospitalised patients with systemic bacterial infections using binary logistic regression
Analysis of prolonged length of stay predictors in hospitalised patients with systemic bacterial infections using binary logistic regression
Discussion
Our study included 379 patients, of whom 51.2% were male. Mean age of the study population was 45.5 years, with 117 patients (30.8%) belonging to the 30–44-year age group. The majority (35.6%) had education up to the secondary level, and 49.6% of the population were of Muslim faith. The observed in-hospital mortality rate of 28.8% among patients with suspected systemic bacterial infections in our tertiary care teaching hospital aligns with findings from similar studies in India and Ethiopia.[9–11] A multicentre prospective registry involving 1,172 intensive care unit (ICU) patients across 19 Indian centres reported an overall hospital mortality rate of 36.3%.[10] Specifically, mortality was 25.6% among patients with sepsis without shock and 50.8% among those with septic shock. The study highlighted that infections caused by carbapenem-resistant organisms were associated with higher mortality rates (31%) compared to carbapenem-sensitive infections (21%). In another study by Garg et al. which included 400 adult ICU patients with sepsis.[11] The 28-day mortality rate was reported at 40%, with 38% of deaths occurring within the first 48 hours of ICU admission.
Pneumonia emerged as the most prevalent infection among inpatients, aligning with findings from studies in low- and middle-income countries.[12] Cephalosporins were the most frequently used antibiotic class, consistent with hospital trends reported in other studies.[13] Empirical antibiotic therapy was initiated for all patients based on local sensitivity patterns, and initial therapy was modified in 23.5% of cases after adjustments with CS reports. Approximately 49.5% of CS reports were available within three days of initiating antibiotic therapy. The universal initiation of empirical therapy suggests a reliance on clinical judgment over microbiological confirmation. While empirical therapy is essential for timely intervention in systemic infections, the underutilisation of CS reports is a concern. In our study, culture testing was either delayed or not performed in several cases due to resource constraints or clinical urgency. This highlights an area for improvement—specifically, reinforcing timely specimen collection before antibiotic initiation and integrating CS data into therapy adjustments. Enhancing laboratory support and streamlining communication between clinicians and microbiology units could significantly improve targeted therapy rates.
The hospital lacked specific antibiotic usage guidelines derived from stewardship programmes; instead, antibiotics were administered according to local endemic patterns. The association of certain antibiotic use with prolonged hospital stays highlights the need for improved stewardship practices. The median length of hospital stay was eight days, comparable to data from European countries.[14,15] This indicates the presence of effective diagnostic and therapeutic protocols, potentially aided by lower prevalence of multidrug-resistant pathogens or good susceptibility to empirical therapies in the local setting.
In this study, the administration of vancomycin was linked to an increased mortality rate of 40.9%. No other studies have corroborated this finding, which may be due to the inappropriate administration of this antibiotic in the healthcare facility.[16] The elevated mortality risk associated with vancomycin use warrants careful interpretation. Vancomycin is typically reserved for severe or resistant gram-positive infections, often used in critically ill patients, which may explain the higher mortality. However, inappropriate use—such as lack of dosing adjustments in renal impairment, delayed initiation, or empirical use without confirmed indication—could contribute to poor outcomes. This highlights the need for stricter antibiotic stewardship protocols, including therapeutic drug monitoring (TDM) and prescriber education to ensure appropriate vancomycin use. Prolonged antibiotic use (>8 days) was related to a significantly higher mortality rate of 57.1% (OR = 5.74, 95% CI: 4.21–8.57, P = .027), likely due to the emergence of antibacterial-resistant strains or hospital-acquired infections.[17] The immunocompromised status of patients emerged as a strong predictor of hospital outcomes, with a mortality rate of 48.6% (OR = 3.18, 95% CI: 1.21–5.57, P = .004).[18] Admission diagnoses of sepsis were also significant predictors of mortality in the internal medicine ward (OR = 1.63, 95% CI: 1.17–3.85, P = .047).[19] Deranged inflammatory markers, including erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), ferritin and d-dimer were associated with adverse hospital outcomes (OR = 1.64, 95% CI: 1.45–2.19, P = .04). Similar outcomes regarding inflammatory marker derangements have been observed in recent coronavirus disease 2019 (COVID-19) outbreaks.[20] The presence of comorbidities among admitted patients was a weaker predictor of hospital outcomes, with an OR of 1.13 (95% CI: 0.62–2.57, P = .038), consistent with studies conducted in Spain.[21]
This study revealed that the diagnoses of pneumonia (OR = 2.59, 95% CI: 1.12–5.99, P = .026), meningitis (OR = 1.15, 95% CI: 1.01–2.63, P = .06) and sepsis (OR = 2.23, 95% CI: 1.24–3.54, P = .026) were associated with prolonged hospital stays. While no studies supporting these findings were identified, this gap highlights the need for further research in these areas. The use of vancomycin (OR = 9.46, 95% CI: 7.12–12.83, P = .007), clindamycin (OR = 2.86, 95% CI: 2.12–3.61, P = .046) and linezolid (OR = 2.35, 95% CI: 1.02–4.68, P = .036) was related to extended duration of hospitalisation. This could be attributed to their use in severe or terminal stages of infections.[16] Median antibiotic days exceeding eight days (OR = 5.67, 95% CI: 4.17–8.99, P = .004) indicated infection severity and served as a predictor of prolonged hospitalisation. These metrics can also inform the cost burden analysis of infectious diseases.[22,23]
The concurrent use of three or more antibiotics (OR = 1.54, 95% CI: 1.03–2.56, P = .07) was positively associated with extended hospital stays (>14 days). Similar findings were observed in a multicentre study conducted in the Netherlands.[24] Conversely, the diagnosis of abscesses (OR = 0.34, 95% CI: 0.21–0.57, P = .001) was negatively associated with prolonged hospital stays, consistent with findings from a hospital in Plymouth.[25] This study highlights the need for the local optimisation of antibiotic use and provides a basis for addressing misuse through hospital authorities. Monitoring factors that predict prolonged hospital stays and in-hospital mortality is crucial for enhancing patient outcomes and minimising the financial costs of hospitalisation. The findings could help inform future research and guide hospital policy on antibiotic use, similar to studies conducted in Spain.[21]
This study has a few limitations, including its single-centre design and the brief two-month duration. The lack of a control group and reliance on empirical antibiotic therapy without comprehensive molecular data limits insights into resistance mechanisms. The study focused solely on in-hospital outcomes, excluding long-term impacts or post-discharge morbidity. While prolonged antibiotic use and hospital stays were associated with higher costs, a detailed cost analysis was not performed.
Conclusion
Our study demonstrated that the use of empirical antibiotic therapy for systemic bacterial infections was generally appropriate, guided by local endemic patterns of infectious agents. However, instances of antibiotic misuse were identified, highlighting the need for increased vigilance and oversight by healthcare authorities to prevent the escalation of AMR. This research also provided valuable insights into the most prevalent infections in the study locality, addressing a significant gap in knowledge, as no prior studies had been conducted in comparable settings. Key takeaways from this study include the high prevalence of pneumonia, the dominant use of piperacillin–tazobactam combinations, and the association of prolonged antibiotic use and immunocompromised status with poorer hospital outcomes. These findings underscore the urgent need for strengthened antimicrobial stewardship programs, context-specific clinical guidelines and ongoing surveillance of antibiotic usage patterns. Policymakers should prioritise investments in hospital-based antibiotic stewardship initiatives and establish routine audits to ensure rational prescribing practices.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the Indian Council of Medical Research (ICMR) for supporting this study under the short-term studentship (ICMR STS) program. Special thanks to Squad Medicine and Research (SMR) for their guidance and help in publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval was taken from Institutional Ethical Committee (IEC) of Burdwan Medical College, West Bengal, India (BMC/IEC/420).
Informed consent
Informed consent was obtained from the patient for the research and the publication.
Credit author statement
Patra S was involved in idea, conceptualisation, data collection, writing draft and approved final draft.
Biswas U helped in idea, conceptualisation, supervision, formal analysis, methodology, writing draft and approved final draft.
Muppavarapu RS contributed to formal analysis, writing draft and revision of draft and approved final draft.
Killi K helped in formal analysis, writing draft and revision of draft and approved final draft.
Suvvari TK was involved in supervision, project administration, resources, formal analysis, writing draft and revision of draft and approved final draft.
Data availability
The data of this project is available and can be provided on request.
Use of artificial intelligence
No AI/AI tools were used while working on this manuscript.