
Abstract
Background and Aims:
Hypotension after spinal anaesthesia is a frequent problem in obstetric patients. Intra-abdominal volume and abdominal circumference (AC) are correlated. During pregnancy, maternal AC rises and is influenced by the uterus, amniotic fluid, and size of the foetus. Previous studies have demonstrated associations between larger AC and higher abdominal pressure and level of sensory block. Several studies have shown that the risk of hypotension in pre-eclampsia is less after spinal anaesthesia as compared to healthy parturient.
Aims and Objectives:
The aim of the study was to evaluate the relationship between the AC and incidence of hypotension during caesarean under spinal anaesthesia. We also wanted to compare the degree of hypotension post-spinal between pre-eclampsia and non-pre-eclamptic patients.
Patients and Methods:
This observational study was conducted at the Department of Anesthesiology, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, with institutional ethical committee approval and written informed consent from the patients. Group 1 consisted of pre-eclampsia patients, and Group 2 comprised non-pre-eclampsia patients undergoing caesarean section.
Observations and Results:
AC of the patients in both groups showed no difference of statistical significance, but there was a significant statistical difference in the haemodynamics in patients of the two groups.
Conclusion:
We observed a higher incidence of hypotension in a non-pre-eclamptic group, which was statistically significant and not related to variations in AC. This implies that AC has no correlation with post-spinal hypotension.
Introduction
Increasing intra-abdominal pressure in the pregnant woman causes the degree of spinal anaesthesia to rise even when the same amount of anaesthetic is delivered.[1]
Intra-abdominal volume and abdominal circumference (AC) are correlated. During pregnancy, maternal AC rises and is influenced by the uterus, amniotic fluid, and size of the foetus. The inferior vena cava may become compressed as a result of these circumstances.[2]
Pre-eclampsia a disorder distinctive to pregnancy raises maternal and newborn morbidity and mortality rates, Several studies have shown that the risk of hypotension in pre-eclampsia is less after spinal anaesthesia as compared to healthy parturient.[3-5] It has been demonstrated that there is an association between larger AC, higher abdominal pressure[4] and level of sensory block in previous studies.[2,6] Thus, we aim to evaluate the relationship between the AC and incidence of hypotension under spinal anaesthesia in obstetric patients. We also wanted to compare the degree of hypotension post-spinal between pre-eclampsia and non-pre-eclamptic patients.
Material and Methods
This research was conducted at the Department of Anesthesiology, Maharishi Markandeshwar University Ambala, with institutional ethical committee approval and written informed consent from the patients. This observational study was conducted between March 2022 and March 2023, involving two groups of 25 patients each. Group 1 consisted of pre-eclampsia patients, and Group 2 comprised non-pre-eclampsia patients undergoing caesarean section. The study included all term pregnant women aged between 15 and 45 years with ASA 2 and who underwent caesarean section under subarachnoid block. However, patients with high-risk pregnancies, such as placenta previa, abrupt placenta, eclampsia, multiple pregnancies, and cardiovascular co-morbidities, were excluded.
The measurement of AC was taken at the level of the umbilicus in a supine position on the day of surgery by a single observer throughout the study. The spinal anaesthesia was performed using the standard technique by an attending anaesthetist. The spinal anaesthesia was administered using 0.5% hyperbaric bupivacaine in the sitting position, and the doses were adjusted by the anaesthetist performing the procedure. The level of anaesthesia was achieved at T4 dermatomal level by adjusting the operative table and coloading was done using 500 ml crystalloid. The blood pressure and heart rate were obtained at baseline and at 1, 5, 10 and 30 minutes after spinal anaesthesia using a non-invasive technique. The target mean arterial pressure (MAP) of 65 mm Hg was maintained using intravenous mephentermine and a systolic blood pressure of less than 90 mm Hg and MAP less than 65 mm Hg was taken as hypotension.
This study was designed with the primary objective of determining the relationship between AC and hypotension in pregnant females after spinal anaesthesia. The patients were divided into two groups: pre-eclampsia patients and non-pre-eclampsia patients.
Statistical Methods
Data were described in terms of range; mean ± standard deviation (±SD), frequencies (number of cases) and relative frequencies (percentages) as appropriate. To determine whether the data were normally distributed, a Kolmogorov-Smirnov test was used. Comparison of quantitative variables between the study groups was done using the Mann-Whitney U test for independent samples for non-parametric data. For comparing categorical data, Chi-square (χ2) test was performed and Fisher exact test was used when the expected frequency was less than 5. A probability value (P value) less than .05 was considered statistically significant. All statistical calculations were done using (Statistical Package for the Social Science) SPSS 21.0 version (SPSS Inc., Chicago, IL, USA) statistical program for Microsoft Windows.
Observation and Result
A total of 50 females were included in this study. They were divided into two groups containing equal parturients. Group A had pre-eclamptic patients and Group B had non-pre-eclamptic patients. Group A and Group B patients were given spinal anaesthesia.
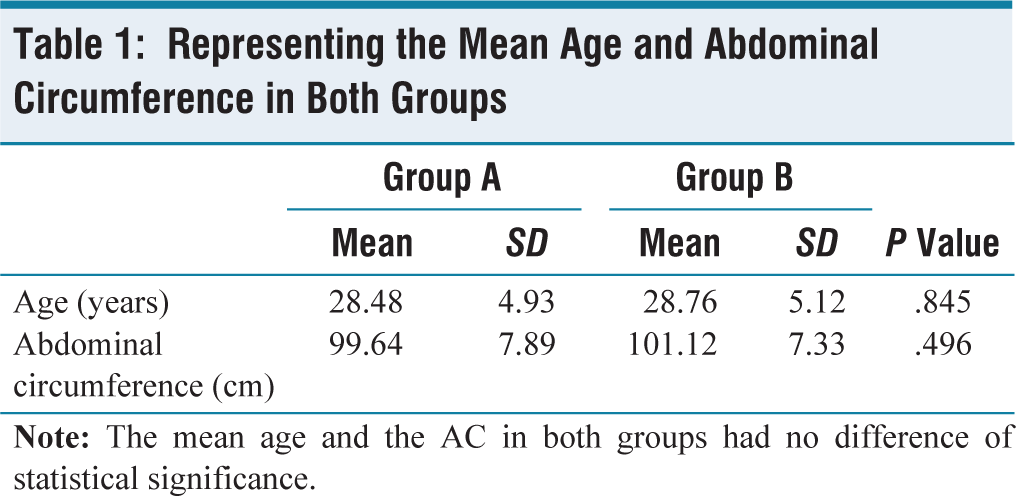
There was no significant difference in the mean age of the patients of the two groups. AC of the patients in both groups showed no difference in statistical significance [Table 1].
Representing the Mean Age and Abdominal Circumference in Both Groups
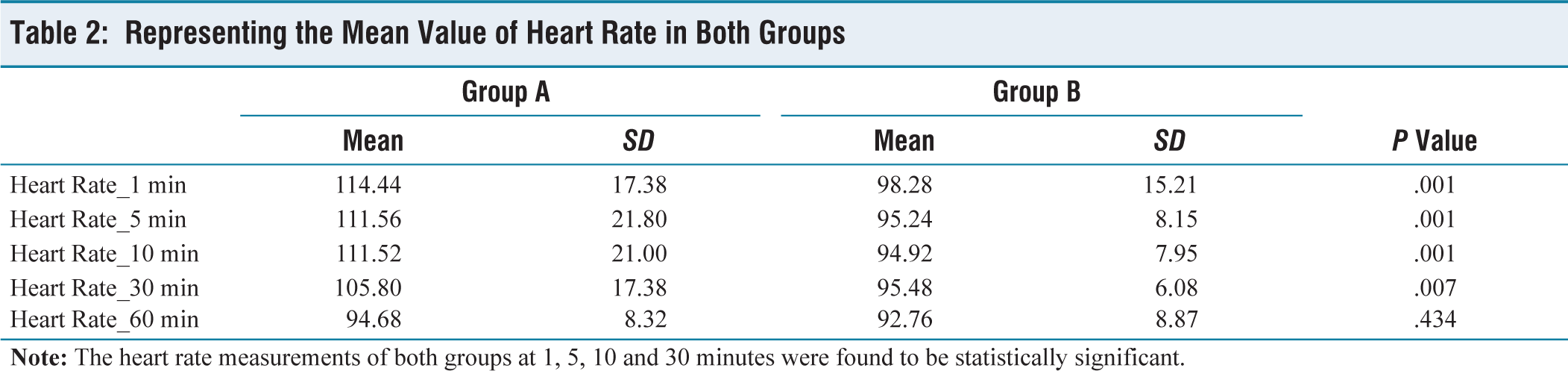
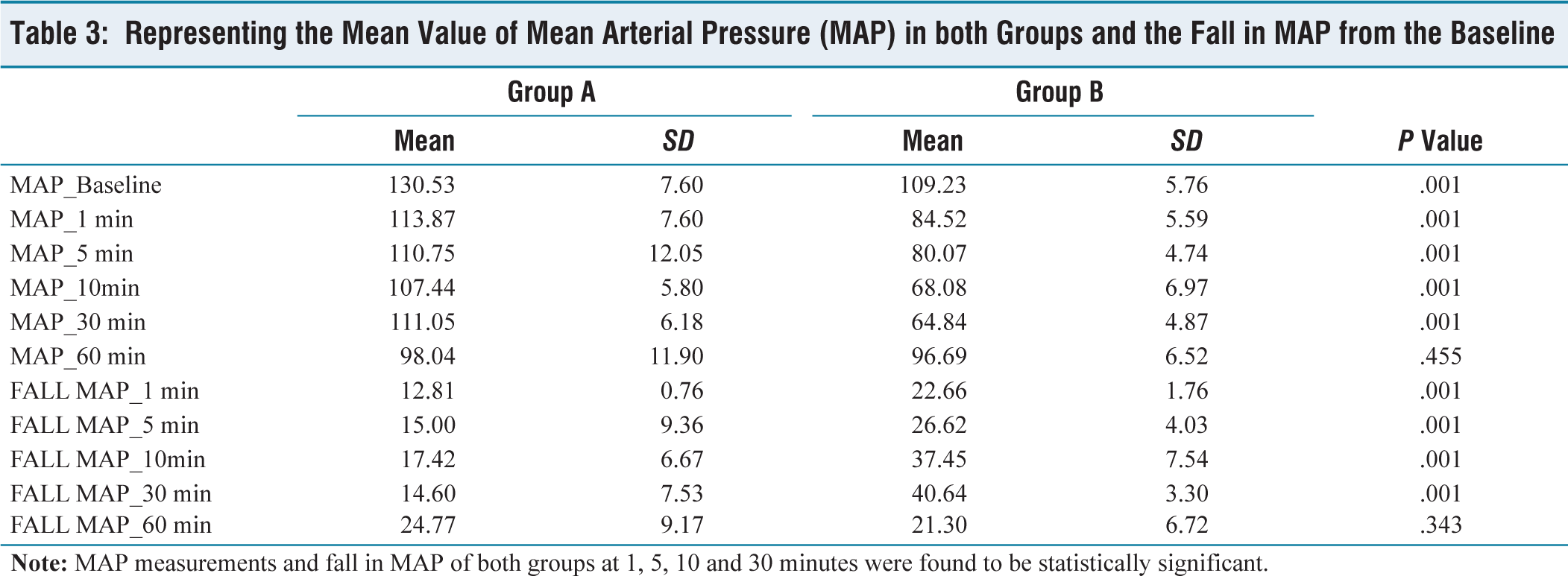
There was a significant statistical difference in the haemodynamics at different time intervals in patients of the two groups [Tables 2 and 3].
Representing the Mean Value of Heart Rate in Both Groups
Representing the Mean Value of Mean Arterial Pressure (MAP) in both Groups and the Fall in MAP from the Baseline
Discussion
The subarachnoid block is the most common mode of anaesthesia for caesarean section delivery and is associated with hypotension in 64%-100% of patients.[4] Of these patients, women with pre-eclampsia have been considered to be more at risk for severe hypotension.[7-11] With recent research, a relationship between AC and changes in MAP after spinal anaesthesia is being studied. In our study, we investigated the effect of AC on the degree of hypotension following spinal anaesthesia in pre-eclampsia and non-pre-eclampsia patients.
The comparison between AC in patients with pre-eclampsia and non-pre-eclampsia patients had no significant difference, which was a mean of 99.64 in Group A and in Group B was 101.12 with the P value of .4 which is non-significant.
According to the data collected the heart rate measurement of both groups at 1, 5, 10 and 30 minutes was higher in pre-eclampsia group and was statistically significant. In our study, the fall in MAP at 1, 5, 10 and 30 minutes in patients with pre-eclampsia had significantly less fall in MAP as compared to non-pre-eclamptic patients. Our figures regarding haemodynamics were similar to what was seen by Alanas Sivevski et al.[12] They studied a total of 78 patients and concluded the incidence and severity of spinal induced hypotension in patients undergoing and section was less in pre-eclamptic than in healthy parturient. Another prospective study by Aya et al. found that pre-eclamptic patients had a significantly lower risk of hypotension than healthy-term parturients.[13] These findings were in accordance with what was found in our study.
The lower incidence of hypotension post-spinal anaesthesia in pre-eclampsia patients might be due is the fact that vasodilator system in these patients has an altered response which maintains high vascular tone, which is independent of spinal-induced sympathetic blockade.[14] Another reason is increased circulations of vasopressor factors and increased sensitivity of small resistant vessels to the exogenous vasopressor stimulation.[15]
In our study, the AC was similar in both groups, however, the degree of hypotension post-spinal block was higher in non-pre-eclamptic patients, which was independent of any effect of AC. Our results were the same as Thomard et al. who also studied the relationship between AC and incidence of hypotension and concluded that there was no relationship between hypotension and AC.[16]
Conclusion
We observed that the incidence of hypotension in the non-pre-eclamptic group was higher, which was statistically significant and not related to variations in AC. This also implies that AC has no correlation with post-spinal hypotension. These findings have implications for clinical practice, as healthcare providers should consider other risk factors in addition to AC when assessing potential complications during caesarean section.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
IEC 2440.
Informed consent
Informed consent was obtained from all participants involved in the study.
Credit author statement
We hereby state that the manuscript has been read and approved by all the authors. This manuscript represents honest work. The contents have not been published elsewhere. As this was an observational study, it was not registered with Clinical Trials Registry.
Gagandeep: Contributed in acquisition and interpretation of data.
Arvin Preet Kour: Conceptualised and designed the study and supervision of Gagandeep.
Akashdeep Singh: Drafting of the article, revising it critically and final approval of the version to be published with all the modifications.
Jasmeet Kaur: Helped in the proof reading and gave valuable inputs in the article.
Use of artificial intelligence
The use of artificial intelligence is not relevant to this article, as it does not involve AI technologies or methodologies in its analysis or conclusions.
Data Availability
Nil.