
Abstract
Background and Aim:
Basal cell carcinoma (BCC) is one of the most common cancers worldwide, accounting for roughly 80% of all non-melanoma skin cancers (NMSC).
Objective:
The aim of this study is to present a six-year experience in the therapy of basal cell carcinoma (BCC) of the head and neck region by analysing age, sex, tumour placement and size, histological subtype of the tumour, reconstruction method and recurrence rates for all fully excised BCCs in the head and neck region.
Methods:
A total of 85 cases were retrospectively reviewed, all of whom received complete treatment at our tertiary care centre between 2014 to 2020.
Results:
There were 85 confirmed cases of BCC of the head and neck region, which were categorised into BCC of the nasal, orbital, cheek, perioral, chin, neck nasolabial fold, lips, forehead and scalp. The most common age group was in the 6th decade with a slight predilection to the male sex. The most prevalent site of involvement was the nose and 51.4% of lesions were more than 2 cm in size. Recurrence rates were approximately 21%.
Conclusion:
The prevalence of BCC in our region is largely undetermined but is still a common presentation in the population due to extensive UV light exposure. BCC was more common in the male sex, and more than half of the lesions were larger than 2 cm. Despite complete excision, BCCs in the head and neck area, particularly those that are more prone to recurrence owing to anatomical and histological characteristics, should be continuously monitored to reduce morbidity and health-care expenditures.
Introduction
Basal cell carcinoma (BCC) is one of the most common cancers worldwide, accounting for roughly 80% of all non-melanoma skin cancers (NMSC).[1,2] Males in their sixth decade of life are marginally more likely to have it than females.[3] Around eighty percent of all BCCs occur in the head and neck region, as it receives the most exposure to short wave ultraviolet-B radiation of the sun, a major causative factor for BCC.[4] Metastasis is extremely rare but the cancer can spread to the regional lymph nodes as well as to the lungs and bone. The invasion and destruction of local tissue, particularly in the head and neck region, causes morbidity associated with basal cell carcinoma. Perivascular and perineural tissue invasion can also occur in very aggressive cancers. There are many treatment options available for managing BCC, such as surgical excision, topical immune-modulating creams, cryotherapy, radiotherapy, cauterisation and photodynamic treatment.[5] Amongst all available options, surgical excision is highly effective and the most utilised option for treating primary BCCs. A macroscopic clear margin of 2mm-4mm is recommended by guidelines for the surgical excision to minimise the risk of disease relapse.[6] The purpose of our study was to analyse and review the experience of our centre with BCC of the head and neck region.
Material and Methods
We performed a retrospective review of all patients who underwent surgical resection of cutaneous basal cell carcinoma (BCC) of the head and neck region with or without adjuvant treatment at our tertiary care centre from 2014 to 2020. For all patients, medical charts were reviewed to determine the quality of the data recorded. Documentation regarding patient demographics (age, gender and any other malignancy), cancer site and number of lesions, method of surgical treatment and possible reconstruction, histological data (depth and diameter) and disease recurrence were all reviewed and collected. The length of follow-up and time between initial excision and development of recurrence or new tumours was also noted. Data was entered and analysed in SPSS Version 23. Variables were expressed as numbers and percentages and chi-square test was utilised for comparison. A P value of < .05 was used as the criterion of statistical significance. Before surgery, all patients who underwent surgical excision were informed about the surgical and aesthetic risks as well as the chance of disease recurrence, and they signed an informed consent form.
Results
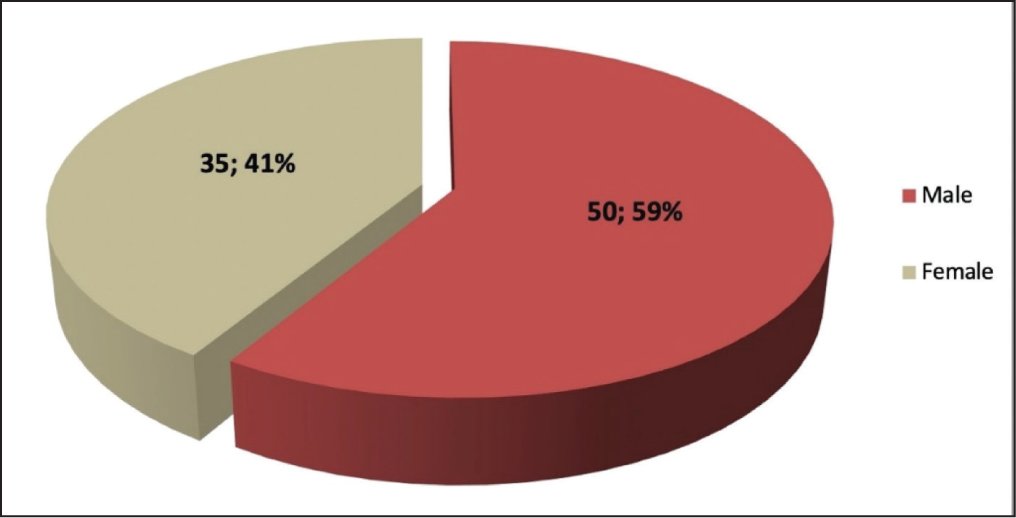
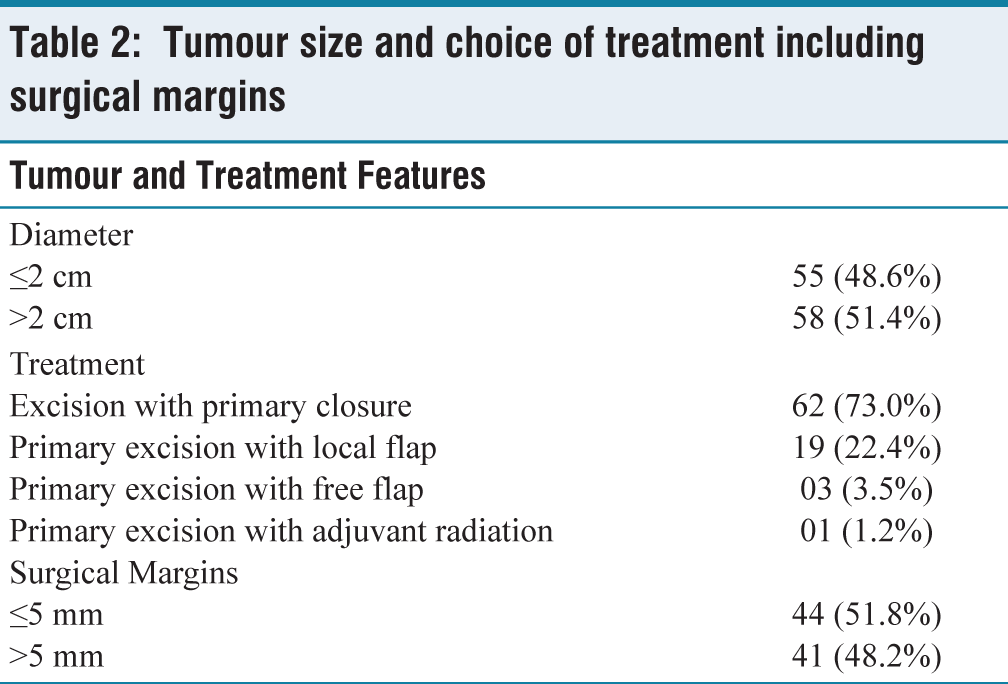
At our plastic and reconstructive surgery department, eighty-five patients with 113 lesions of cutaneous basal cell carcinoma in the head and neck region underwent surgical excision. Of those, 50 (58.8%) patients were male, as shown in Figure 1, and the mean age was 63.1 years. Seventeen patients had more than one lesion and out of these seventeen patients, six patients had three or more lesions. In addition, 58 lesions (51.4%) were more than 2 cm in size. Demographic breakdown, tumour features and choice of tumour treatment are shown in Tables 1 and 2. Pre-surgical biopsies were not performed for any of our patients as our centre does not routinely sanction the practice due to cost-effectiveness. All tumours were excised with safe margins (1 cm) and most of the defects were repaired with primary closure and followed by local flap closure [Table 2].
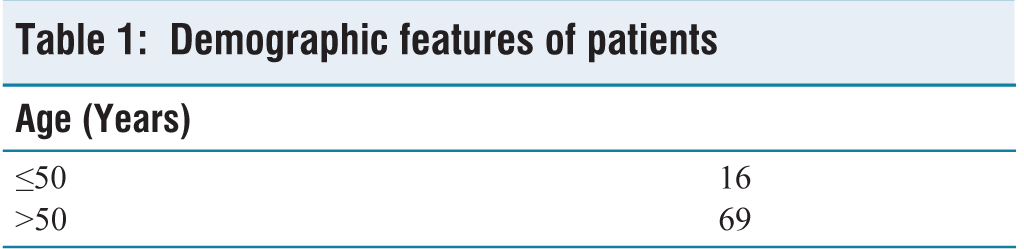
Demographic features of patients
Demographic features of patients
Tumour size and choice of treatment including surgical margins
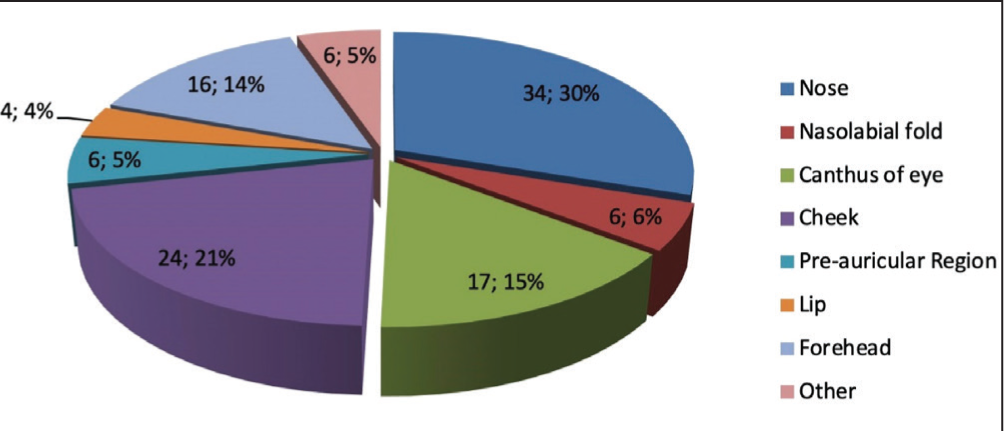
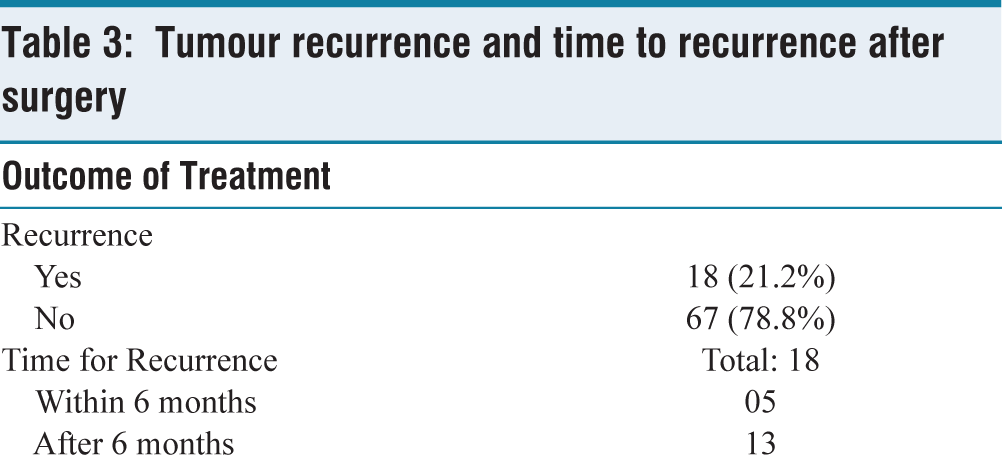
The nose (30.0%) and cheek (21.2%) were the most common sub sites, followed by the eye canthus (15.0%) as shown in Figure 2. Moreover, Table 3 shows the recurrence of 5 tumours that had previously been resected. Out of the total 85 patients, 62 had excision with primary closure, while 22 required reconstructions with a local or a free flap and 1 patient required adjuvant radiation. The 55-65 age group had a higher prevalence of patients (34.7%), which was statistically significant at P < .05.
Sub-sites of the tumour
Tumour recurrence and time to recurrence after surgery
Discussion
Basal cell carcinoma, formerly known as ‘rodent ulcer’, was first described by Jacob Arthur in Dublin in 1827.[7] The characteristic features of basal cell carcinomas are local invasiveness and slow growth. The incidence of basal cell carcinoma is increasing worldwide due to increasing environmental and industrial pollution as well as due to global warming, ultraviolet rays and depletion of the ozone layer.[8] The aetiology of basal cell carcinoma can be described as DNA damage caused by ultraviolet rays, resulting in the abnormal and uncontrolled growth of skin lesions. Mutations in the sonic hedgehog pathway also cause this malignancy in immunocompromised persons, while Bazex syndrome, Rombo syndrome, Nevoid Basal Cell Carcinoma Syndrome, Rasmussen’s encephalitis and Darier disease are all also related to basal cell carcinomas.[9,10] Furthermore, the head and neck region is also particularly susceptible to basal cell carcinomas.[11]
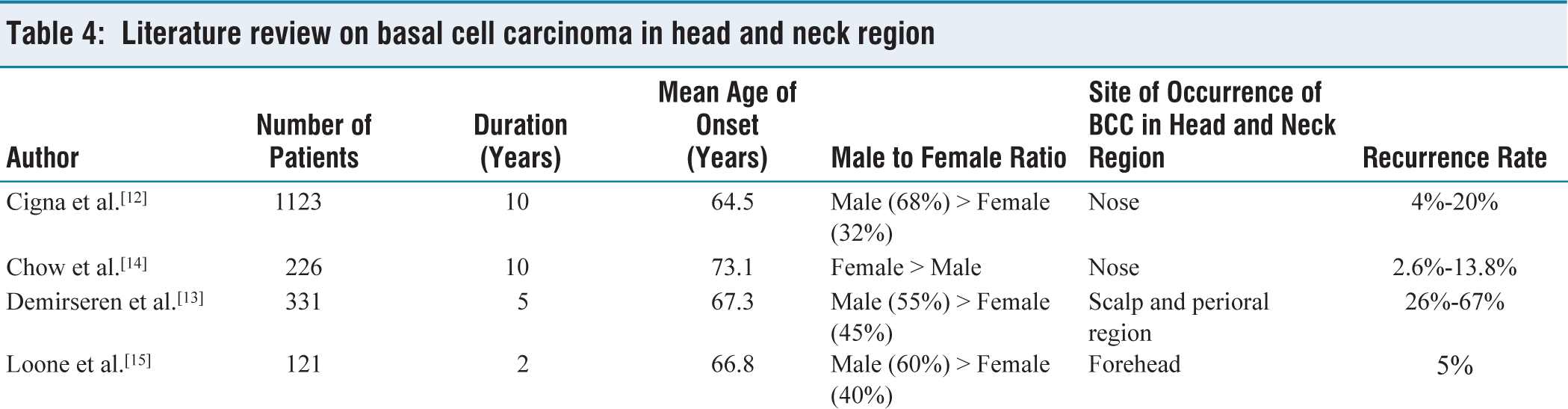
BCC was more common in male patients in our study, with 58.8% male and 41.2% female patients. This could be because men undertake more outdoor work and are hence more susceptible to sun exposure in our region. These findings are in line with those of Cigna et al.[12] and Demirseren et al.,[13] while on the other hand, Chow et al.’s[14] report states that BCC is more prevalent among women than men. In our study, most BCC lesions are found in people aged above 60, with an average age of 63.1 years. Cigna et al.[12], Demirseren et al.[13] and Loone et al.[15] illustrated similar results as shown in Table 4.
Literature review on basal cell carcinoma in head and neck region
Our findings revealed that the nose is the most common site of BCC with the highest rate of recurrence and inadequate margins and similar findings have been reported by Chow et al.[14] and Janjua et al.[16] This can be explained by the embryonic fusion planes, as basal cell carcinomas spread aggressively, and due to the lack of sufficient cutaneous tissue, technical difficulties may occur in closing the skin, resulting in more conservative margins for the excision.
Existing literature describes a variety of therapeutic approaches for treating basal cell carcinomas, with surgical excision characterised as a particularly effective treatment for initial lesions.[17] According to our research, the recurrence rate after full excision is 21%. The size of the peripheral and deep surgical margins should be correlated with the risk of subclinical tumour expansions to get the best surgical outcomes. Griffiths et al.[18] described in their study that the clearance of deep margins is in the range of 0.1mm and 9.9mm. Excision through subcutaneous fat is generally recommended but this depends on the local anatomy and the site of the lesion. One of the most important requirements during the management of any malignancy, including BCC, is to obtain a clear surgical resection margin. In our study, out of the 85 patients, 44 patients had tumour resection margins of less than 5 mm on final histopathology and 41 patients had tumour resection margins of more than 5 mm on final histopathology. Currently, guidelines recommend a resection margin of 4 mm for small, well-defined basal cell carcinomas, as this has shown to achieve a complete resection rate of approximately 95%.[19]
In our analysis, most patients were treated with excision and primary closure (73.0%; n = 62) followed by excision and reconstruction with local flap (22.4%; n = 19). In addition, the ears, nose and eyelids were found to be the areas where the edges were most affected. This could be because Mohs microsurgery cannot be performed in most plastic surgery facilities, and because anatomical landmarks are important in these regions, surgeons tend to adopt a less aggressive approach in removing tumours. For cases with marginal involvement, patients are referred for radiotherapy and the re-excision is mainly done when the site is mostly closed.
Conclusion
Basal cell carcinoma is growing more widespread in our society, and this study found a substantial number of BCCs in the head and neck area. Assessing patients, considering epidemiology, achieving clear surgical margins to reduce the recurrence rate and incentivising patients for follow up care will improve patient survival.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Review Committee (ERC) of the Aga Khan University Hospital (AKUH), Karachi. The IRB number is 2020-3671-10229
Informed consent
All subjects gave their informed consent for inclusion before they participated in the study.
Credit author statement
AAU: Conception and Design, Acquisition of Data, Analysis and Interpretation of Data.
MHD: Acquisition of Data, Analysis and Interpretation of Data.
HK: Analysis and Interpretation of Data and Drafting of Article.
MOA: Analysis and Interpretation of Data and Drafting of Article.
MFR: Conception and Design and Final Approval.
Data availability
Data is available on request.
Use of artificial intelligence
Artificial Intelligence was not used in any way for this manuscript.