
Abstract
Introduction:
Knee dislocations are an uncommon type of dislocation that requires surgical interventions and ligament reconstruction. There are various configurations and classifications of knee dislocation as described in Kennedy system, which is based on the direction of dislocation, and Schenck system based on the pattern of ligament injury. A multitude of causes can result in an irreducible knee dislocation.
Case report:
We report a case of 57 year old male patient with irreducible knee dislocation due to interposition of the vastus medialis muscle.
Results:
A rare case of irreducible knee dislocation due to interposition of vastus medialis that required open reduction is described.
Conclusion:
Vastus medialis muscle interposition is a rare cause for irreducible knee dislocation, and one needs to aware of this to decreased morbidity.
Introduction
A dislocation is a joint injury where the ends of two connected bones come apart with complete loss of joint integrity. Shoulder, fingers, toes, patella and hip are amongst the common types of joint dislocations, whereas the knee (0.5%) is itself a rare occurrence.[1-7] These injuries require special surgical intervention and reconstruction given its high association with complex multiligament injuries and potentially life-threatening neurovascular complications.
Younger patients are more susceptible to knee dislocation, with a male-to-female ratio 4:1.[1,8] Injuries commonly involve high-energy trauma typical of motor vehicle accidents; however, relatively lower-energy injuries of impact sports have become increasingly common.[1,9–11] The injury mechanism often involves a hyperextension force, posterior tibial translation, rotational loads or combination of all elements.[1,9] Irreducible knee dislocations are a rarity to encounter, with common causes resultant of soft tissue interposition. Common clinical finding to suspect the reducible knee dislocation is a ‘dimple sign’ or ‘pucker sign’.[3,12–14]
Case Report
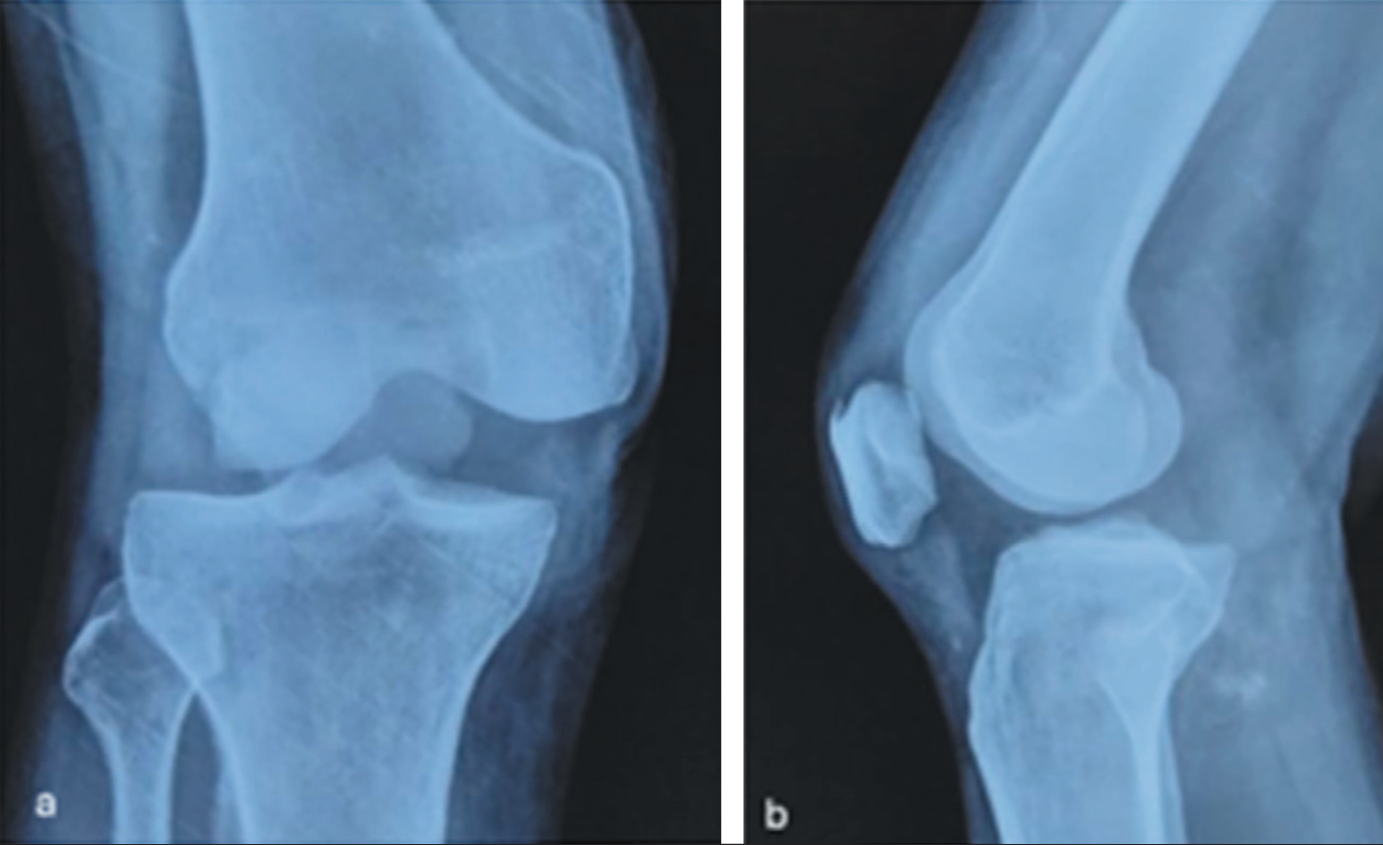
Following a high-velocity motor vehicle accident, a 57-year-old male patient presented to the emergency department. From immediately following the crash, the chief complaint was severe right knee pain. There was a visible swelling around the knee with puckering of the skin across the anteromedial aspect with an obvious visible deformity. On physical examination, the patient had an irreducible posterolateral knee dislocation with valgus deformity and additional lateral patellar dislocation. This was consistent with the initial radiograph [Figure 1] with soft tissue mass in the intercondylar region. No fracture or intra-articular loose bodies. Neurovascular integrity appeared intact; hence computed tomography (CT) angiography was not performed. A closed reduction was then attempted, although the dislocation was not successfully reduced.
Anteroposterior (AP; a) and lateral (b) radiographs of the dislocated right knee
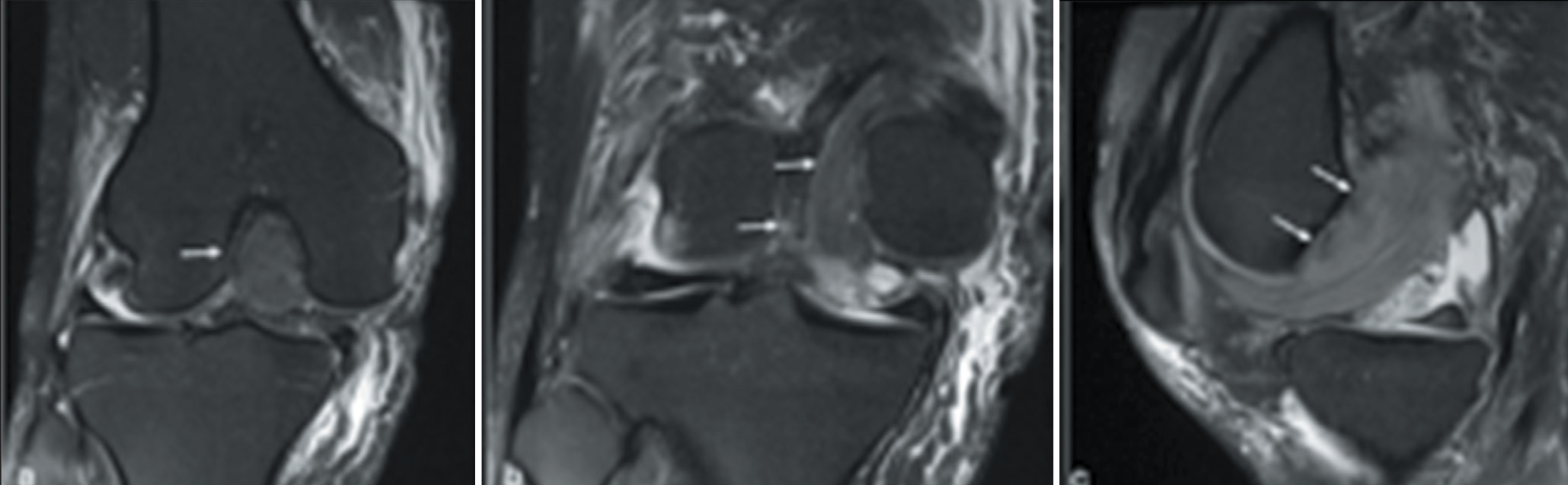
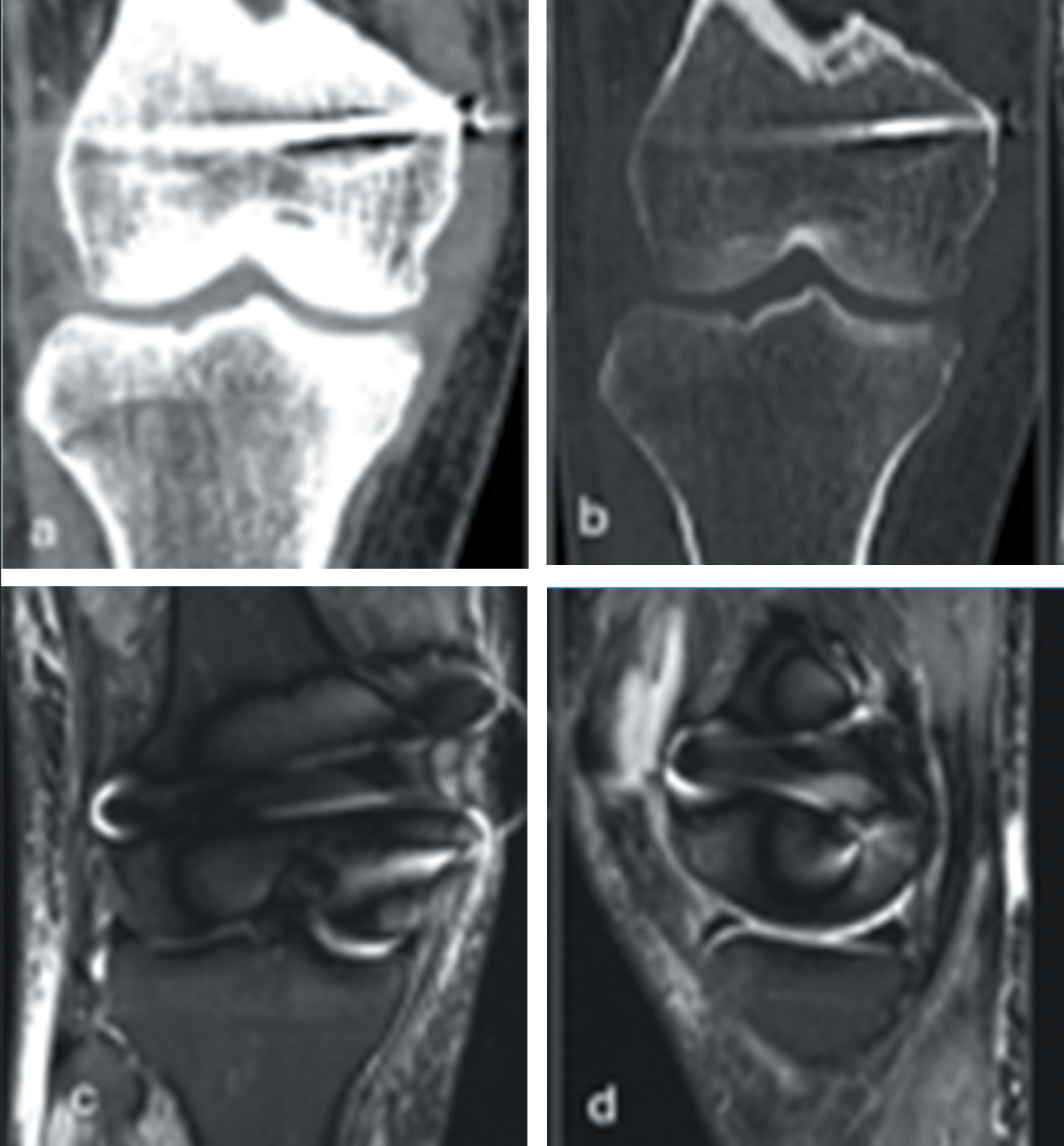
Further characterisation with magnetic resonance imaging (MRI) identified complete rupture of both anterior and posterior cruciate ligaments (ACL and PCL), medial patellofemoral ligament (MPFL), as well as of both medial and lateral collateral ligaments. There was an additional tear through the medial meniscus anterior horn. There was a surprising finding whereby a large component of the lateral portion of vastus medialis (VM) had displaced into the intercondylar notch to partially interpose the tibiofemoral joint. Longitudinal splitting through the vastus medialis obliquus (VMO) permits enclosure and ‘buttonholing’ of the medial femoral condyle through the distal VM muscle belly with intact distal VMO footprint into the superomedial patellar margin. These VM fibres displaced into the intercondylar notch were responsible for the irreducible knee dislocation [Figure 2]. There was no associated fracture or haematoma. The patient underwent uncomplicated surgical reduction of the knee joint with combined MCL and MPFL reconstruction. Postoperative MRI and CT scans were performed showing normal VM position and intact MCL and MPFL reconstruction [Figure 3]. He is scheduled for a staged ACL and PCL reconstruction at a future date.
Proton-density (PD) fat-saturated (FS) coronal (a, b) and sagittal (c) sequences showing dislocated knee and interposition of vastus medialis (arrows)
Coronal soft tissue (a) and bone (b) CT windows; and coronal (c) and sagittal (d) PDFS images showing reduced knee dislocation with MCL reconstruction
Discussion
Knee dislocations are very rare dislocations and account for approximately 0.5% of all dislocations.[1–7] It accounts for approximately 0.02%-0.2% of all traumatic injuries.[7,15,16] Young patients are more prone to knee dislocation with a male-to-female ratio of 4:1.[1,8] Common associated injuries with knee dislocation are ACL, PCL, medial collateral ligament and lateral collateral ligament tear. Irreducible knee dislocations are even rare condition to encounter in day-to-day practice.[2] Common cause of irreducible knee dislocation is interposition of the soft tissue such as muscles, tendons or intra-articular loose bodies in a dislocated knee. Isolated dislocations of the patella in the absence of dislocation of the distal femur and proximal tibia occur in injuries with much lower impact and cause limited morbidity because the underlying neurovascular structures typically remain uninjured.[4]
Irreducible posterolateral dislocation of the knee joint is considered a rare complication, and it is important to recognise and treat this condition promptly because it cannot be reduced by closed methods.[6]
In our case, posterolateral irreducible knee dislocation required surgical management because a large component of distal fibres of the VMO muscle was displaced inside the tibiofemoral joint which prevented the closed reduction. Significant valgus force is responsible for posterolateral dislocation of the knee causing injury to the medial retinaculum and subsequent interposition of the VM muscle. MRI emerged as a crucial diagnostic tool for assessment of the cause of the irreducibility and associated ligament injury and provided the foundation for planning the further management and follow-up of the patient. However, in other associated life-threatening fractures and neurovascular injuries, management of such injuries is a priority. MRI in such life-threatening injuries should be avoided as the first line of investigation.
Overall, a rare orthopaedic emergency such as irreducible knee dislocation should undergo an MRI examination in absence of the other life-threatening fractures or neurovascular injuries to assess the cause of the irreducibility. MRI also provides a noninvasive alternative tool to arthroscopy in such cases. Identifying complicated knee dislocation with soft tissue interposition and emergency open reduction is vital to minimise the neurovascular complication.[5,17]
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors Karthikeyan P. Iyengar and Rajesh Botchu are members of the Editorial Board of Apollo Medicine. The authors did not take part in the peer review or decision-making process for this submission and have no further conflicts to declare.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
None.
Informed consent
Informed consent was obtained from the patient.
Credit author statement
All authors contributed significantly to the paper.
Data availability
None.
Use of artificial intelligence
None.