
Abstract
Objectives:
Acute colonic pseudo-obstruction is a massive colonic dilation with signs and symptoms of colonic obstruction, but without a mechanical cause.
Methodology:
A 73-year-old hypertensive male on clonidine therapy developed spontaneous left basal ganglia haemorrhage with interventricular haemorrhage. While undergoing neurological treatment patient developed abdominal distension and constipation during hospital stay. All investigations done lead to the diagnosis of Acute colonic pseudo-obstruction (ACPO) (Ogilvie Syndrome).
Results:
Clonidine was suspected cause of Acute colonic pseudo-obstruction (ACPO). Hence clonidine was stopped and patient gradually improved.
Introduction
When there is no mechanical blockage, a rare syndrome known as acute colonic pseudo-obstruction (ACPO) manifests as acute colonic dilatation. Sir William Ogilvie initially reported it in 1948 in two individuals who had pre-vertebral ganglia malignant infiltration.[1]
ACPO usually occurs in hospitalised patients with severe illness or trauma, or following general, orthopaedic, neurosurgical, gynaecological or other surgical procedures, with an estimated incidence of 100 cases per 1,00,000 admissions and a mortality rate of 8%.[2,3] Colonic ischaemia or perforation occurs in up to 15%, and is associated with an estimated 40% mortality.[4-6]
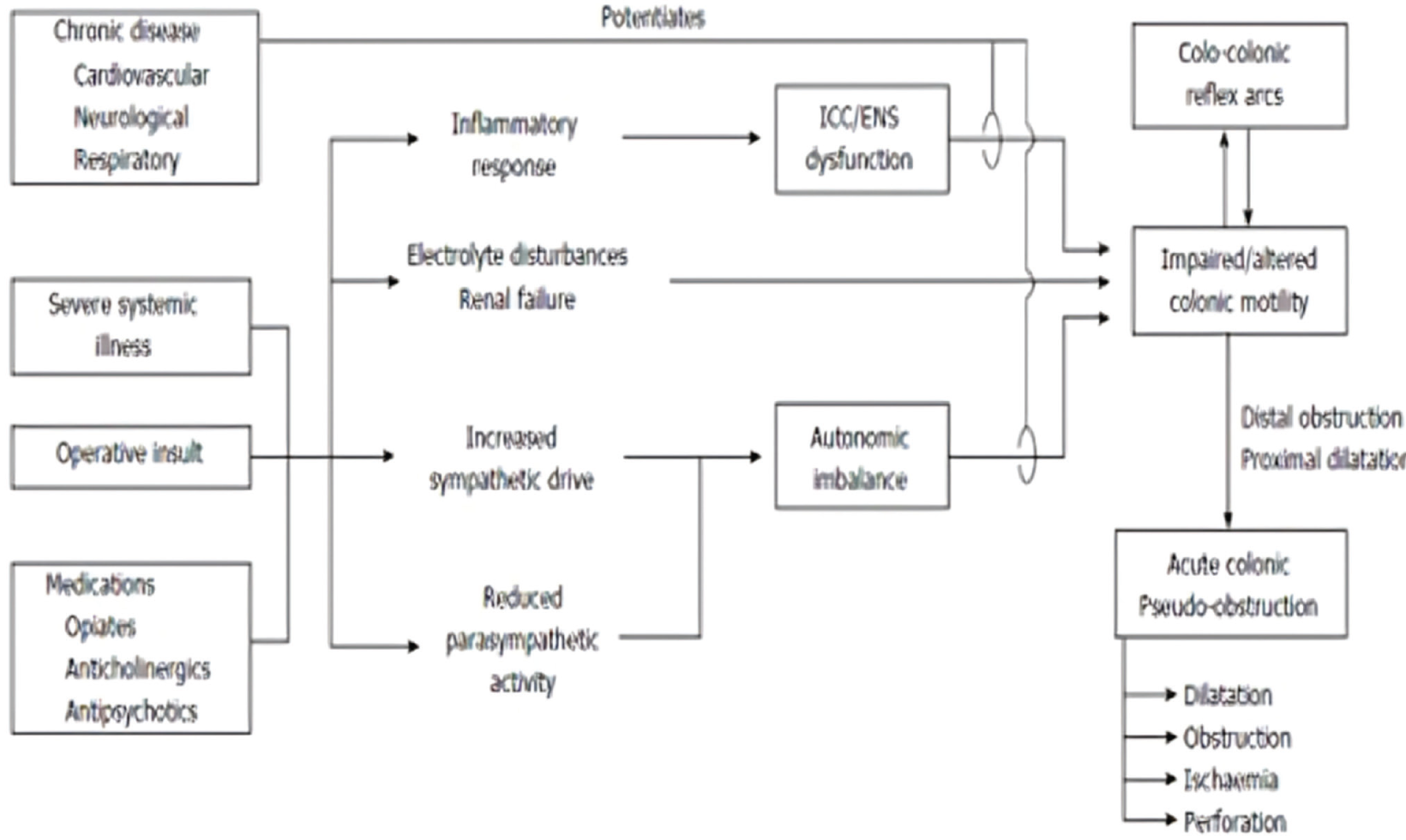
Although little is known about the pathogenesis of ACPO, an imbalance in colonic autonomic innervation is the most widely accepted theory.[2,4] Pacemaker signals from Cajal interstitial cells control colonic motility, which is then modulated by the autonomic nervous system and colonic arc reflex. ACPO could occur if any of those components are disturbed. Similarly, an atonic region in the colon with proximal dilatation may result from autonomic imbalance accompanied by either decreased parasympathetic regulation or greater sympathetic overflow. Sympathetic agonists and parasympathetic antagonists exhibit this imbalance.[7,8]
The development of ACPO has been linked to pathophysiological variables. ENS stands for enteric nervous system; ICC stands for interstitial cells of Cajal.
At relatively high doses of 0.3 mg BID, α2 receptor agonist, clonidine, reduces intestinal fluid and electrolyte secretion,[9] and inhibits gastric and colonic tone, phasic contractility and sensation in the rectum and colon in response to balloon distension in healthy humans.[10-12]
Case Report
The 73-year-old male was admitted to the hospital with chief complaints of sudden onset of right upper and lower limb weakness with aphasia. The patient is a known case of hypertension and was on treatment for the same (ongoing treatment Tab Telmisartan 40 mg OD, Tab Amlodipine 5 mg BD and Tab Clonidine [0.2 mg QDS]). On neuroimaging studies, acute intracerebral haemorrhage in the left basal ganglia with oedema was seen. In view of low Glasgow Coma (E1M5VT), scale patient was intubated and mechanically ventilated. The patient was treated with antioedema measures, antibiotics (as the patient was put on mechanical ventilation and central line insertion and Foley’s catheter insertion was done so single prophylactic antibiotic was started), antihypertensives, antiepileptics and antipyretics (given on as and when required basis). Gradually neurological condition of the patient improved and weaning was started. A tracheostomy was done on day 8 of his admission in view of the long duration of ventilation.
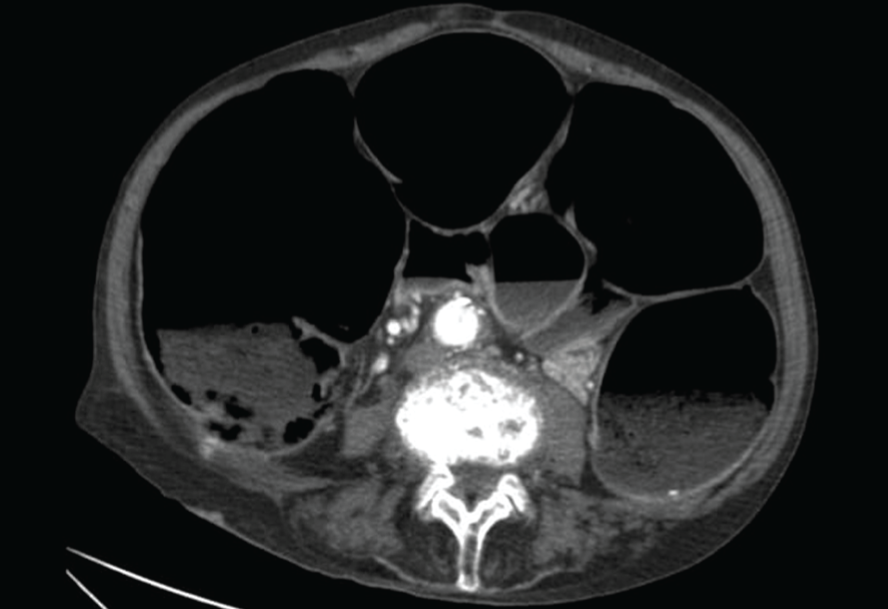
On day 10 of his admission, patient developed abdominal distension and constipation. Abdominal girth was increased from baseline. Rectal examination was done and rectum was empty with ballooning. X-ray of the abdomen and ultrasonography (bedside ultrasonography done in ICU so picture not available) of abdomen was done which showed dilated fluid-filled and gas-filled small bowel loops with a maximum size of 5.1 cm. The small bowel wall appears normal. CT scan of abdomen was done which showed significant dilatation of the large bowel from caecum to rectum and dilation was predominantly gaseous with mild faecal matter. Small bowel loops were normal suggestive of functional large bowel obstruction (pseudo-obstruction) likely.
The patient was treated with rectal enema[13] and rectal tube insertion (rectal enema was given as per advice by a gastro physician and gastro surgeon along with repeated per rectal tube insertion) and neostigmine infusion. Abdominal girth was monitored but no significant improvement was seen. A colonoscopy was done which showed significant dilatation throughout the colon and hence colonic decompression was done. Ongoing treatment was reviewed and clonidine was suspected as a cause of ACPO. Hence, clonidine was tapered and gradually stopped. The patient gradually improved after the withdrawal of clonidine. Abdominal distension was decreased. Gradually patient was decannulated and discharged.
Discussion
Autonomic imbalance is likely to play a key role in the development of ACPO.
After three years of haemodialysis for chronic renal failure, a 26-year-old male patient underwent a renal transplant in 1976. He had persistent hypertension after the procedure, which was eventually managed with a combination of medications (hydralazine 400 mg/day, propranolol 400 mg/day, methyldopa 2 g/day, frusemide 40 mg/day and clonidine 2 mg/day). This patient had pseudo-obstruction caused by clonidine. The patient experienced constipation and abdominal distension in the third- and fourth-weeks following transplantation, which were refractory to laxatives and mineral oil. Only a lot of soft, thick faeces were found during the colonoscopy. The distension was momentarily reduced by colonic lavage, but the constipation persisted. The patient experienced nausea and vomiting 30 days after the transplant. In addition to radiographic indications of gross intestinal distension with air-fluid levels, there were high-pitched, tinkling bowel sounds. After stopping clonidine, the gastrointestinal symptoms went away and bowel movements reverted to normal in 36 hours, even if other antihypertensive medications were still being used.[14]
Two cases of severe colonic pseudo-obstruction (Ogilvie’s Syndrome) following high doses of clonidine intravenous infusions for delirium tremens were reported by D S Stieger et al. in 1997. In both cases, pseudo-colonic blockage was diagnosed via emergency laparotomy. We suggest that the formation of colonic pseudo-obstruction was caused by clonidine, either alone or in conjunction with other factors, because it had a significant parasympatholytic impact on the large bowel of these patients.[15]
An in vitro investigation conducted on guinea pigs in 2002 showed that peristaltic motor activity was inhibited when clonidine (10 nM-100 µM) was added to the organ bath.[16]
According to a 2023 article, using opioids can have a number of negative side effects, including sleepiness, pruritus, constipation (which can also result in colonic pseudo-obstruction),[17] nausea, respiratory depression, tolerance and dependence.
Similarly, in our patient also clonidine was suspected as a cause of ACPO and hence managed accordingly. Our patient drastically improved within 24-48 hours of withdrawal of clonidine. Hence clonidine in high doses is a suspected cause of ACPO.
Conclusion
Colonic pseudo-obstruction can be life-threatening, and if untreated may lead to perforation and a high rate of morbidity and mortality. Early consultation with a gastroenterologist is appropriate to diagnose the suspected cause and the impending agent should be stopped immediately. Patients with large dilations may require pharmacologic, colonoscopic, fluoroscopic or surgical intervention if conservative management fails. Hence, appropriate diagnosis and early therapy are necessary to decrease morbidity and mortality.
Note
This suspected adverse drug reaction was reported to the Pharmacovigilance Centre with Report ID-IN-IPC-300938205. Since withdrawal of the drug leads to improvement in the condition of the patient (positive de challenge) this ADR appears probably related to the drug clonidine as per WHO Causality Assessment Criteria.[18]
X-ray abdomen of patient.
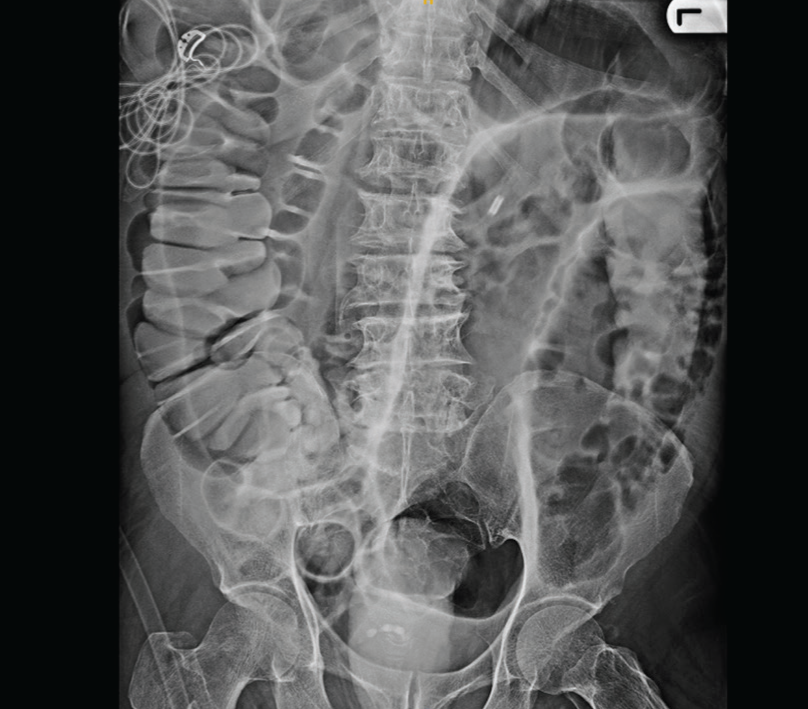
Dilated large bowel loops suggestive of ACPO.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical permission was not applicable for this article, as this is a review article drafted from various research articles and not from patients directly.
Informed consent
Written informed consent was obtained from all participants included in the study.
Credit author statement
Dr Deepak Malhotra contributed in development of idea, manuscript review and editing.
All authors have contributed in manuscript writing and data analysis.
Data availability
Patients case records obtained with permission.
Use of artificial intelligence
The use of artificial intelligence is not relevant to this article, as it does not involve AI technologies or methodologies in its analysis or conclusions.