
Abstract
Introduction:
Bronchogenic cysts are a rare congenital anomaly. The majority of cases are reported in children, and they are extremely rare in adults. Extrathoracic presentation is also uncommon. The patient with a neck cyst may present with a variety of symptoms, ranging from an asymptomatic neck swelling or a fistula to other broader symptoms like neck pain or dysphagia.
Case Report:
We report a case of a 51-year-old female presented with chronic mild throat pain for one year. Examination findings were within normal limits except for a doubtful swelling on the right side of the neck while palpating. In radiological examination, a cyst was found at the cricoid level.
Conclusion:
Surgical excision was done and the histopathological report suggested a bronchogenic cyst.
Keywords
Introduction
We are presenting a case of an adult woman with a neck cyst. Congenital cystic lesions in adults include thyroglossal duct cysts, dermoid cysts, branchial cleft cysts and rare causes like cervical bronchogenic cysts and cervical thymic cysts.[1] Acquired lesions, which are mainly due to neoplastic or inflammatory aetiology, should also be considered in adult patients.
When the symptoms and clinical history of the patient do not elucidate much into the diagnosis, and the clinical examination was also doubtful about the presence of a neck swelling, the radiological imaging of the neck could find a cystic swelling in the neck. Radiological imaging can interpret the nature of the lesion, its extent and its relation with surrounding structures. Once the cystic nature of the lesion is detected by imaging, the differentials to be considered vary from the acquired and congenital causes of the neck cyst including the rare causes. The evaluation of a patient with a suspected neck cyst should progress in an algorithmic order, starting from clinical examination to radiological investigation, and ultimately, histopathological examination is essential for establishing the final diagnosis.
Case Description
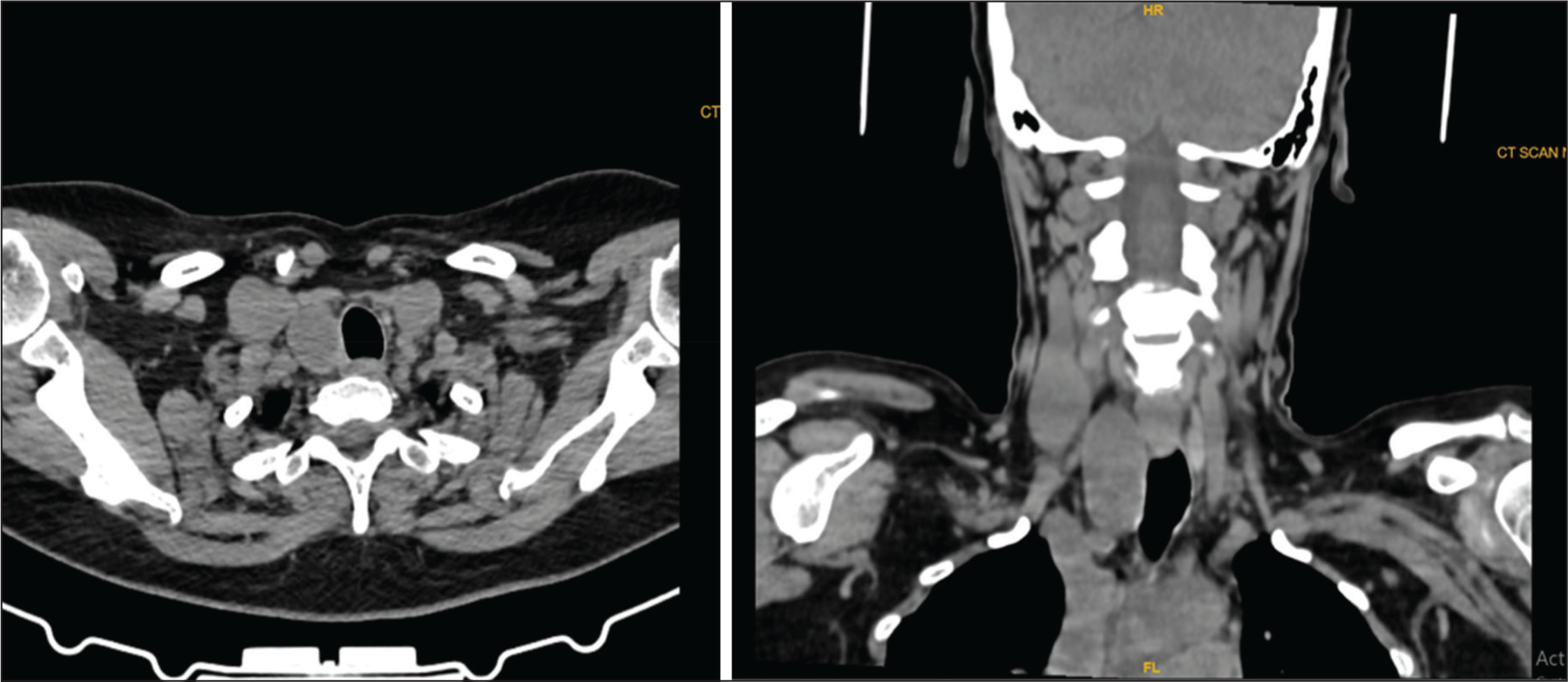
A 51-year-old female patient presented with dull, right-side, mild throat pain for one year. There was no dysphagia, odynophagia, breathing difficulty or voice change for the patient. Indirect laryngoscopy examination was normal. There was no visible swelling in the neck. On palpation, there was a doubtful swelling at the level of the cricoid region. The patient was sent for computed tomography (CT) scan imaging of the neck, which showed a well-circumscribed, smooth-margined, ovoid, hypodense lesion in the right tracheo-oesophageal groove, extending from the level of the cricoid region and small retrosternal extension, causing anterolateral displacement of the contents of the right carotid sheath and medially causing subtle tracheal deviation. Two tiny hyperdense foci (isodense to thyroid tissue) are noted along the anterior wall of the cyst [Figure 1A and B]. The common differentials were branchial cleft cyst, an ectopic thyroid tissue with thyroglossal cyst, a thyroid cyst or a parathyroid cyst. The surgery proceeded by making an anterior skin crease incision between the cricoid cartilage and the suprasternal notch. The cyst measured 5 × 2 × 2 cm and was found posteromedial to the thyroid gland and in the tracheo-oesophageal groove. The right side recurrent laryngeal nerve was seen crossing over the cyst wall, which was identified and preserved [Figure 2A and B]. The cyst wall adhered to the tracheal wall and the cricopharyngeal musculature, which made the dissection difficult. However, the surgery was done meticulously without any rent in the tracheal wall or the pharyngeal mucosa. The cyst was excised in toto without any leakage of content. The patient was on nasogastric tube feeding for two days, after which she started on oral feeds. The patient was given only painkillers. No antibiotics were given.
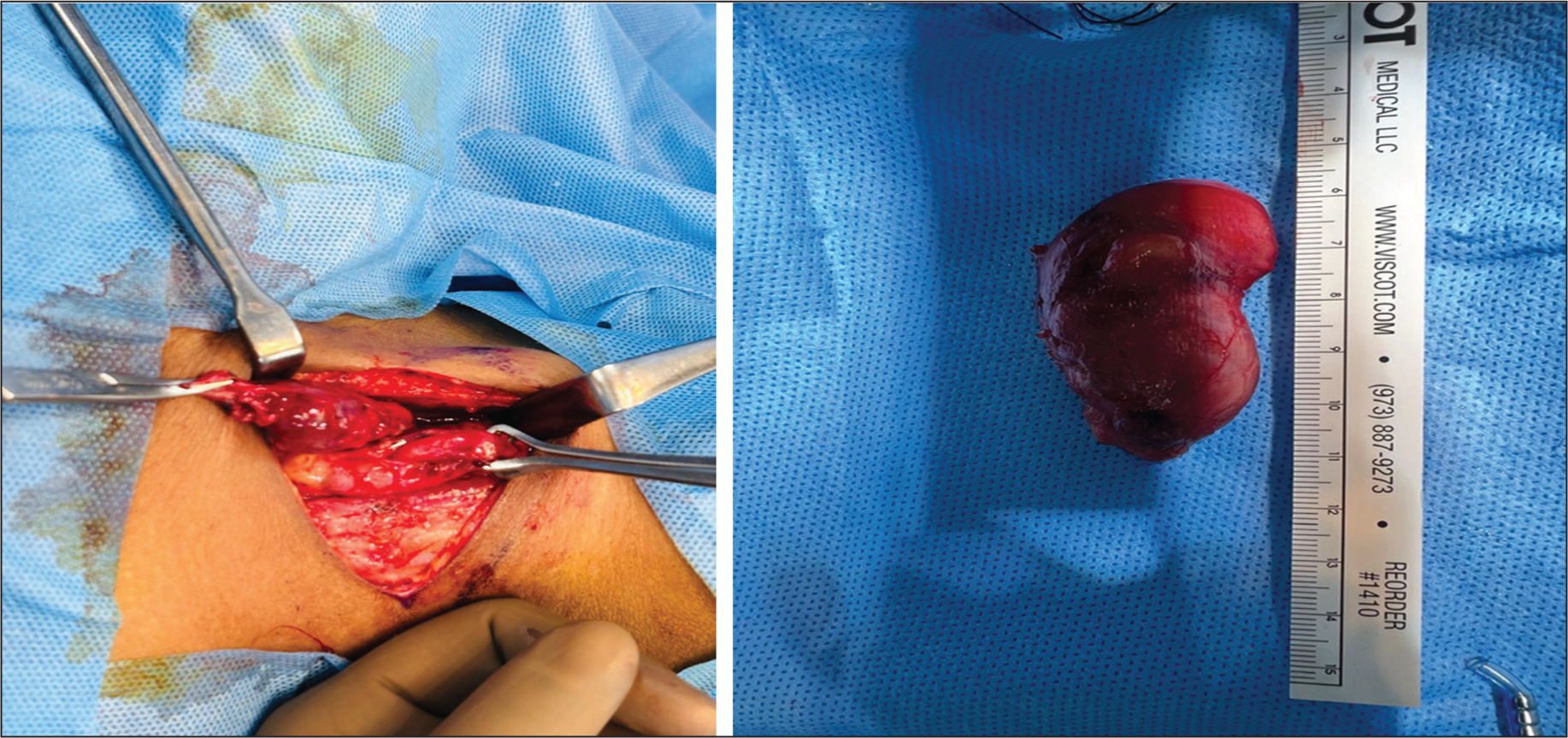
The cyst was filled with yellow mucoid material and solid areas were identified. Histologically, the cyst wall is composed of stratified ciliated respiratory-type epithelium associated with smooth muscle bundles, seromucinous glands and focal hyaline cartilage. Associated fibrosis and chronic inflammation with peri-glandular chronic lymphocytic infiltration and focal areas of hyalinisation were noted. All these features were suggestive of a bronchogenic cyst [Figure 3].

The patient is under follow-up and is asymptomatic with no dysphagia, dyspnoea or dysphonia. The patient is under follow-up for six months with no recurrence to date.
Discussion
Bronchogenic cysts are abnormal growths that develop from the early developmental stages of primitive foregut, typically between the third and seventh week of gestation.[2] They can be connected to the airways or exist independently. These cysts grow due to fluid buildup inside them. In most cases, they occur in the lung parenchyma or mediastinum near the tracheobronchial tree, though they can also be found near the neck, stomach and subcutaneous tissue. Their unusual locations suggest these abnormal cell growths might originate early during organogenesis.[3,4] Maier in 1948 classified the bronchogenic cysts based on location into: paratracheal, carinal, hilar, paraesophageal and, miscellaneous groups.[3,5]
A review of the literature of 14 cases of adult cervical bronchogenic cysts was done by Moz et al. in 2009, describing the cysts to occur in supraclavicular, suprasternal, paratracheal, pretracheal and thyroid regions. Many of the cases belonged to the paratracheal and thyroid areas.[5–16] A similar study by Santos et al. in 2019, where they did a literature review of 33 articles from PubMed research, yielded 49 cases of cervical bronchogenic cysts, with a slight female predominance (31 females and 18 males). The age of diagnosis ranged from 18–70 years, with most cases (31 out of 49) diagnosed before age 50. Most cysts were found in the lower neck and most were located in the midline.[17] The location of cervical bronchogenic cysts in our reported case is very similar to the location of the case reported by McManus et al. in 1984 of an adult male of 34 years, with the cyst between the right carotid sheath and tracheo-oesophageal groove, beginning at the cricoid cartilage and extending into mediastinum.[7]
Cervical bronchogenic cysts often do not cause any symptoms. However, a cyst may grow larger and can produce compressive symptoms. It can compress the trachea causing shortness of breath, coughing and dysphagia due to compression of the oesophagus. In rare cases, infection can develop, leading to abscess formation or sinus tract formation with pus drainage.[18]
Complications of a bronchogenic cyst may include rupture of the cyst, secondary infection and malignant transformation. In literature, malignancy of bronchogenic cysts has been reported in adults and includes adenocarcinoma, squamous cell carcinoma, bronchoalveolar carcinoma, large cell carcinoma and mucoepidermoid carcinoma.[19] Malignant melanoma arising from a cutaneous bronchogenic cyst in the scapular area has also been reported.[12]
A bronchogenic cyst should be differentiated from other neck cysts including branchial cleft cysts, thyroglossal duct cysts, cervical thymic cysts, cystic degeneration of lymph nodes, cystic papillary carcinoma of thyroid gland, cystic hygromas, laryngocele, pharyngocele, lymphatic and vascular malformations, epidermal cysts, dermoid cysts, oesophageal duplication, tracheal diverticulum and cystic neuromas.[5,13–18]
The ultrasound (US) scanning of the neck is the most frequently used imaging technique for neck masses as it reveals the cystic nature of the mass and defines its size, extent and relationship to the surrounding structure. The US may be adequate most times, but a CT scan provides additional information regarding the internal calcification and extent of the lesion, especially for larger masses where the full extent cannot be visualised with the US.[11,14,15] Magnetic resonance imaging is supplementary and can be considered for additional information, particularly for more deep-seated lesions due to its multiplanar capability and better contrast resolutions.
A definitive diagnosis can be made only by the histological examination of the excised cyst. In terms of gross appearance, the cyst will have smooth walls and be either unilocular or multilocular. The content of the cysts will be mostly mucoid and sometimes gelatinous or pus-filled. Histologically, bronchogenic cysts are usually lined by columnar, ciliated, pseudostratified epithelium, with potential areas of metaplasia in some places. Airway components like smooth muscle, cartilage plates and bronchial glands are also found in the cyst wall. In rare cases, it has been reported that the cyst wall contains adipose and nerve structures.[20]
The mainstay of treatment of a cervical bronchogenic cyst is surgical excision via the transcervical approach. The proximity of the cervical cyst to the major blood vessels, trachea, oesophagus and recurrent laryngeal nerve makes the surgery challenging. In accordance with St. Georges et al., in a significant number of patients, the cyst was adherent to nearby organs such as the lung, oesophagus, pericardium or tracheobronchial tree.[4] Recurrences are rare in a case of complete cyst excision. In our case, the recurrent laryngeal nerve was running across the cyst wall and the cyst was attached to the oesophageal muscles and tracheal wall. However, a complete resection of the cyst was achieved without complications.
Conclusion
In our case, the absence of an obvious neck swelling was a tricky situation to proceed with. However, the one-year history of throat pain and the doubtful swelling in the neck prompted us to send for a radiological examination. Neck lumps in adults can account for a variety of pathological conditions. Radiological imaging could help us in providing the nature and extent of lesion, but the final diagnosis will depend on a histopathological examination. Surgical excision is both curative and diagnostic. The surgery might be challenging for many because of the proximity to the vital structures and due to the attachment of the cyst to the tracheal and oesophageal wall.
Footnotes
Acknowledgements
Thanks to Dr Shivashankari—Research assistant, Research department and Mr Sam Daniel—Physician assistant, Department of ENT, Head and Neck Surgery.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
We did not get an institutional ethical committee approval since it was not an observational or interventional study. This is a routine case which every surgeon does in their routine practice.
Informed consent
Informed consent has been obtained from the patient.
Credit author statement
FJ participated in literature search, data collection and analysis and manuscript preparation.
BM participated in conceptualisation, investigation and management of the patient, supervision and manuscript editing.
Data availability
Data related to the case report is available with the corresponding author.
Use of artificial intelligence
Nil.