
Abstract
Introduction:
Antiphospholipid syndrome (APS) is typified by the development of antiphospholipid antibodies (aPL) that are persistently positive with the clinical manifestation of thromboembolic problems and pregnancy morbidity. The identification of aPL, specifically lupus anticoagulant (LAC), anticardiolipin (aCL) and antibeta2-glycoprotein I antibodies (aβ2GPI) IgG or IgM, is necessary for the laboratory diagnosis of APS. Also, the diagnostic and risk stratification value of other aPL, known as ‘non-criteria aPL’, has gained importance in recent years. The non-criteria aPL, the antiphosphatidylserine-prothrombin (aPS/PT) antibodies and antibodies against the domain I of beta2-glycoprotein (aDI) have shown relevance in thrombotic events and pregnancy complications.
Material and Methods:
This was a prospective observational study done on 136 patients with APS profiles, correlating LA and antiphosphatidyl serine/PT complex. Patients on anticoagulants and those who lost to follow-up were excluded.
Results:
Of the 118 patients who did not have LA, 96.6% (114) had an IgG result of ≤30 (negative), while 3.4% (4) had a result of >30 (positive). Among the 18 patients with LA, 72.2% (13) had a positive result of IgG >30, while 27.8% (5) had a negative result of <=30, indicating a negative predictive value. Similarly, of the 118 patients without LA, 89.8% (106) had an IgM result of <=30 (negative), and 10.2% (12) had a result of >30 (positive). Among the 18 patients with LA, 38.9% (7) had a positive result of IgG >30, while 61.1% (11) had a negative result of <=30, indicating a negative predictive value.
Conclusion:
Our study showed a statistically significant correlation between LA and aPS/PT complex in patients with arterial thrombotic history. There was a significant association between IgG and LA with a P value of < .001 and between IgM and LA with a P value of < .004.
Keywords
Introduction
The autoimmune condition known as antiphospholipid syndrome (APS) is typified by the development of antiphospholipid antibodies (aPL) that are persistently positive along with the clinical manifestation of thromboembolic problems and pregnancy morbidity.[1-5] The identification of aPL, specifically lupus anticoagulant (LAC), anticardiolipin (aCL) and antibeta2-glycoprotein I antibodies (aβ2GPI) IgG or IgM, is necessary for the laboratory diagnosis of APS.[6-9] The laboratory measures are now frequently employed as diagnostic criteria, even though the Sydney criteria were originally meant to be categorisation criteria.[10] However, the diagnostic and risk stratification value of other aPL, known as ‘non-criteria aPL’, has gained importance in recent years.[1,11]
Among these non-criteria aPL, the antiphosphatidylserine-prothrombin (aPS/PT) antibodies and antibodies against the domain I of beta2-glycoprotein (aDI) have shown relevance in thrombotic events and pregnancy complications.[12-14] Recent research has indicated that patients who have triple positive (LA, aCL and aβ2GPI) are most vulnerable to obstetric problems as well as venous and arterial thrombosis.[15,16]
The interpretation of results requires considering the antibody profiles, as combined positivity for LA, aCL and aβ2GPI antibodies is associated with a high risk of thrombotic events and pregnancy complications.[17,18] Non-criteria aPL, such as aDI and aPS/PT antibodies, can provide additional information for risk stratification in APS patients.[19-21] Numerous investigations have demonstrated that patients may exhibit APS-like clinical characteristics in a significant number of instances, although their aPL titres may be temporarily positive or consistently negative. Those cases, by definition, are called seronegative APS (SN-APS). LA is thought to be the primary risk factor for thrombosis in individuals with aPL (LA).[22] In individuals with LA, the development of a thrombotic episode is linked to increased mortality. Thus, it may be possible to increase survival in LA positives by preventing thromboembolic events.[23]
However, the determination of LA is impaired by the presence of anticoagulant therapy. Still, aPS/PT is the major determinant of LA activity and might substitute LA assays in those indeterminate cases.[24] Classical APLs for APS are either detected by coagulation tests or by an enzyme-linked immunosorbent assay (ELISA).[3,25,26] Recently, it was reported that aPS/PT was found in approximately half of these SN-APS patients, acting as a reliable laboratory biomarker for identifying APS individuals who do not have traditional APLs.[27,28] Assays incorporating PS/PT rather than PT alone for LA activity may be preferable in patients on oral anticoagulation, where it is difficult to test for LA activity. This is because several studies have suggested that PS/PT complex, and not PT alone, is the target of LA activity.[29-31] One simple laboratory test that can help with a more accurate and thorough diagnosis of APS patients is IgG aPS/PT detection.[32]
In conclusion, the laboratory diagnosis of APS is complex, and the detection of aPL is crucial.[33] While the current classification criteria focus on LA, aCL and aβ2GPI antibodies, the inclusion of non-criteria aPL, such as aDI and aPS/PT antibodies, can enhance risk stratification.[7,8,13] Harmonisation of laboratory methods and ongoing research are needed to improve the diagnosis and management of APS.[34-37]
Aims and Objectives
To study the correlation of LA and antiphosphatidyl serine/PT complex along with their clinical significance.
Materials and Methods
This was a prospective observational study done on 136 patients with APS profiles in a quaternary care hospital, from January 2023 to March 2024. Patients on anticoagulants and those who lost to follow-up were excluded. The clinical data and anticoagulant history of patients were recorded from requisition forms and electronic medical records.
Methodology
LA in human plasma is detected by diluted Russell’s viper venom time.
Type of sample: Citrated plasma.
Carefully mix 1-part sodium citrate solution (3.2%) with nine parts venous blood, avoiding the formation of foam.
Centrifuge whole blood at 3500 rpm for 15 minutes to prepare platelet-poor plasma.
Separated plasma should be stored at 2°C-8°C and tested within four hours of collection.
If samples are to be frozen before testing, the plasma must be double-spun to remove platelets prior to freezing, as these can shorten the LA1 screening reagent clotting time.
An abnormal diluted Russell viper venom time (dRVVT screen ratio > = 1.2) may suggest LA. However, other possibilities include congenital/acquired deficiencies or dysfunction of factors I(fibrinogen), II, V or X. If the screen ratio is > = 1.2, a second test called a confirmatory test is done. In the confirmatory test, excess phospholipid is added to neutralise any remaining LA. The ratio of screening and confirmatory test (normalised ratio) is then calculated and interpreted as weak, moderate or strong LA.[38]
Normalised ratio criteria:
1.2–1.5 weak LA 1.6–2.0 moderate LA >2 strong LA
aPS/PT complex antibody (IgG and IgM) is determined by ELISA.
Interpretation of results: The sample can then be classified as negative or positive, as given below:
Negative ≤30 Positive >30
Data Management and Statistical Analysis
The statistical analysis was conducted by the use of SPSS (IBM, 28.0).
Descriptive statistics were presented as frequency (percentage) and mean ± SD for categorical and continuous factors.
The association between two independent categorical factors was established through Chi-square/Fisher’s exact test.
P value of less than .05 is considered to be statistically significant.
Observations and Results
Of the data presented in Table 1, 63 patients (46.3%) were male, while the remaining (53.7%) were female. The age range of these patients is also sufficiently distributed, with the youngest being 14 years old and the oldest being 86. The average age of the patients was 43.6 years, indicating a diverse group.
Demographic factors
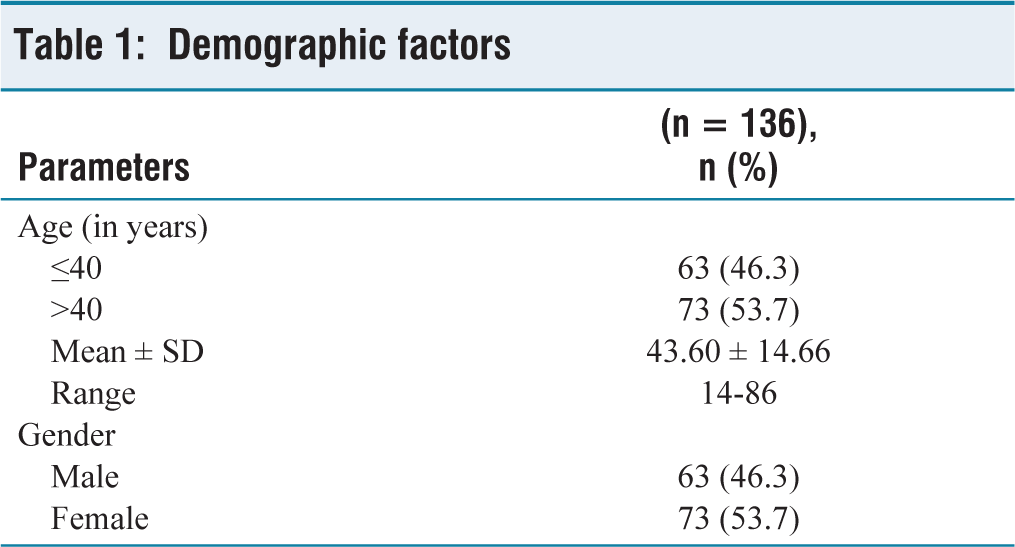
Table 2 presents data based on reports of 136 patients, of whom 118 (86.8%) did not report detection of LAC, while 18 (13.2%) did.
Clinical factors
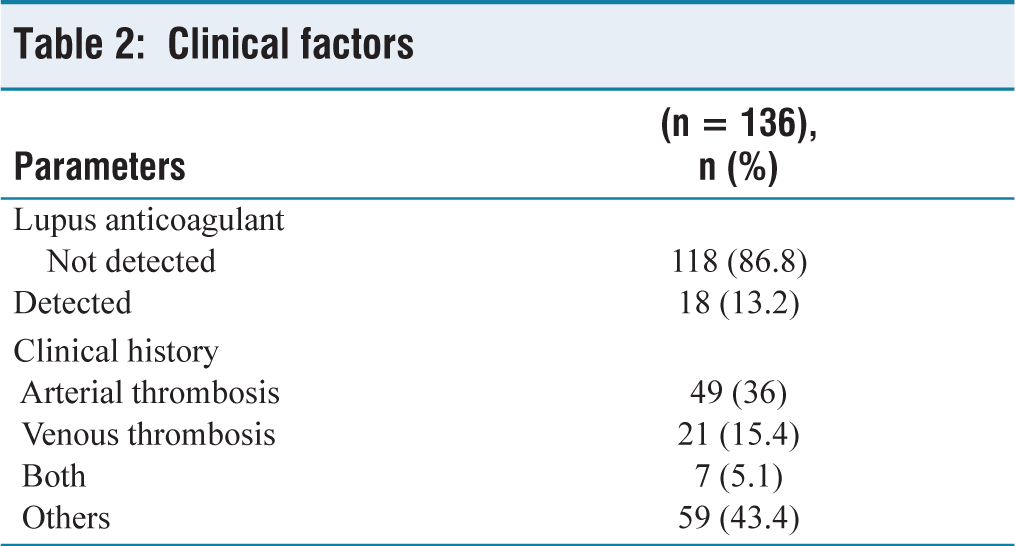
Among the patients without LAC, 49 (36%) had a history of arterial thrombosis, 21 (15.4%) had a history of venous thrombosis, 7 (5.1%) had a history of both arterial and venous thrombosis, and 59 (43.4%) were classified as ‘other’, where patients did not present with a history of thrombosis. Of the 18 patients who tested positive for LAC, 12 (66.7%) had a history of arterial thrombosis, 5 (27.8%) had a history of venous thrombosis, and 1 (5.6%) had a history of both arterial and venous thrombosis. None were classified as ‘other’.
It provides insights into the prevalence of thrombotic events in patients with and without LAC and highlights the importance of further investigation into the relationship between LAC and thrombotic events.
Table 3 shows that of the 118 patients who did not have LA, 96.6% (114) had an IgG result of ≤ 30 (negative), while 3.4% (4) had a result of >30 (positive). Among the 18 patients with LA, 72.2% (13) had a positive result of IgG >30, while 27.8% (5) had a negative result of <= 30, indicating a negative predictive value. Similarly, of the 118 patients without LA, 89.8% (106) had an IgM result of <= 30 (negative), and 10.2% (12) had a result of >30 (positive). Among the 18 patients with LA, 38.9% (7) had a positive result of IgG > 30, while 61.1% (11) had a negative result of <= 30, indicating a negative predictive value. Based on the data analysed, there was a significant association between IgG and LA with a P value of < .001 and between IgM and LA with a P value of < .004.
Association between lupus anticoagulant and aPS/prothrombin complex
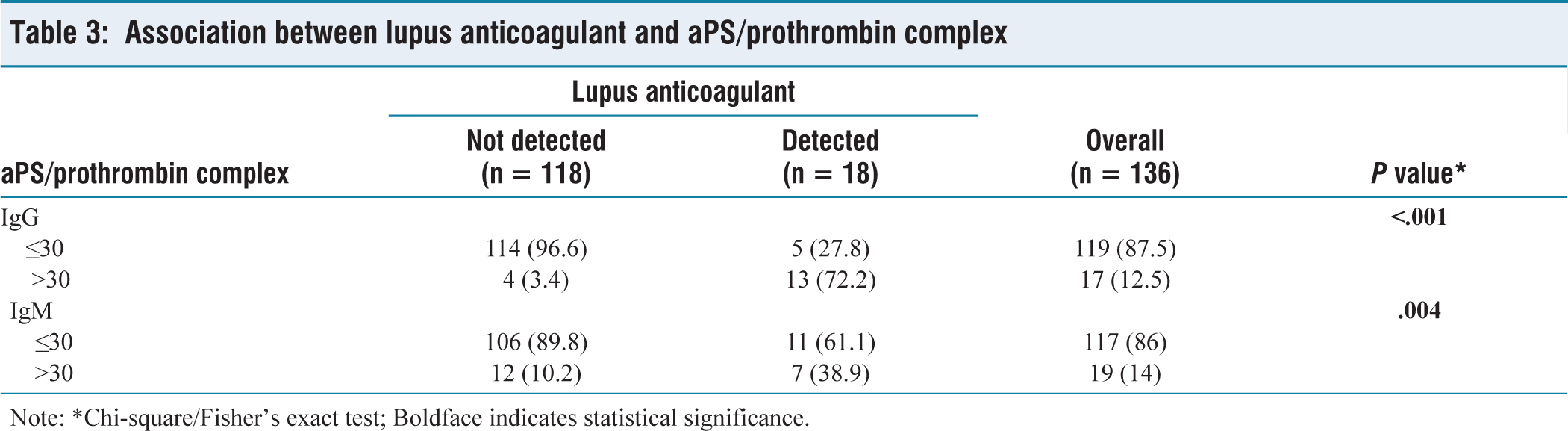
Table 4 presents the association between LA and aPS/PT complex based on the history of thrombosis. During the evaluation of the thrombotic history, results indicated that in cases of arterial thrombosis among 49 patients, all 48 (100%) patients without LA showed IgG <= 30, and only one (100%) patient with LA had IgG > 30, leading to a significant P value of < .020. Similarly, among 21 patients with venous thrombosis, 18 patients were without LA. Out of those 18, 16 patients (88.9%) had IgG <= 30, and 2 (11.1%) patients had IgG > 30. In contrast, among the three patients with LA, two patients (66.7%) had IgG <= 30, and a single patient (33.3%) showed IgG > 30. In seven patients with both arterial and venous, all six patients without LA had IgG <= 30, and one patient with LA also had IgG <= 30. None of them showed a positive IgG (> 30). Furthermore, among 59 patients with other histories, 46 patients did not have LA, and 13 had. Out of those 46, 44 patients (95.7%) had IgG <= 30, and only two patients (4.3%) had IgG > 30. In contrast, out of 13 patients with LA, two patients (15.4%) had IgG <= 30, and 11 patients (84.6%) had IgG > 30, leading to a significant P value of < .001.
Association between Lupus anticoagulant and aPS/Prothrombin complex along with clinical factors
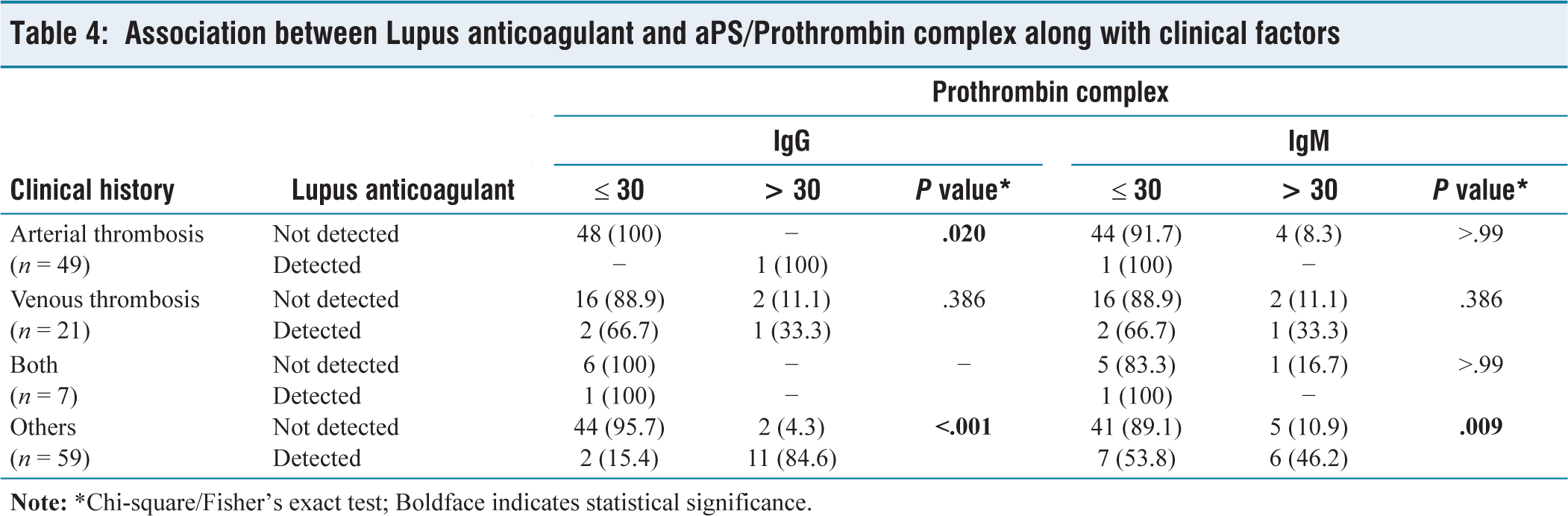
Regarding IgM, during the evaluation of the thrombotic history in cases of arterial thrombosis among 49 patients, out of 48 patients without LA, 44 patients (91.7%) had IgM <=30, and 4 (8.3%) patients showed IgM > 30. Only one patient with LA showed an IgM of <= 30. Similarly, among 21 patients with venous thrombosis, 18 patients were without LA. Out of those 18, 16 patients (88.9%) had IgM <= 30, and 2 (11.1%) patients had IgM>30. In contrast, among the three patients with LA, two patients (66.7%) had IgM <= 30, and a single patient (33.3%) showed IgM > 30. In seven patients with both arterial and venous, all six patients without LA had IgM <= 30, and one patient with LA had IgM>30. A single patient who was detected with LA was also IgM <= 30. Moreover, among 59 patients with other histories, 46 patients did not have LA, and 13 had. Out of those 46, 41 patients (89.1%) had IgM <= 30, and only 5 (10.9%) had IgM>30. In contrast, out of 13 patients with LA, 7 patients (53.8%) had IgM <= 30, and six patients (46.2%) had IgM > 30, leading to a significant P value of < .009.
Discussion
aPL are a diverse and significant class of autoantibodies that interact with cell-associated phospholipids and phospholipid-binding proteins, including PT and beta-2-glycoprotein I (β2GPI), to activate endothelial cells, platelets and neutrophils.[39-43] APS stands for antiphospholipid syndrome, an acquired thrombotic inflammatory illness characterised by maternal difficulties and chronically circulating aPL, as well as arterial, venous and microvascular thrombotic events.[40] According to the current APS categorisation criteria, solid-phase assays (aCL IgG/IgM, antiβ2GPI [aβ2GPI] IgG/IgM) or the LA functional assay must consistently demonstrate aberrant test results (over at least 12 weeks).[44,45] The traditional coagulation tests, known as the aPTT, have historically been used to identify LA when it was (unintentionally) discovered that people who were generally healthy and did not exhibit any coagulation factor deficiencies had longer pre-surgical screens.[46] In our study, there was a significant association between IgG and lupus anticoagulant with a P value of < .001 and between IgM and LA with a P value of < .004, aligning with the study by Žigon et al. and Radin et al. which showed that LA-positive patients had only high titres of aPS/PT IgG/IgM.[47,48]
Similar to our findings, Tonutti et al. study population consisted of 71.5 % females, 53 ± 15 years, and the study was conducted for one year. In total, 49/421 (11.6%) instances had aPS/PT IgM positive (i.e., 30 U/ml) and/or IgG frankly positive (40 U/ml) antibodies. Of the individuals who tested positive for LA, 56.1% had positive results for aPS/PT, and 31.7% had positive results for aCL and/or aβ2GPI. Additionally, they noticed that in individuals who tested positive for LA, aPS/PT antibodies had a significantly higher sensitivity (55.8% vs. 15.4%) than aPT antibodies. These findings correlate with our study.[1]
Regarding the association of LA and aPS/PT complex based on clinical history, during our evaluation of the thrombotic history, we found that out of 13 patients with LA, two patients (15.4%) had IgM<=30, and 11 patients (84.6%) had IgG > 30, leading to a significant P value of < .001and regarding IgM, seven patients (53.8%) had IgM <=30, and six patients (46.2%) had IgM >30, leading to a significant P value of < .009. This finding is similar to the study by Pontara et al. and Vandevelde et al.[49,50] This is similar to the study by Pontara et al. who found a strong link (r = 0.78, P < .0001) between aPL (PT) and LAC potency in 83 participants, including carriers, patients with APS, and controls.[49] Vandevelde et al. in a study of 757 patients, those with triple positive APS test results had higher levels of aPS/PT antibodies, which strongly predicted thrombotic APS (TAPS). However, this association was only independent when adjusting for aCL/aβ2GPI, but not when considering LAC.
Limitations of the Study
No follow-up was conducted regarding the treatment received and outcome.
Detailed clinical history could not be obtained as most of them are sample patient referral cases.
A sample size of a larger number would have given a better insight into delineating the correlation.
Conclusion
LA and IgG aPS/PT showed a more significant correlation when compared to IgM aPS/PT complex.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
This study was approved by the Institutional Ethical Committee under approval number AMH-DNB-005/01-23.
Informed consent
Consent was not applicable, as this is a review article compiled from various research articles and guidelines and not from patients directly.
Credit author statement
Study designed, conducted and manuscript written by Dr Githa.
Study conceptualized, guided and manuscript reviewed and revised by Coauthor Dr Mamta Soni.
Data availability
Available on request.
Use of artificial intelligence
The use of artificial intelligence is not relevant to this article, as it does not involve AI technologies or methodologies in its analysis or conclusions.