
Abstract
Introduction:
Hyperglycaemia, both chronic and stress-induced forms, plays a significant role in determining outcomes for critically ill patients. Chronic hyperglycaemia, reflected by elevated HbA1c levels, contributes to a pro-inflammatory state, while stress-induced hyperglycaemia during acute illness increases the risk of poor outcomes. Novel metrics like the glycaemic gap and stress hyperglycaemia ratio (SHR) have shown promise in predicting clinical outcomes. This prospective observational study aimed to examine the relationship between admission hyperglycaemia and 30-day mortality in critically ill patients admitted to the intensive care unit (ICU) at a tertiary care centre in South India.
Methods:
A prospective observational study was conducted which included 200 patients who were admitted to the ICU. Key markers such as HbA1c, admission venous blood glucose, glycaemic gap, and SHR were assessed. The clinical course of the patients and 30-day mortality were monitored.
Result:
The study found significant correlations between an elevated glycaemic gap and SHR with increased 30-day mortality. The glycaemic gap cutoff of 45.49 mg/dL and SHR cutoff of 1.355 effectively predicted mortality, with high sensitivity and specificity. Elevated glycaemic gap and SHR were also associated with longer ICU stays, mechanical ventilation, and renal replacement therapy.
Conclusion:
The results suggest that glycaemic gap and SHR are reliable markers for predicting clinical outcomes in critically ill patients, with higher values correlating with poorer prognoses. These markers, in conjunction with blood glucose levels and HbA1c, can be used to assess disease severity and guide clinical management, especially in resource-limited settings.
Keywords
Introduction
Diabetes mellitus is a chronic disease that carries high mortality and morbidity and is prevalent across the world. One of the most important causative factors for type 2 diabetes mellitus is obesity, which is often associated with metabolic syndrome. Hyperglycaemia mediates inflammation through various interlinked pathways, leading to oxidative stress and endothelial dysfunction. Chronic hyperglycaemia leads to an immunosuppressed and prothrombotic state, leading to microvascular and macrovascular complications, which worsen the functional status of the patient.[1,2]
Several metrics are used to assess the glycaemic status and control. Despite its limitations, HbA1c is the most widely accepted marker of chronic hyperglycaemia. Studies have established HbA1c as an independent marker of disease severity and mortality in the intensive care unit (ICU).[3] While diabetes causes chronic hyperglycaemia, there are situations (e.g., acute illnesses) which cause temporarily elevated blood glucose levels and are called stress-induced hyperglycaemia. It was initially thought to be beneficial to the patient as it was categorised as a physiological adaptation response. However, later studies began reporting an increase in the incidence of mortality and poor functional outcomes in patients with hyperglycaemia.[4,5] This gave rise to new concepts in stress hyperglycaemia, namely glycaemic gap and stress hyperglycaemia ratio (SHR). Many studies were undertaken, and a positive correlation was found between these markers and poor functional outcomes. However, only a few studies in India looked into the effect of hyperglycaemia on outcomes in critically ill patients, and they focussed either only on HbA1c, random blood glucose level, or glycaemic gap.[6-8]
Thus, the data available in India, which incorporates both chronic hyperglycaemia and stress-induced hyperglycaemia and their effects on outcomes in critically ill patients, is scanty. Our study is an effort to provide important data on the relationship between hyperglycaemia (both acute and chronic) and clinical outcomes. We studied the relationship between admission glucose levels and the 30-day mortality in critically ill patients admitted to the ICU in a tertiary care centre in southern India.
Material and Methods
A prospective observational study was conducted among patients admitted to the ICUs of Apollo Hospital, a tertiary care centre in South India, from July 2022 to December 2023. The institutional review board approved this study. Informed consent was obtained from the patients. Privacy and patient confidentiality were maintained as per norms.
Inclusion Criteria
Patients older than 18 years and admitted to the ICU for at least 24 hours.
Exclusion Criteria
Patients with two or more episodes of hypoglycaemia (<70 mg/dL) during the period of observation which is independently associated with increased mortality and this study focuses on hyperglycaemia. Patients who had previously required renal replacement therapy and/or mechanical ventilation. Patients with severe anaemia (Hb < 9 g/dL) due to decreased red cell turnover and patients with haemoglobin variants that interfere with HbA1c measurement.
Methodology
A total of 200 consecutive patients who met the inclusion and exclusion criteria were included in the study. Detailed clinical history was collected for comorbidities. Random venous blood glucose level was collected at the time of admission. HbA1c was done within three days of admission. Glycaemic gap and SHR were calculated as per the standard formulae. The parameters studied include 30-day mortality, length of hospital and length of ICU stay, need for mechanical ventilation and need for renal replacement therapy.
Statistical Analysis
Data entry was done in the MS Excel spreadsheet. Descriptive statistics were presented with frequency (percentage) and mean ± SD for the categorical and continuous factors, respectively. The normality of the data was checked by using the Shapiro-Wilk test. Karl-Pearson/Spearman Rank order correlation test was used to determine the linear relationship between two independent factors. Chi-square/Fisher’s exact test was used to determine the association between two independent categorical factors depending on the cell count. Student’s t-test was used to determine significant changes between two independent groups. A P < .05 was considered statistically significant. Data analysis was carried out by using the statistical software SPSS (IBM, 28.0).
Results
The mean age of the patients included in our study was 60.48 ± 13.379. Male patients (76.5%) were more compared to female patients (23.5%). Diabetes mellitus (78%) was the most common comorbidity, followed closely by hypertension (58.5%). Coronary artery disease and chronic kidney disease were present in 24.5% and 9% of the study population. 5.5% had chronic obstructive pulmonary disease, and 1.5% had chronic liver disease.
The mean HbA1c of the patients included in our study was 7.85 ± 1.9606. The mean venous blood glucose at admission was 227.8 ± 118.1595. The mean estimated average blood glucose calculated from HbA1c was 178.595 ± 56.269. The mean glycaemic gap was 49.205 ± 92.6132. The mean SHR was 1.267 ± 0.4524.
42.5% of the patients had acute coronary syndrome. 11% of the patients were admitted with sepsis and 7.5% were admitted with acute ischemic stroke. 77.5% of the patients included in the study were alive at the end of the 1-month study period [Table 1]. The mean length of hospital stay was 7.81 ± 6.952 days. The mean length of ICU stay was 5.15 ± 5.578 days.
Comparison between outcome at one month and HbA1c, venous blood glucose at admission, glycaemic gap and SHR

Mechanical Ventilation was needed in 55 patients (27.5%) of the study population [Table 2], and renal replacement therapy was needed in 20 patients (10%) of the study population [Table 3].
Comparison between mechanical ventilation and HbA1c, venous blood glucose at admission, glycaemic gap and SHR

Comparison between renal replacement therapy and HbA1c, venous blood glucose at admission, glycaemic gap and SHR

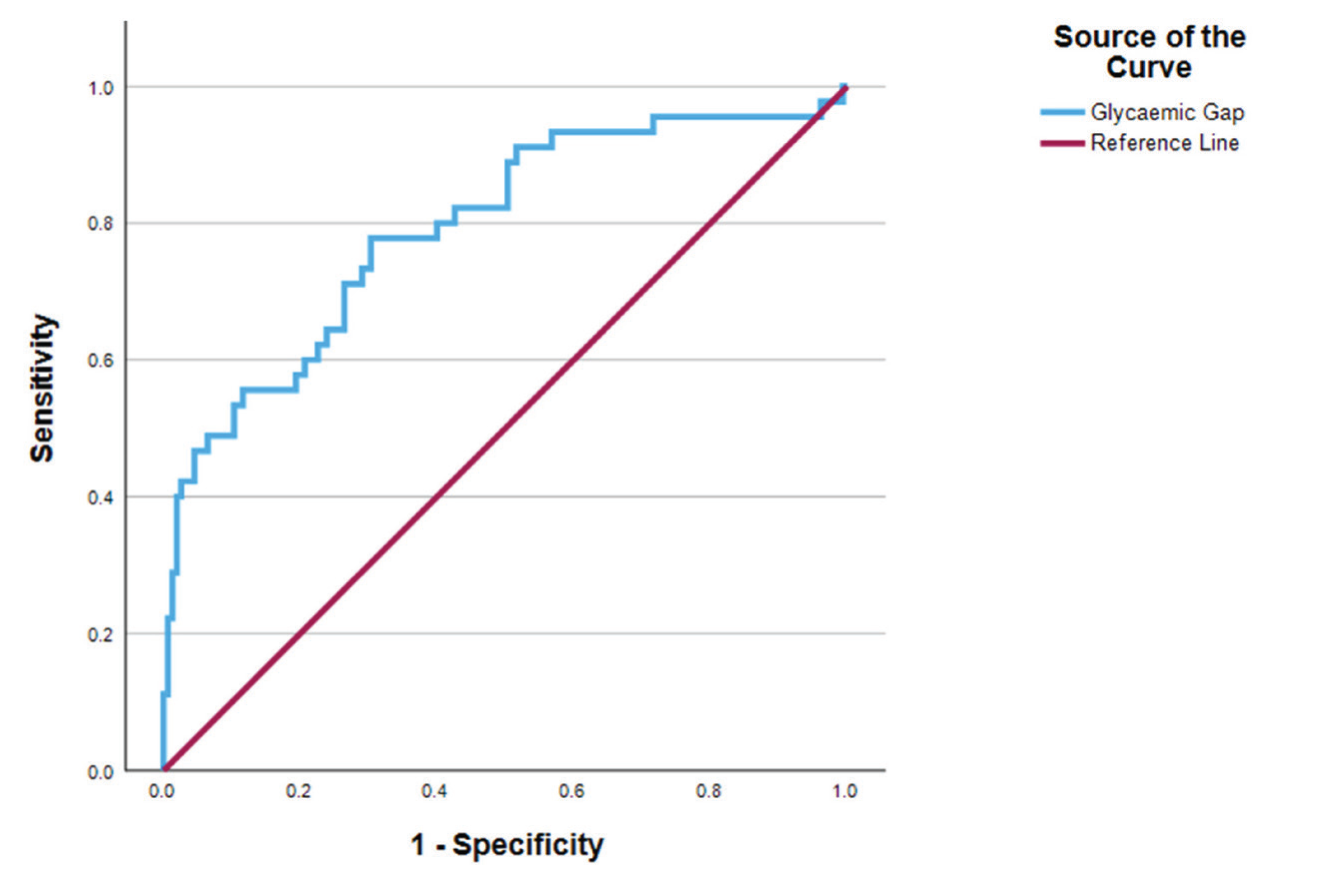
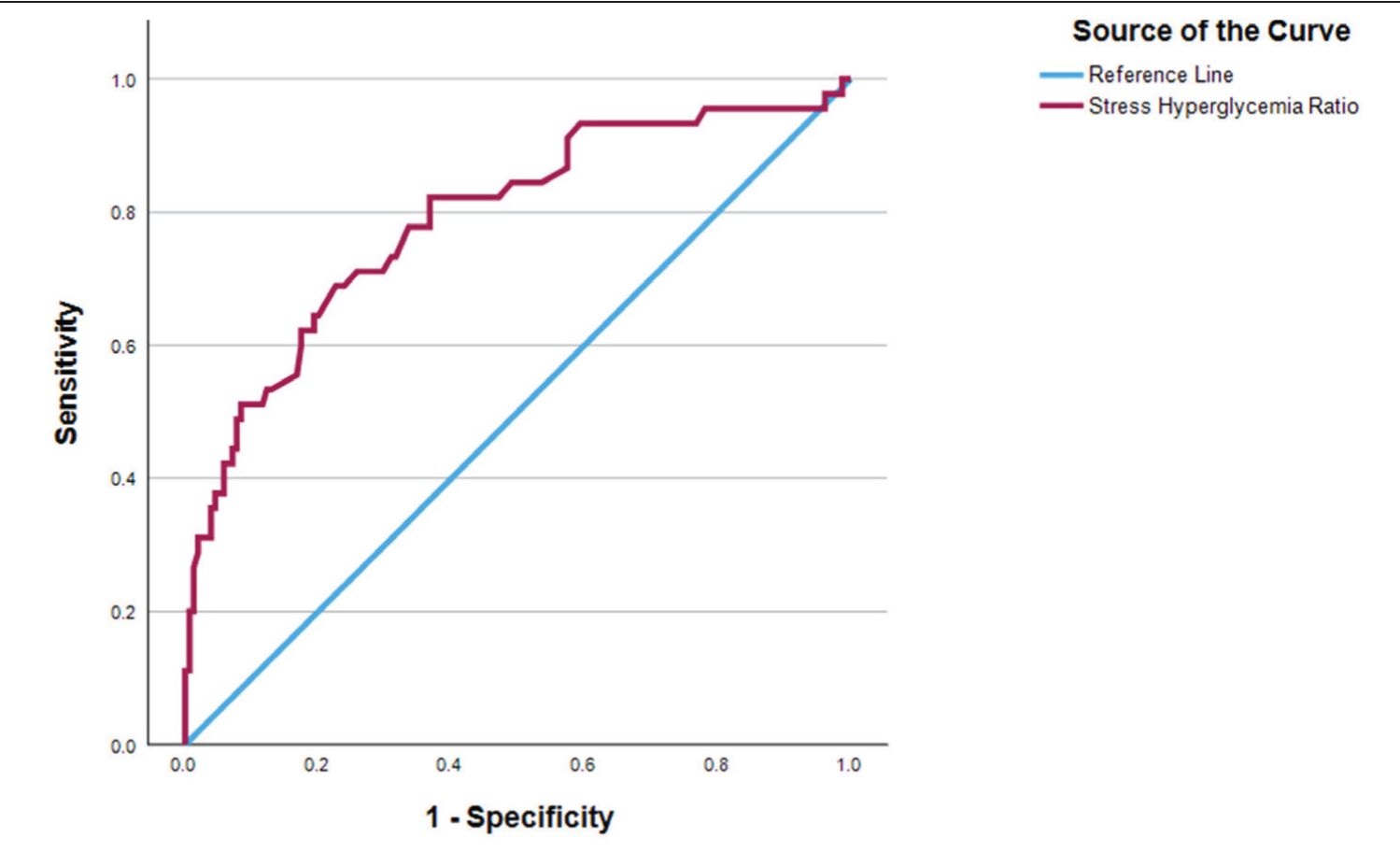
The glycaemic gap showed a significant correlation with outcome at one month in all patients. The glycaemic gap cut-off of 45.49 is found to be discriminatory for predicting 30-day mortality with Area Under ROC = 0.793, P < .01; Sensitivity 77.8%, Specificity 69.7% [Figure 1]. SHR also showed a significant correlation with outcome at one month in all patients. SHR cut-off of 1.355 is found to be discriminatory for predicting 30-day mortality with Area Under ROC = 0.789, P < .01; Sensitivity 68.9%, Specificity 77.4% [Figure 2].
Receiver operator characteristic showing a comparison between glycaemic gap and outcome at one month
Receiver operator characteristic showing comparison SHR and outcome at one month
Discussion
This study included 200 patients admitted to the ICU of our hospital for at least the initial 24 hours during the study period. The study’s main goal was to study the relationship between admission hyperglycaemia and mortality and morbidity outcomes. It aimed to determine the ability of HbA1c, venous blood glucose at admission, glycaemic gap and SHR in predicting 30-day mortality. The low cost of the tests used in our study and the fact that they are routinely done in many centres can help in identifying markers of severity and outcome which can be easily used even in resource-limited settings.
The mean age of the patients included in our study was 60.48 ± 13.379. The mean age of patients alive after 30 days was 60.07 ± 13.379, while those who were not alive were 61.89 ± 13.432. There was no significant correlation between the age of the patient and 30-day mortality. The mortality rate was slightly higher in female patients (25.5%) compared to male patients (21.6%). Patients with a history of CAD had the highest mortality rate among the studied comorbidities (32.7%), and it also showed a significant correlation with 30-day mortality (P = .05)
In our study, higher HbA1c showed a significant correlation with 30-day mortality outcomes in only the study participants with Diabetes Mellitus. In our study, as the patients who had previously undiagnosed diabetes mellitus with HbA1c more than 6.5% had been added to the Diabetes Mellitus group, our study showed a significant association between HbA1c and 30-day mortality in only the Diabetes Mellitus group. Higher HbA1c also showed a significant correlation with length of hospital stay, need for mechanical ventilation and renal replacement therapy.
Similar to previous studies, higher venous blood glucose at admission showed a significant correlation with 30-day mortality, length of hospital stay, length of ICU stay, and need for mechanical ventilation and renal replacement therapy.
The glycaemic gap is calculated as the difference between admission venous blood glucose level and ADAG. It can be used as a tool to eliminate the impact of chronic hyperglycaemia in patients with pre-existing diabetes.[9] A higher glycaemic gap significantly correlated with 30-day mortality, length of ICU stay, and need for mechanical ventilation and renal replacement therapy in all patients. A clear increase in mortality rate was seen in analysing the data after dividing into groups based on percentiles. The cut-off for predicting 30-day mortality was found to be 45.49. In a study published in 2018, ICU Mortality was predicted by a glycaemic gap cut-off of 43.31 mg/dL,[7] which is similar to our study.
The SHR is calculated as the ratio between admission venous blood glucose level and ADAG. Similar to the glycaemic gap, it is a novel marker for Stress-Induced Hyperglycaemia. A higher SHR was significantly correlated with 30-day mortality, length of ICU stay, and need for mechanical ventilation and renal replacement therapy in all patients. The cut-off for predicting 30-day mortality was found to be 1.355. In a study published in 2022, it was shown that SHR had an independent relation to mortality and risks of MACEs in STEMI patients. Patients with SHR ≥ 1.329 and underlying diabetes exhibited the highest risk of MACEs.[10]
Conclusion
In conclusion, venous blood glucose at admission, glycaemic gap and SHR can consistently predict the clinical course and outcome in critically ill patients. A higher level of the above parameters is more likely to be associated with increased 30-day mortality and increased morbidity. However, this is a single-centre observational study, and the patients who expired within 24 hours were not included in the study. The study population was heterogeneous as it included all patients admitted to a multidisciplinary ICU, so the study findings have to be interpreted with caution.
Footnotes
Acknowledgements
To Dr Shivasankari: research assistant and Mr Logesh: Biostatistician, Research department, Apollo Hospital, Chennai.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The study was approved by the Institutional Ethical Committee under approval number ASH–DNB-028/06-22.
Informed consent
Informed consent has been obtained from all the patients who met the eligibility criteria.
Credit author statement
ES participated in data acquisition, literature search, investigations, data analysis and manuscript preparation.
JC and NK participated in conceptualisation, investigation, supervision, data analysis and manuscript editing.
All the authors reviewed and approved the manuscript.
Data availability
Data presenting the study’s findings is available with the corresponding author.
Use of artificial intelligence
The use of artificial intelligence is not relevant to this article, as it does not involve AI technologies or methodologies in its analysis or conclusions.