
Abstract
Objective:
This prospective, randomised comparative study assessed the volumetric and dosimetric impact of dual adaptive radiotherapy (ART) versus single ART on parotid glands in head and neck cancer patients.
Materials and Methods:
Eighty patients were enrolled, with 40 in each arm. Targets and organs at risk (OARs), including ipsilateral (iParotid) and contralateral parotid glands (cParotid), were delineated on planning scans. The control arm received a single adaptive plan at the 25th fraction (APLAN 25), while the study arm underwent dual adaptive replanning at the 15th and 25th fractions (APLAN 15/25). A non-adaptive plan (DPLAN 25) was generated to estimate the dose delivered to OARs if the primary plan had been executed without adaptation. Volumetric and dosimetric analyses were performed.
Results:
Significant parotid shrinkage was observed, with approximately 65.92% of the volume loss occurring within the first 15 fractions. Dual ART achieved a statistically significant reduction in dose to the iParotid (6.07%) and cParotid (4.3%) compared to single ART.
Conclusion:
Dual ART in the 3rd and 5th week of radiation significantly reduced parotid doses compared to single ART in the 5th week.
Introduction
Radiotherapy plays a crucial role in the treatment of head and neck malignancies, contributing significantly to organ preservation. The growing emphasis on preserving organs has established radiotherapy as an indispensable treatment modality for these cancers.[1] Among many survivors of head and neck cancer, the prevailing enduring consequence of radiation therapy (RT) is Xerostomia, known as dry mouth syndrome. Damage to the salivary glands caused by radiation results in alterations to the volume, consistency, and pH of secreted saliva. The transformation involves a shift from thin secretions with a neutral pH to thick and tenacious secretions characterised by heightened acidity. Individuals undergoing such changes often experience oral discomfort or pain, encounter difficulties in speaking, chewing, and swallowing, and face an elevated risk of dental caries or oral infections. Consequently, these challenges may lead to a decline in nutritional intake and subsequent weight loss. Xerostomia not only significantly diminishes the quality of life (QoL) for numerous patients who may potentially be cured from their cancer but also presents a substantial new health concern for them.[2] Deformations in the targets, normal structures, and patient anatomy may manifest over the duration of a six to seven-week radiotherapy regimen. Studies have demonstrated that the parotid gland experiences alterations in both volume and dose throughout the course of radiotherapy.
Salivary gland function remains largely preserved when the mean radiation dose is below 10–15 Gy. As the dose increases to the range of 20–40 Gy, a progressive decline in glandular function is observed, with significant impairment—typically exceeding 75% reduction—occurring at doses above 40 Gy. Although functional recovery may occur over time with doses up to 40–50 Gy, exposure to higher doses generally results in irreversible glandular hypofunction and persistent xerostomia.[3,4] The risk of developing severe xerostomia—characterised by long-term salivary output falling below 25% of baseline—can be significantly reduced if at least one parotid gland receives a mean radiation dose of <20 Gy, or if both parotid glands are limited to mean doses <26 Gy. In scenarios involving complex partial volume irradiation techniques such as intensity-modulated radiotherapy (IMRT), it is advisable to minimise the mean dose to each parotid gland as much as feasible, while maintaining adequate clinical target volume coverage. Improved salivary function is generally associated with lower mean parotid doses, including in cases where doses are kept below 10 Gy.[3] Comprising acinar cells, the parotid gland undergoes apoptosis of these cells during the radiotherapy process, leading to considerable changes in its volume. Additionally, a discernible medial shift of the organ has been identified. Consequently, the mean dose administered to the parotid tends to exceed the calculated values based on the treatment planning CT.[5,6]
Adaptive radiation therapy (ART) is a concept that enables clinicians to reassess the planned dosage, considering any potential alterations, to precisely administer the remaining radiation dose to the tumour while effectively reducing radiation exposure to surrounding healthy tissues. Given the considerable amount of literature suggesting a correlation between volume alterations and the dosimetric impact on both tumour and parotids, we aimed to investigate this relationship prospectively. Additionally, we sought to determine the optimal timeframe during which these changes are significant enough to warrant a modification in the treatment plan in order to decrease the mean dose to parotids, keeping in mind the target coverage as well. Head and neck malignancies offer an ideal setting for such adaptive analysis due to their high prevalence, the proximity of critical structures and the established benefits of intensity-modulated radiation therapy (IMRT) in managing these malignancies. Therefore, we initiated this prospective study focusing on ART in head and neck cancers to determine the changes in mean dose received by the parotids and thereby causing a reduction in the risk of xerostomia
Materials and Methods
Study Design and Duration
This prospective randomised comparative study was conducted at the Department of Radiation Oncology, Apollo Specialty Hospital, Teynampet, Chennai, from June 2022 to December 2023.
Study Sample
Inclusion Criteria: Patients with head and neck carcinoma (squamous cell carcinoma), aged 18–70 years, Karnofsky performance status >70, receiving concurrent Cisplatin, undergoing definitive radiotherapy with bilateral cervical nodal irradiation, and opting for high-precision techniques (IMRT, IGRT, Rapid Arc).
Exclusion Criteria: Prior head and neck radiotherapy, parotid tumours, unilateral irradiation, documented salivary gland dysfunction, CTV involvement of the parotid, prior resection or induction chemotherapy, recurrent cancer.
Radiotherapy Preparation
Patients were immobilised using a 5-point thermoplastic mask on a flat couch. A contrast planning CT scan (CTplan) was obtained with 3 mm slice thickness from the base of the skull to the superior mediastinum. The CT images were transferred to the Eclipse Treatment Planning System (Version 13). Patients were randomised into the control arm (1 adaptive re-planning at 25 fractions) and the study arm (2 adaptive re-plannings at 15 and 25 fractions).
Contouring
Gross Tumour Volume (GTV) included the primary tumour and clinically involved nodes.
Clinical Target Volume (CTV) included suspected subclinical disease and regional lymphatics.
Planning Target Volume (PTV): Expanded GTV by 3 mm (high-risk) and CTV by 3 mm (intermediate-risk).
Organs at Risk (OAR) such as parotids, spinal cord, mandible, and lungs were contoured.
Radiotherapy Planning
A dose of 66 Gy in 2 Gy/fraction was prescribed to the PTV (High risk), and 59.4 Gy in 1.8 Gy/fraction to the PTV (Intermediate risk). A mean dose constraint of <26 Gy was applied to each parotid gland. Treatment planning was conducted in the Eclipse system by Varian. Plans were assessed through visual examination of isodose lines and dose-volume histograms. Accepted plans were labelled as OPLAN 25 (original initial plan in control arm) and OPLAN 15/25 (original plan in study arm). All patients received concurrent weekly Cisplatin (40 mg/m²).
Adaptive Re-planning
Control Arm: A follow-up CT at 25 fractions (CT25) was registered with the planning CT images.
Study Arm: Follow-up CTs were performed at 15 fractions (CT15) and 25 fractions (CT25). CT15 was registered with the planning CT, and CT25 with CT15.
Volumetric Analysis
Structures were modified in CT25 (control arm) and CT15 & CT25 (study arm) based on changes in body and tumour volumes. The GTV volume remained unchanged. Volumetric changes in ipsilateral (iParotid) and contralateral (cParotid) parotids were measured. Modifications were performed by the same physician
Dosimetric Analysis
Control Arm: The OPLAN 25 was applied to the follow-up CT scan obtained after 25 fractions (CT25). The isocenter was realigned to match the original plan, and calculations were rerun to determine the doses for the ipsilateral (iParotid) and contralateral (cParotid) parotid glands if the initial plan were executed over the updated volume. This resulted in a non-adaptive plan, termed DPLAN 25. Subsequently, a single adaptive re-planning (APLAN 25) was performed using the CT25 images with modified structures. The mean doses (Dmean) for iParotid, cParotid, and bilateral parotids after this single adaptive re-planning were then measured and compared.
Study Arm: The OPLAN 15/25 was first applied to the CT scan obtained after 15 fractions (CT15). The CT15 images, along with modified structures, were used for the first adaptive re-planning, covering the subsequent 10 fractions of treatment. Following this, the plan from CT15 was adapted to CT25, incorporating further modifications. The CT25 images, now updated, were used for the second adaptive re-planning, which addressed the remaining 8 fractions. This double adaptive plan was designated as APLAN 15/25. Mean doses for iParotid, cParotid, and bilateral parotids after both adaptive replannings were then assessed and compared to those in the control arm.
The calculated sample size was 80, with a minimum of 40 participants in each group. Participants were randomly assigned to the control or study arm using a lottery method, with 40 slips for each group. Each participant drew a slip to determine their assignment.
Statistical Analysis
Descriptive statistics included frequency (percentage) and mean ± SD for categorical and continuous factors, respectively. Chi-square/Fisher’s exact test assessed associations between categorical factors. Paired t-test/Wilcoxon signed-rank test evaluated paired observations. Repeated Measures ANOVA/Friedman test assessed changes in paired observations. One-way ANOVA/Kruskal-Wallis test analysed Dmean variations. Student’s t-test/Mann-Whitney U test compared the study and control arms. A P < .05 was considered significant. Statistical analysis was performed using SPSS (IBM, 28.0).
Results
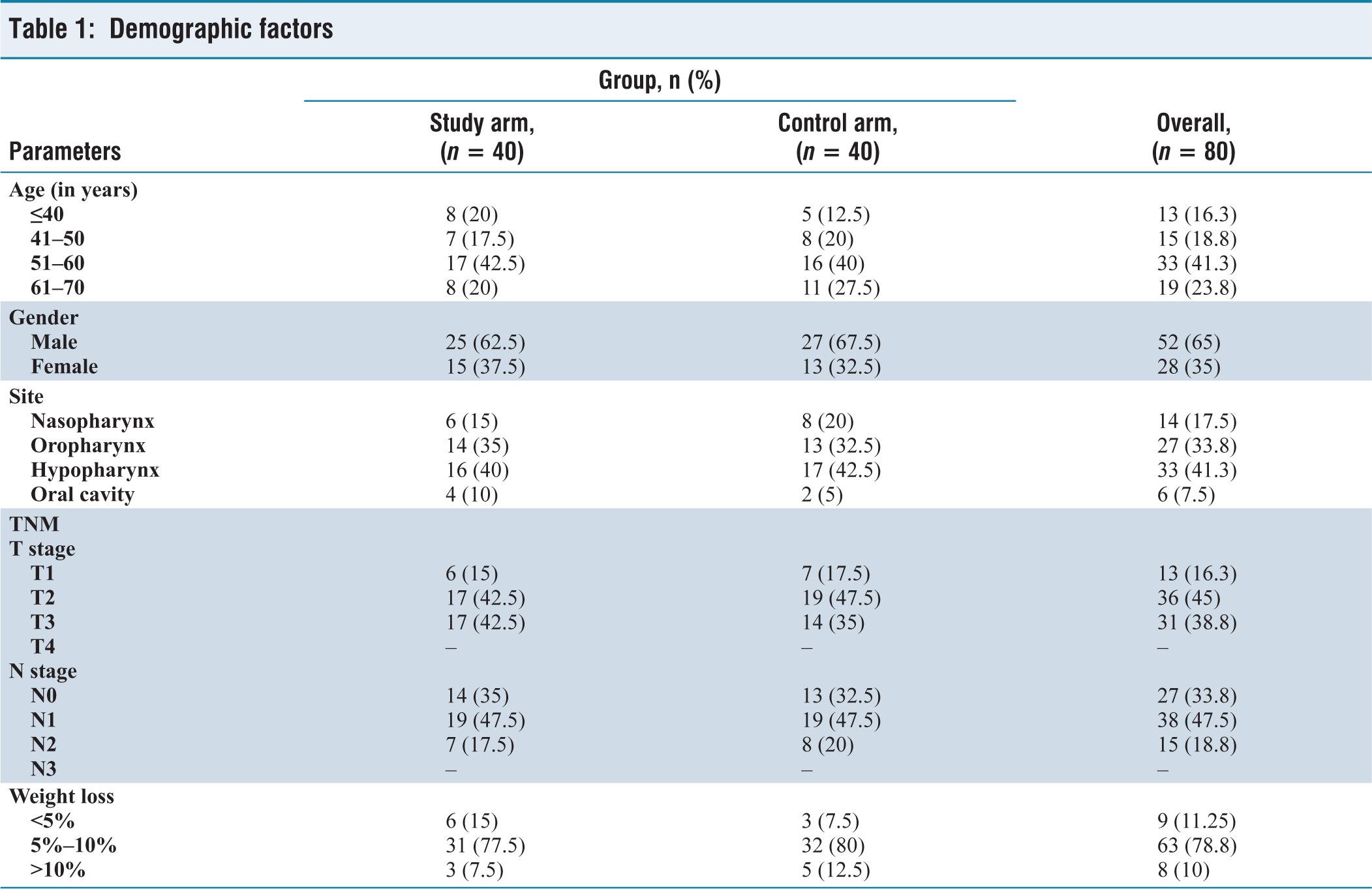
Eighty patients fulfilling the inclusion criteria were analysed for dosimetric and volumetric changes, with each arm having 40 patients each. Patient characteristics are summarised in Table 1.
Demographic factors
Volumetric Analysis in Dual ART Arm
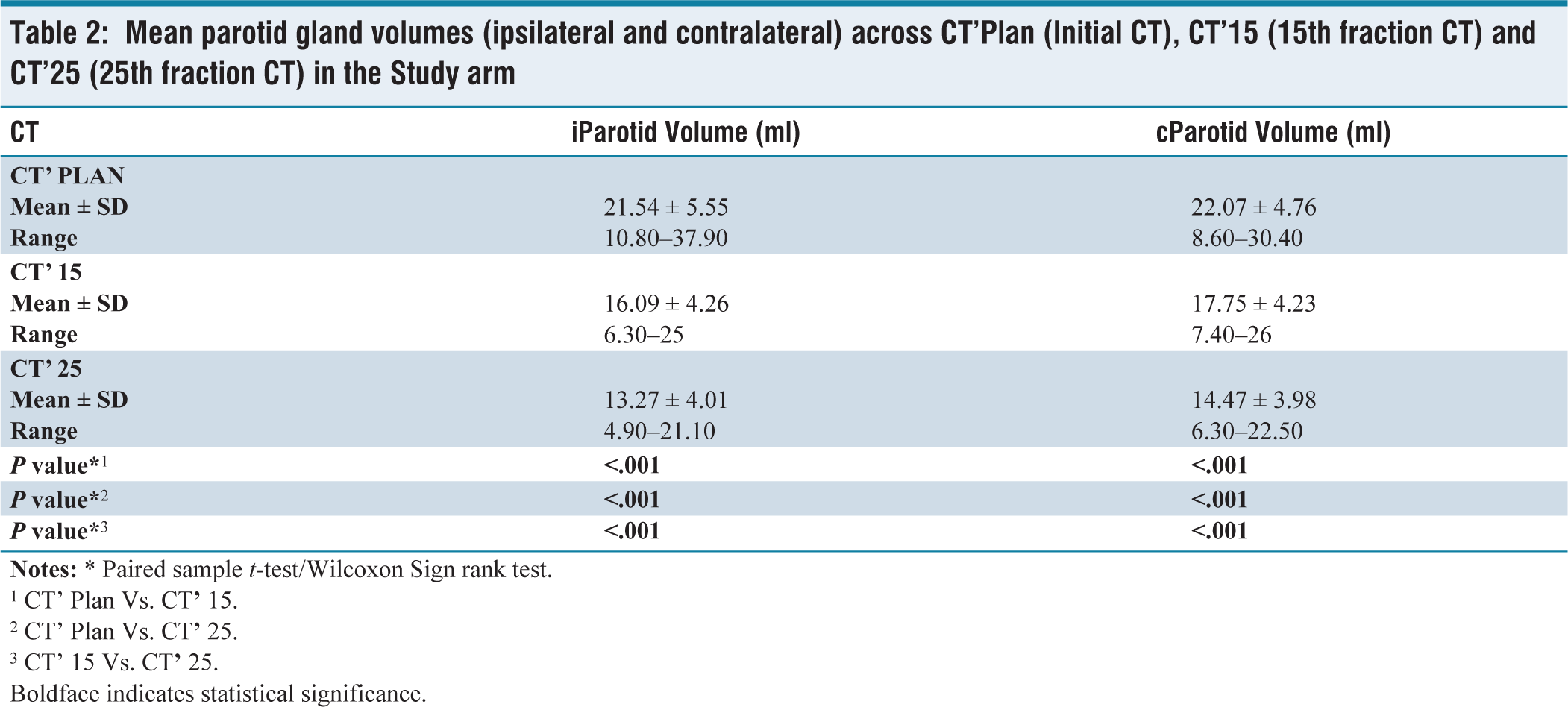
In the initial CT (CT’PLAN), the mean iParotid and cParotid volumes were 21.54 ml (±5.55) and 22.07 ml (±4.76), respectively. After 15 fractions of radiotherapy (CT’15), the iParotid volume decreased by 25.32% (5.45 ml) and the cParotid by 19.10% (4.32 ml). By 25 fractions (CT’25), the iParotid and cParotid volumes further decreased by 17.53% (2.82 ml) and 18.56% (3.28 ml), respectively. Overall, iParotid volume reduced by 8.26 ml, with 65.92% of this loss occurring in the first 15 fractions. Similarly, the cParotid lost 7.59 ml, with 56.9% occurring in the first 15 fractions. The values were all statistically significant (P < .05). These reductions were statistically significant (P < .05). This suggests that a significant portion of the volume reduction in the parotid glands occurs early in the RT process [Table 2].
Mean parotid gland volumes (ipsilateral and contralateral) across CT’Plan (Initial CT), CT’15 (15th fraction CT) and CT’25 (25th fraction CT) in the Study arm
1 CT’ Plan Vs. CT
2 CT’ Plan Vs. CT
3 CT’ 15 Vs. CT
Boldface indicates statistical significance.
Dosimetric Analysis in Single ART Arm
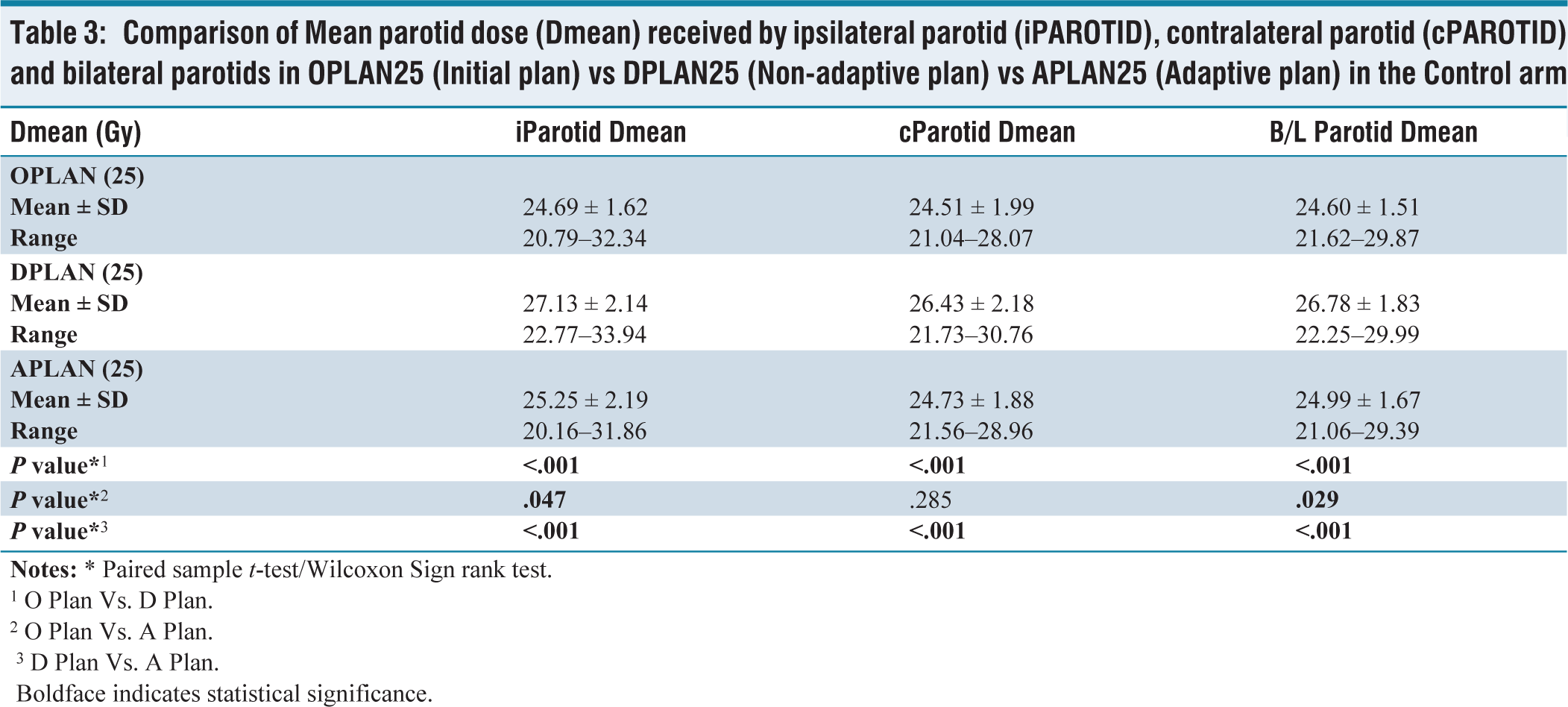
The initial radiotherapy plan (OPLAN 25) delivered mean doses of 24.69 Gy to the iParotid and 24.51 Gy to the cParotid. In contrast, the non-adaptive plan (DPLAN 25) resulted in significantly elevated doses, with 27.13 Gy (9.88% increase) to the iParotid and 26.43 Gy (7.83% increase) to the cParotid as shown in Table 3. The adaptive plan (APLAN 25), designed after 25 fractions, reduced the mean doses to 25.25 Gy for the iParotid and 24.73 Gy for the cParotid. A single adaptive plan (APLAN 25) implemented after 25 fractions significantly reduced mean dose exposure compared to DPLAN 25, providing relative reductions of 7.62% (iParotid), 6.94% (cParotid), and 7.28% for the bilateral parotids. The values were all statistically significant (P < .05).
Comparison of Mean parotid dose (Dmean) received by ipsilateral parotid (iPAROTID), contralateral parotid (cPAROTID) and bilateral parotids in OPLAN25 (Initial plan) vs DPLAN25 (Non-adaptive plan) vs APLAN25 (Adaptive plan) in the Control arm
1 O Plan Vs. D Plan.
2 O Plan Vs. A Plan.
3 D Plan Vs. A Plan.
Boldface indicates statistical significance.
Dosimetric Analysis in Dual ART Arm
OPLAN (15/25) delivered mean doses of 24.36 Gy to the iParotid and 23.73 Gy to the cParotid. APLAN (15/25) significantly reduced these doses to 23.43 Gy (3.82% reduction) for the iParotid and 22.92 Gy (3.41% reduction) for the cParotid. Statistically significant differences in mean doses were observed between OPLAN and APLAN for both parotid glands (P < .05).
Dosimetric Comparison Between Dual Adaptive (Oplan 15/25) Versus Single Adaptive (Oplan 25) Versus Non-adaptive (Dplan 25) Plans
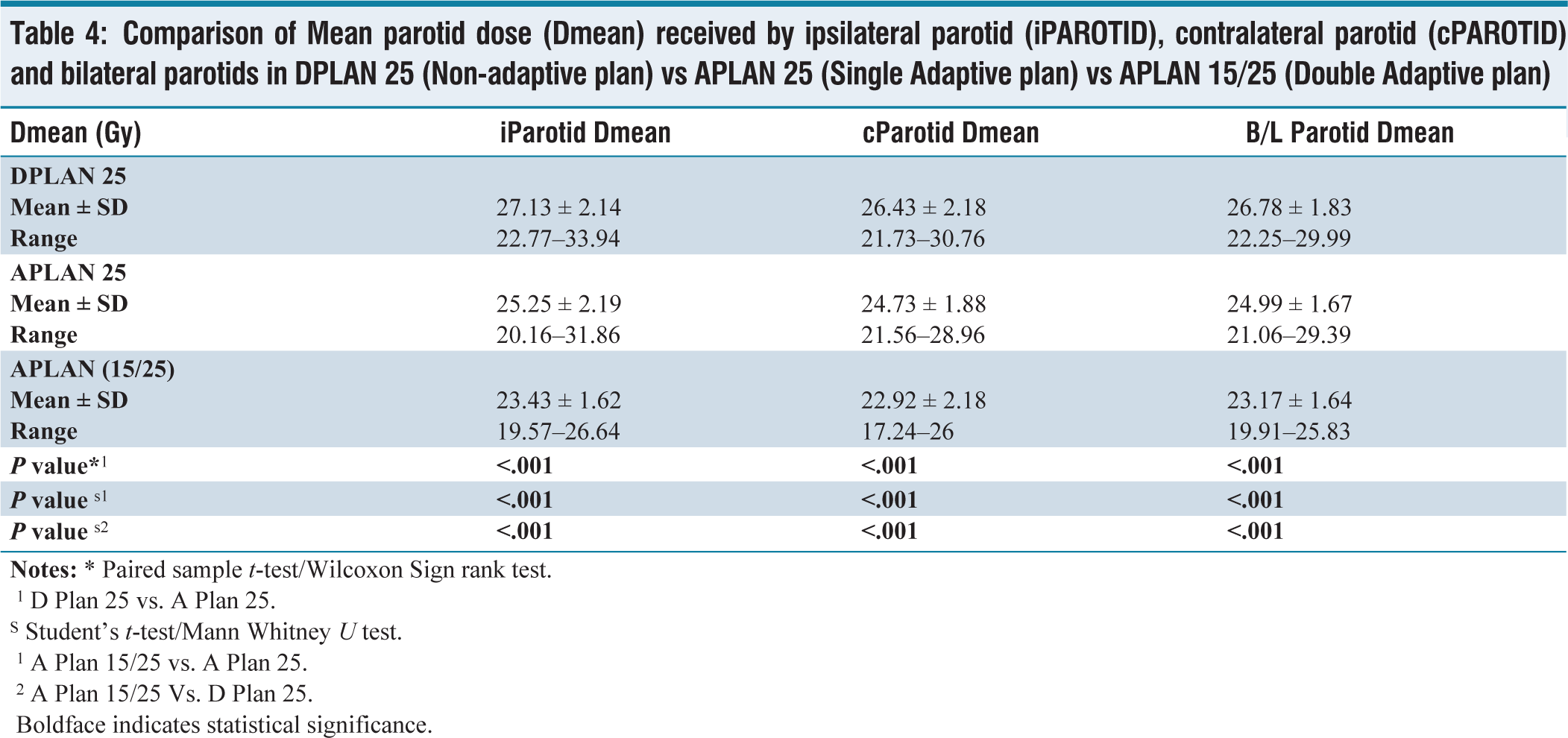
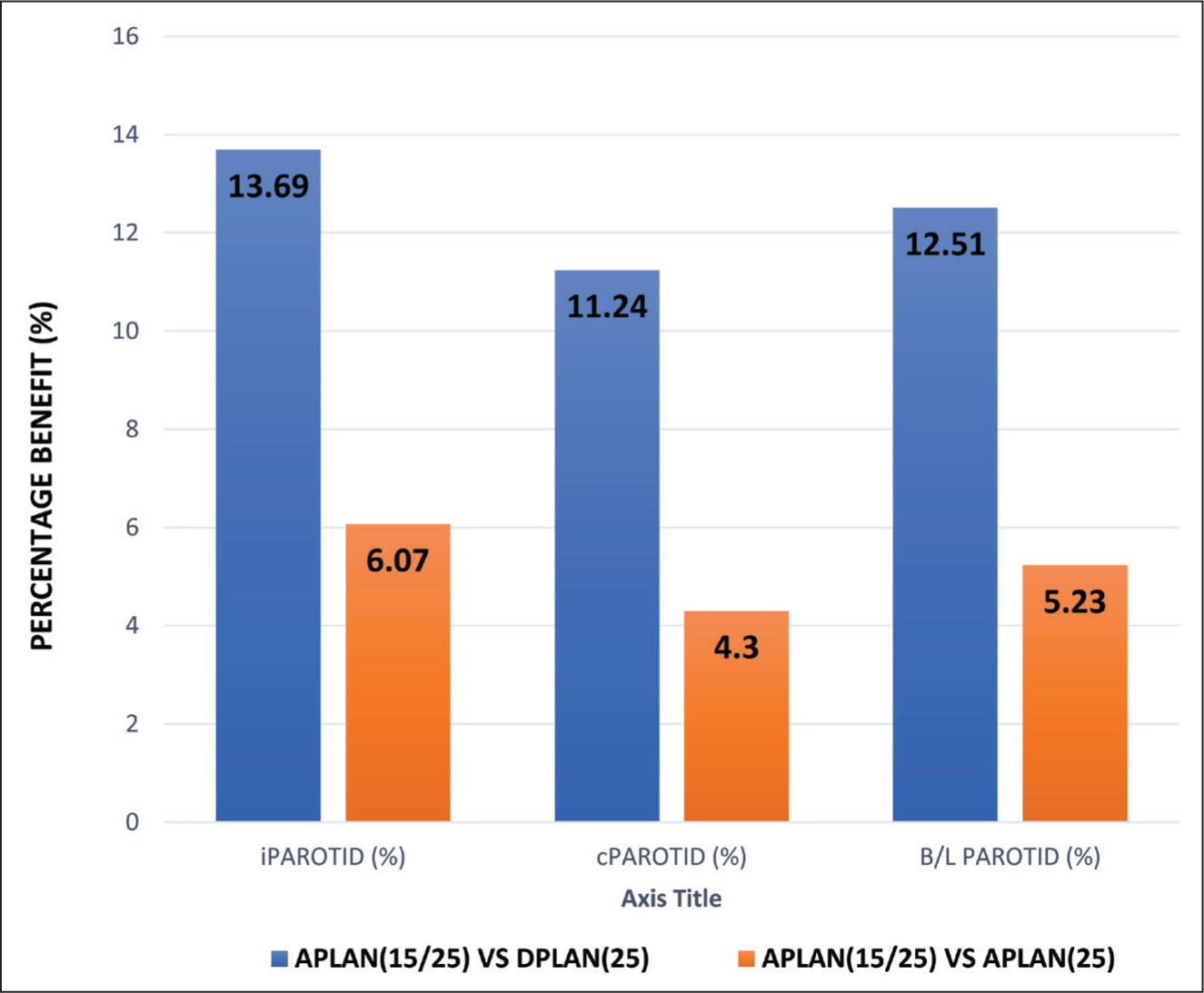
Double ART (APLAN 15/25) offers significant reductions in mean parotid doses compared to both non-adaptive (DPLAN 25) and single adaptive RT (APLAN 25), as shown in Table 4 and Figure 1. For the ipsilateral parotid, APLAN 15/25 reduced the Dmean by 13.69% compared to DPLAN 25 and by 6.07% compared to APLAN 25. Similarly, the contralateral parotid showed reductions of 11.24% versus DPLAN 25 and 4.3% versus APLAN 25. Bilateral parotids demonstrated a 12.51% and 5.23% reduction compared to DPLAN 25 and APLAN 25, respectively. These findings underscore the superior efficacy of double adaptive RT in reducing radiation exposure.
Comparison of Mean parotid dose (Dmean) received by ipsilateral parotid (iPAROTID), contralateral parotid (cPAROTID) and bilateral parotids in DPLAN 25 (Non-adaptive plan) vs APLAN 25 (Single Adaptive plan) vs APLAN 15/25 (Double Adaptive plan)
1 D Plan 25 vs. A Plan 25.
S Student’s t-test/Mann Whitney U test.
1 A Plan 15/25 vs. A Plan 25.
2 A Plan 15/25 Vs. D Plan 25.
Boldface indicates statistical significance.
Comparison of Relative Percentage advantage in Parotid mean dose reduction by double adaptive RT (APLAN 15/25) VS DPLAN 25 (Non-adaptive RT) and APLAN 25 (Single Adaptive RT)
Discussion
A significant challenge encountered in irradiating head-and-neck cancer arises from the proximity of critical organs to the target area, especially the salivary glands. Consequently, patients experience a significant decline in their quality of life as a result of these treatment-related complications.[7] The utilisation of contemporary irradiation techniques, such as IMRT or Volumetric Modulated Arc Therapy (VMAT), necessitates comprehensive patient assessment from multiple dimensions. This includes meticulous imaging evaluation preceding each dose fraction, as well as meticulous verification of proper patient immobilisation. Moreover, it is imperative to monitor any fluctuations in patient weight and ensure the appropriate fit of immobilisation masks to optimise treatment accuracy and efficacy.[8] The phenomenon of parotid gland volume reduction and positional displacement during RT is potentially linked to various factors, including reductions in tumour and nodal volumes, patient weight loss, alterations in muscle mass, shifts in fat distribution, and changes in bodily fluid dynamics. Additionally, studies have indicated that medial migration of the parotids toward regions of high radiation dose during the course of radiotherapy contributes to organ shrinkage.[8] Schwartz et al. demonstrated in their study that implementing ART for oropharyngeal squamous cell carcinoma allows for significant dosimetric enhancements, with the majority of these improvements achievable through one or two replanning sessions conducted during the midpoint of treatment.[9]
Changes in Parotid Volumes
The volume changes that occur during the course of radiotherapy can be quantified by serial CT scans. In our study, the parotid glands underwent reduction in their volume, which has been quantified as 25.3% & 19.5% in the ipsilateral and contralateral parotids at the end of 15 fractions respectively and 38.3% and 34.3% in the ipsilateral and contralateral parotids at the end of 25 fractions respectively which was statistically significant. Table 5 shows a comparison of parotid volume change with previous studies. They are in concordance with our study. Upon analysing these variations, our study, in line with several others in the literature, has identified statistically significant changes occurring post-15 fractions. Notably, findings from Bhide et al. indicate significant changes as early as the 2nd week based on weekly analyses, corroborating similar conclusions drawn by Beltran et al. and Bhandari et al. Furthermore, Schwartz et al. proposed that significant changes manifest during the 3rd and 4th weeks of radiotherapy.[10] The observed phenomenon can be attributed to the heightened sensitivity of acinar cells to radiotherapy during the initial weeks, followed by a relative resilience of less sensitive cells, resulting in minor volume fluctuations thereafter. Considering the substantial adipose content within normal parotid glands, the observed shrinkage correlates understandably with treatment-induced weight loss.[11]
Comparison of parotid volume change of our study with previous studies

Changes in Mean Parotid Dose
Changes in the volume of the GTV, CTV and PTV lead to increased plan inhomogeneity and decreased conformity. As radiation progresses, the volume of parotid glands diminishes. Coupled with the expansion of the prescription isodose line to cover more volume than initially planned, this results in an elevation of the mean parotid dose compared to the initially planned dose. In our study, DPLAN 25 (non adaptive RT), on comparison with OPLAN 25 (Original initial plan) exhibited elevated mean doses received by parotid glands, by 2.44 Gy (9.88%) for iParotid and 1.92 Gy (7.83%) for cParotid which was statistically significant.
Single Adaptive RT plan, APLAN 25 showed slightly elevated mean doses received by parotids compared to OPLAN 25 by 0.56 Gy (2.26%) for iParotid and 0.22 Gy (0.89%) for cParotid, which was statistically significant. There is a notable decrease in mean parotid doses with the implementation of Adaptive plans compared to the non-adaptive plan. The study by Franzese et al.[12] showed comparative results with our study, as shown in Table 6.
Comparison of difference in parotid mean dose in DPLAN and APLAN with initial plan, of our study with previous study

In our study, 2 ART sessions - APLAN 15/25 resulted in a 3.81% decrease in mean parotid dose for the ipsilateral parotid gland (iParotid) and a significant 3.41% reduction for the contralateral parotid gland (cParotid), which was statistically significant. Wu et al.[13] conducted a study revealing that implementing two replanning sessions during the course of head and neck radiotherapy resulted in a 5% improvement in parotid mean dose sparing. This is in concordance with our study.
Avgousti et al. recommended that the optimal timing for adaptive replanning typically falls between the third and fourth week of radiotherapy. Replanning was prompted when specific thresholds were exceeded, including anatomical deviations greater than 1 cm in the external body contour, average weight loss exceeding 10%, a reduction in target dose coverage by more than 5%, or significant deviations in the dose delivered to surrounding normal tissues.[14] Castelli et al. identified nodal disease stage, the size of the largest involved lymph node at baseline, diagnosis, and initial body weight as significant factors for inclusion in predictive models and risk stratification profiles for ART.[15] In a study by Yao WR et al. specific criteria were proposed to guide the timing of ART for parotid gland preservation. The criteria included three parameters: (a) an initial parotid volume exceeding 52.80 cm³; (b) an initial mean parotid dose greater than 32.04 Gy; and (c) a weight loss rate of more than 2.3% by the 11th fraction, more than 3.6% by the 16th fraction, or more than 4.4% by the 21st fraction. If a patient met any two of these three criteria, there was a high likelihood of parotid overdose, and replanning was advised at that treatment fraction. These criteria effectively integrate volumetric and dosimetric changes with patient-specific characteristics and can be assessed without the need for repeated CT imaging during the course of radiotherapy.[16]
Comparison of relative percentage advantage in parotid Dmean reduction by double ART (APLAN 15/25) versus single ART (APLAN 25) showed benefit of 6.07% in ipsilateral parotid (iPAROTID) and 4.3% in contralateral parotid (cPAROTID), Schwartz et al.[9] observed that by dual adaptive planning, a reduction in mean parotid gland (PG) dose by 3.8% for contralateral PGs and by 9% for ipsilateral PGs was achieved. He demonstrated in their research that for patients requiring dual adaptive plans, the median trigger for the first replan was observed at the 11th fraction, while the second replan was typically triggered around the 22nd fraction. In our study approximately 65.92% of the total volume loss occurred during the first 15 sittings of radiation, indicating that the major loss in volumes indeed occurs during the first three weeks of radiation treatment. Hence re-planning at this juncture could enhance critical structure preservation and potentially mitigate long-term toxicities.
Conclusion
Head and neck malignancies present an optimal scenario for ART, given their high prevalence, the close proximity of vital structures, and the established advantages of IMRT in treating these malignancies. Our study demonstrated a significant reduction in mean parotid doses with the use of adaptive plans compared to non-adaptive plans. Dual ART (done at the 3rd and 5th week) compared to single ART (done at the 5th week) showed a statistically significant dose benefit of 6.07% in the ipsilateral parotid and 4.3% in the contralateral parotid.
Several unresolved issues persist with ART, including the individualised prediction and localisation of disease and normal tissue targets for mid-treatment dose adjustment using functional imaging. Additionally, there is a need to determine the feasibility and necessity of developing fully automated, online dosimetric evaluation, replanning, and treatment modification systems. Furthermore, patient selection criteria based on the greatest need for ART are essential to optimise cost-effectiveness.[9] The utilisation of models to identify patients who would benefit most from replanning may aid in the optimal utilisation of ART techniques.[10]
Footnotes
Acknowledgements
First and foremost, I would like to thank my co-authors, Dr. Sanjay Chandrasekhar and Dr. Mahadev Potharaju, for their expert guidance and invaluable insights throughout the course of this research. Their mentorship and constructive feedback were pivotal in refining the methodology and overall direction of the study. A special thanks to my wife and co-author, Dr. Nimmy Varghese, for her unwavering support, both personally and professionally. Her assistance with data management and her dedication to helping me stay organised was critical in completing this project. Lastly, I am grateful to the language and editorial team for their help with proofreading and refining the manuscript, ensuring that the final version was polished and ready for publication. As the corresponding author, I am deeply appreciative of all the collaborative efforts that have made this work possible.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The research/study was approved by the Institutional Review Board at Apollo Hospital AHEL, Chennai, number ASH-DNB-025/06-22, dated 21.06.2022.
Informed consent
The authors certify that they have obtained all appropriate patient consent.
Credit author statement
Dr Rakesh Bastin: Data collection and compilation of the article.
Dr Nimmy Varghese: Data collection.
Dr Sanjay Chandrasekhar: Expert insights and guidance.
Dr Mahadev Potharju: Expert guidance.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article.
Use of artificial intelligence
None.