
Abstract
Background:
Abdominal pain is one of the most common complaints of patients presenting to the gastroenterology outpatient department (OPD). Despite exhaustive evaluation, the cause of pain often remains elusive. This study was performed to assess the use of endoscopic ultrasound (EUS) examination in ascertaining the aetiology of upper abdominal pain and its impact on therapeutic decision making.
Method:
Fifty patients (19 male and 31 female) with chronic pain abdomen who were previously undiagnosed and had undergone biochemical and cross sectional imaging (either Contrast enhanced computed tomography of abdomen on Magnetic resonance imaging of abdomen) were included in the study. All underwent EUS using a linear and radial scope under general anaesthesia (GA).
Results:
EUS could reach a diagnosis in 24 (48%) patients. EUS diagnoses were as follows: gallbladder (GB) stones/sludge in 10 (20%) and common bile duct (CBD) stones/sludge in 9 patients (18%), CBD stricture in 2 (4%) and chronic pancreatitis in 3 patients (6%). Out of the 24 patients who were diagnosed on the basis of EUS, 19 underwent therapeutic procedures (endoscopic retrograde cholangiopancreatography (ERCP)/surgery) and 16 (84.21%) amongst them were pain free at six months follow-up.
Conclusion:
EUS could successfully diagnose the cause of pain in 48% of patients and this resulted in therapeutic interventions (medical, endoscopic or surgical) in 40% of them. Hence, it could significantly alter the management in a large number of patients resulting in pain relief.
Introduction
Chronic abdominal pain (CAP) is one of the most common complaints in the gastroenterology outpatient department (OPD).[1] Its diagnosis can be a challenging problem for the clinician. The standard workup for the investigation of CAP includes biochemical tests like liver function test (LFT), serum amylase and lipase which are followed by simple imaging tests like ultrasound, followed by endoscopy and if this does not result in a diagnosis, then more specialised tests like computed tomography (CT), magnetic resonance imaging (MRI) or positron emission tomography (PET) scan. Despite the number of available investigations, 35% of patients remain undiagnosed even after an extensive workup.[2]
Endoscopic ultrasound (EUS) has changed the management of abdominal pain completely. It has become the gold standard for the diagnosis of gallbladder (GB) microlithiasis, common bile duct (CBD) stones and chronic pancreatitis.[3,4] However, its positioning in the management algorithm of abdominal pain is still not clear given its high cost and the need for anaesthesia. This study was performed to assess the role of EUS in patients of CAP and to suggest an algorithm for their management.
Methods
Inclusion Criteria
Consecutive patients of CAP attending the gastroenterology OPD between December 2019 and July 2021 were included in the study. The inclusion criteria were as follows:
Patients with pain upper abdomen lasting greater than six months with no identified cause despite biochemical investigations, upper gastrointestinal (GI) endoscopy, transabdominal ultrasonography abdominal CT, MRI, magnetic resonance cholangiopancreatography (MRCP) or PET scan.
Exclusion Criteria
Patients with pre-existing hepatobiliary-pancreatic disorders
Patients with known psychiatric disorders
Ongoing GI bleed
Patients aged less than 18 years
All patients included in the study underwent baseline haematological and biochemical evaluation (complete blood count (CBC), LFT, kidney function test (KFT), amylase and lipase) and transabdominal ultrasound and either contrast-enhanced computed tomography (CECT) or MRI and MRCP. Thereafter, they underwent EUS which was performed with Olympus Linear and Radial echo endoscope Olympus EVIS EXERA III CLV-190 processor. The procedure was done under short-acting general anaesthesia (Propofol). The procedure was performed as an outpatient procedure and all patients were observed for two hours prior to discharge.
All patients underwent an assessment of pain on a visual analogue scale prior to inclusion and were reassessed two weeks and six months after any intervention arising out of EUS findings either in the OPD or as a telephonic interview. A reduction in pain to a level less than or equal to 2 OR a reduction in pain by 50% in the first two weeks after the procedure was taken as a positive response.
Results
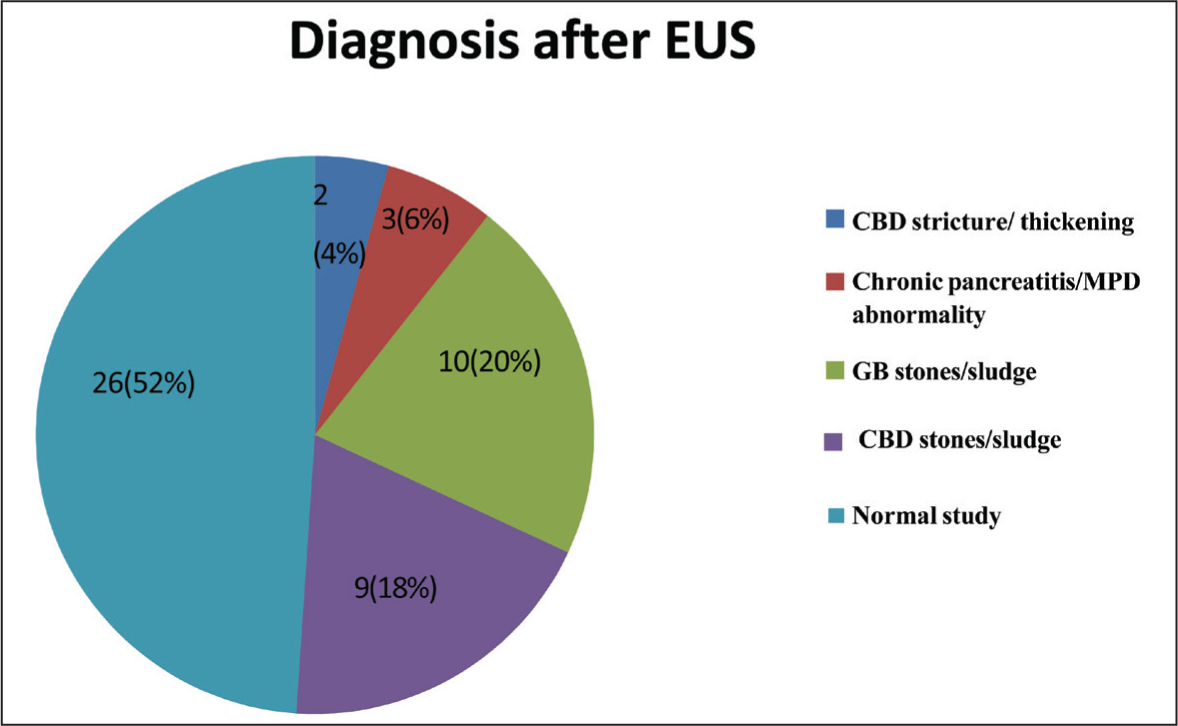
A total of 50 patients (19 males and 31 females) were included in the study. The mean age of patients was 44.2 years. Age of presentation was higher in females (50 years) than males (38 years). Among these patients, a majority (72%) of patients had pain lasting for more than one year. Of the 50 patients presenting with pain, 32(64%) had mild pain, 15(30%) had moderate pain and 3(6%) reported severe pain. Serum amylase and serum lipase were deranged in 3 (6%), whereas deranged liver function tests were present in 12(24%) patients. After completion of EUS examination, a diagnosis could be reached in 24(48%) of the total patients enrolled. These included GB stones/sludge in 10 (20%) and CBD stones/sludge in 9 patients (18%), CBD stricture in 2 (4%) patients and chronic pancreatitis in 3 patients (6%) [Figure 1].
Pie chart depicting the various causes of chronic abdominal pain
Of the 10 patients diagnosed to have gallstones, 8 agreed to undergo a cholecystectomy and 6 (75%) had relief of pain two weeks following surgery, and 2 patients continued to report pain but of lesser intensity. All 9 patients with CBD stones underwent ERCP successfully. Eight of nine (88%) patients reported relief of pain two weeks later. Of the two patients of CBD stricture, one underwent ERCP and had pain relief. Of the three patients diagnosed to have chronic pancreatitis, one had dilated main pancreatic duct (MPD) and underwent a pancreatic stenting and had relief of pain [Table 1]. Three patients reported abdominal pain and distention following EUS. No major complication was reported.
Analyses of pain relief following interventions

EUS could diagnose the cause of pain in 24/50 (48%) of patients of these pain could resolve in 16/50 (32%). There were no complications reported following diagnostic EUS.
Discussion
Patients with undiagnosed CAP tend to have repeated hospital visits and a large percentage remains undiagnosed despite repeated hospital visits and multiple high-end investigations like CT abdomen and MRI. EUS is a relatively new therapeutic modality which has very rapidly replaced MR and CT as the gold standard for a number of conditions like chronic pancreatitis, CBD stones and GB microlithiasis. Early use of EUS in the diagnostic protocol of pain abdomen is likely to result in saving in both time and cost for these patients.[5]
In our study, EUS could successfully diagnose the cause of pain in 48% of our patients. And this resulted in therapeutic interventions (medical, endoscopic or surgical) in 40% of patients. Hence, it could significantly alter the management in a large number of patients resulting in pain relief.
It is well known now the EUS has a significantly higher sensitivity and specificity than cross-sectional imaging like CT or MR in detecting CBD stones (especially those less than 0.5 mm) GB microlithiasis and chronic pancreatitis.[6] All three are major causes of upper abdominal pain of obscure origin. Another advantage of EUS is that it can sample lesions (lymph nodes, masses) in the same session obviating the need for another procedure.[7]
Conclusion
Based on our study, we would suggest the final step-wise protocol for the management of CAP of unknown origin:
Biochemical investigations and ultrasound whole abdomen Upper GI endoscopy and colonoscopy as required by the clinical assessment CECT or MRI abdomen EUS (if all the above are negative) Rare biochemical investigations
Footnotes
Acknowledgements
We would like to thank the Departments of Gastro surgery and Pathology for their support.
Consent for publication
Informed consent for publication was obtained from all patients as well as the authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval and consent to participate
Ethical approval obtained from Institutional Ethics Committee- Biomedical Research, Indraprastha Apollo hospital New Delhi under approval number IAH-BMR-010 11-19. Informed consent to participate was obtained from all patients or their legal representatives.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Credit author statement
Dhruv Kant Mishra: Conceptualization, Methodology, Software, Validation, Formal Analysis, Investigation, Data Curation, Writing – Original Draft, Visualization, Project Administration.
Syed Uzair: Conceptualization, Methodology, Software, Validation, Formal Analysis, Investigation, Data Curation, Writing – Original Draft, Visualization, Project Administration.
Amit Pandita: Resources, Writing – Review & Editing, Supervision.
Varsha Kachroo: Resources, Writing – Review & Editing, Supervision.
Akash Batra: Resources, Writing – Review & Editing, Supervision.
Yogesh Batra: Resources, Writing – Review & Editing, Supervision, Funding Acquisition.
Data availablity statement
All data supporting this study are available within the article and its supplementary materials. Further inquiries can be directed to the corresponding author.
Use of artificial intelligence
No use of artificial intelligence.
Human ethics
The study was conducted in accordance with the principles of the Declaration of Helsinki and the IEC guidelines.