
Abstract
Introduction:
Ankylosing spondylitis (AS) is a chronic inflammatory condition primarily affecting the axial spine, commonly associated with extra-articular manifestations such as anterior uveitis (AU). Racial disparities have been observed in the prevalence of AU among AS patients, with African American individuals often experiencing higher frequencies compared to their white counterparts. Moreover, AS is linked with various comorbidities, contributing to increased morbidity and mortality. This study aims to investigate the prevalence of AU and associated comorbidities among AS patients, with a focus on racial differences.
Methods:
This retrospective study utilised data from the 2020 National Inpatient Sample (NIS) database, identifying adult patients with AS admitted to hospitals in the United States. Descriptive statistics were employed to analyse demographic characteristics and comorbidity prevalence. Multivariate analysis assessed the association between AU, race, comorbidities, and inpatient outcomes.
Results:
Our analysis revealed significant racial disparities in the prevalence of AU among AS patients. Patients with AU tended to be younger, with a mean age of 48 years versus a mean age of 60 in patients with AS without AU. Among patients with AS without AU, 82% were Caucasians and African Americans represented 6%. Among patients with AS with AU, Caucasians represented 71% and African Americans represented 18%. In terms of outcomes, patients with a history of AU exhibited similar inpatient mortality rates (less than 1%) compared to those without (3%). Acute kidney injury (AKI) was more prevalent among patients with AU (24%) versus those without (16%) but was not statistically significant. The comorbidities commonly associated with AS include hypertension, both complicated (23%) and uncomplicated (40%), along with diabetes presenting with and without chronic complications at rates of 17% and 11%, respectively.
Conclusion:
Our study underscores the need for further research to elucidate the relationships between AS, AU, and comorbidities, particularly in the context of racial disparities. Improved risk assessment and early detection strategies tailored to the African American population are crucial for facilitating timely diagnosis and targeted treatment interventions for AS. Addressing these disparities and advocating for proactive management approaches can help mitigate healthcare inequities and enhance overall health outcomes for African American AS patients.
Introduction
Ankylosing spondylitis (AS) is characterised by inflammatory arthritis affecting the axial skeleton, notably the sacroiliac joint, peripheral joints, and the entheses. The onset of AS typically occurs in the third decade of life, presenting as progressive back pain and stiffness that limit patients’ physical activity and productivity. AS is classified among seronegative spondyloarthropathies (SpA), a group that includes psoriatic arthritis, reactive arthritis, enteropathic arthritis, and juvenile-onset spondylarthritis. These autoimmune inflammatory diseases lack rheumatoid factor or antinuclear antibody in their serum and share a strong genetic association with human leukocyte antigen (HLA)-B27.[1,2] AS is the most common SpA disease, with a prevalence in the Caucasian population ranging from 0.5% to 1.8%, with a higher prevalence in populations with a higher prevalence of HLA-B27 positivity. Incidence is estimated at 0.49 in Japan compared to 10 in Norway per 100,000 individuals.[3] Despite the strong link between HLA-B27 and AS, only 5% of HLA-B27-positive individuals in the general population develop AS.[4]
There is a growing acknowledgement of the extra-axial manifestations (EAMs) of AS. Frequently observed EAMs include anterior uveitis (AU), psoriasis, inflammatory bowel disease, as well as, heart, lung, skin, bone, and kidney involvement. There is no accurate estimate of the prevalence of AU in AS, but studies, using databases similar to ours, estimate a prevalence of 20%-30% AU in patients with AS.[5] It manifests as acute unilateral pain, photophobia, and blurriness due to inflammation of the anterior part of the eye. Approximately 50% of patients who develop AU are positive for HLA-B27, and it has been linked to a more prolonged disease course in patients with AS.[6] Previous studies show mixed results when comparing AS patients with AU in different racial groups. Some studies have suggested that there is a stronger correlation between AU and AS in Caucasian individuals and that AU is less likely in African Americans with AS.[2] AU in AS patients is associated with higher disease activity, poor functional ability, and advanced physical impairment.[7]
Patients with AS have significantly more comorbidities than matched controls, including asthma, cardiovascular disease, depression, osteoporosis, spinal fractures, and inflammatory bowel disease.[8] Mortality in AS is increased in both male and female patients, with predictors of death including socioeconomic status, general comorbidities, and hip replacement surgery.[9] Twenty-eight percent of patients with AS had comorbidities, with high blood pressure being the most common at 19%, followed by diabetes mellitus at 4%.[10]
Here, we present a retrospective study exploring the comorbidities linked to AS, with a particular focus on how AU impacts clinical outcomes in hospitalised AS patients.
Methods
This retrospective study focused on adult patients admitted to hospitals with comorbid AS within the United States. The primary objective was to evaluate common comorbidities among AS patients and compare outcomes between patients with AS with and without AU. The analysis relied on data extracted from the 2020 National Inpatient Sample (NIS) database, a 20% stratified sample representing US hospitalisations, obtained from the Healthcare Utilisation Project (HCUP). Patient selection was based on the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) coding system, identifying relevant diagnoses for AS (M45 0-9) and AU (H2001, H2002, H201).
Variables of Interest, Study Outcomes, Statistical Analysis
The study primarily examined the demographic characteristics of patients with AS, stratified by the presence or absence of AU. Additionally, the study evaluated in-hospital mortality, length of stay, and the risk of inpatient complications, such as acute kidney injury (AKI), cerebrovascular accident, and acute heart failure. Statistical analysis was conducted using STATA version 17.0.[11] Descriptive statistics expressed data as percentages for categorical variables and mean ± standard deviation for continuous variables. Student’s t-test compared continuous variables, while chi-square tests were utilised for categorical variables. A significance threshold of P < .05 determined statistical significance.
Results
Demographics and Characteristics Among AS Patients with AU
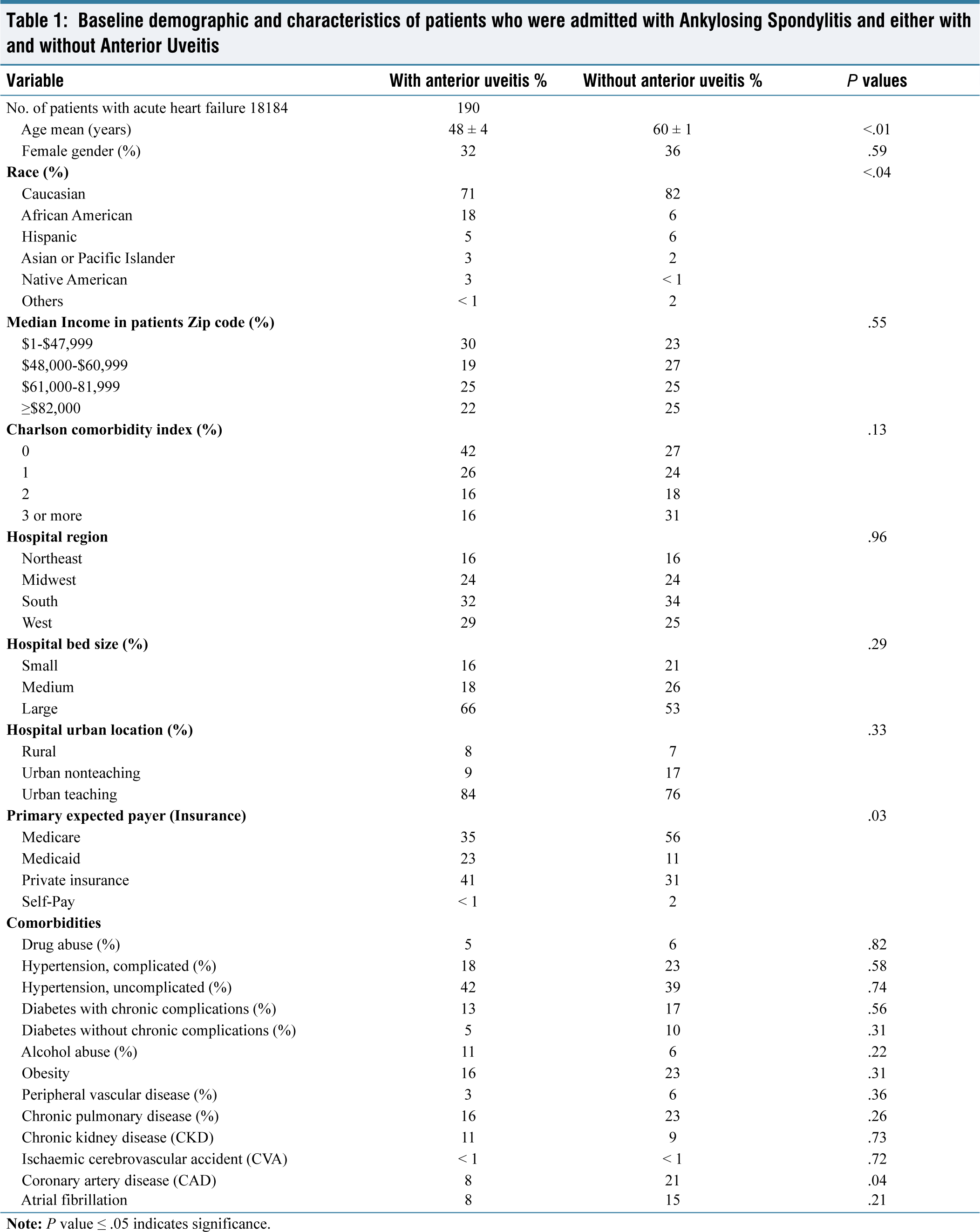
In examining patients admitted with AS and considering their AU status, significant differences in demographics and characteristics were observed. Those with AU tended to be younger, with a mean age of 48 years compared to 60 years for those without. Among patients with AS without AU, Caucasians represented 82% and African Americans represented 6%. Among patients with AS and a history of AU, Caucasians represented 71% and African Americans represented 18%. Thus, African American representation was higher among AS patients with AU (18%) compared to those without (6%) (P = .04).
Moreover, there was a notable difference in insurance coverage, with Medicare more prevalent among those with AU (35%) than those without (56%). The Charlson comorbidity index also demonstrated variations, revealing a higher prevalence of patients with a score of 3 or more among individuals without AU (31%) compared to those with (16%) which can be related to the higher average age in the AS without UA population in our study . Baseline demographics and characteristics of patients who were admitted with ankylosing spondylitis and either with or without anterior uveitis can be seen in Table 1.
Baseline demographic and characteristics of patients who were admitted with Ankylosing Spondylitis and either with and without Anterior Uveitis
Proportion of Comorbidities and Patient Characteristics Among AS Patients
Analysing comorbidities and patient characteristics among AS admissions showed subtle differences between patients with and without AU. Conditions such as hypertension (both complicated and uncomplicated), chronic pulmonary disease, and coronary artery disease exhibited marginal variations.
The comorbidities commonly associated with AS irrespective of AU include hypertension, both complicated (23%) and uncomplicated (40%), along with diabetes presenting with and without chronic complications at rates of 17% and 11%, respectively. Chronic pulmonary disease is prevalent among 23% of patients, while obesity affects a similar proportion at 23%. Additionally, drug abuse, alcohol abuse, and peripheral vascular disease are observed in approximately 6% of individuals with AS.
Outcomes Among AS Patients with and Without AU
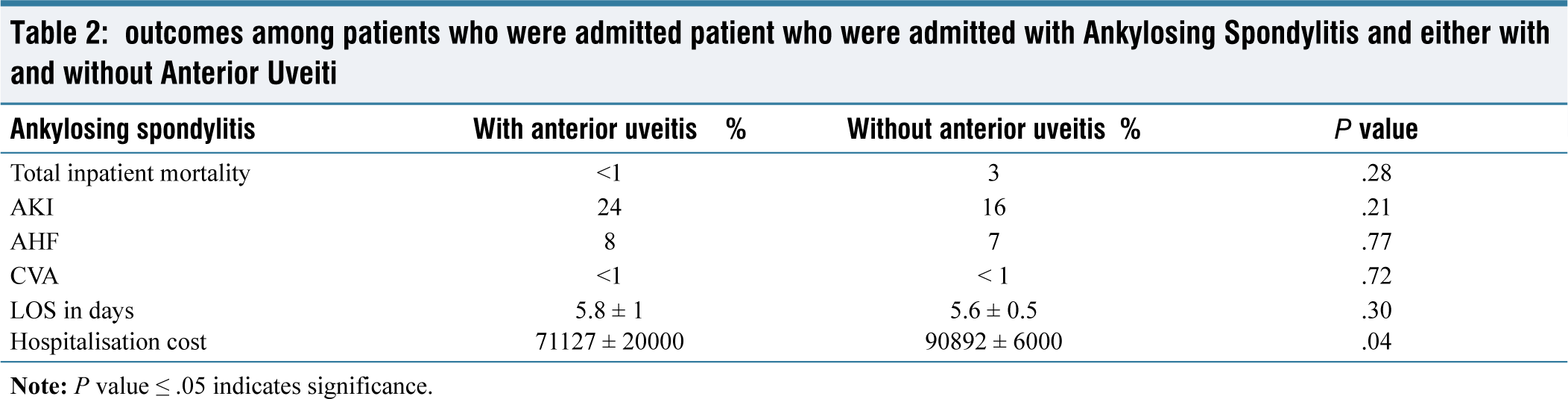
Examining the overall outcomes among AS admissions based on AU status showed that inpatient mortality was similar between those with a history of AU (less than 1%) compared to those without (3%) (P = .28). Similarly, AKI was not statistically different between patients with AS and AU (24%) versus those without AU (16%) (P = .21). Additionally, hospitalisation costs were similar among patients with AU ($71,127 ± $20,000) and those without ($90,892 ± $6,000) (Table 2).
outcomes among patients who were admitted patient who were admitted with Ankylosing Spondylitis and either with and without Anterior Uveiti
Discussion
AS falls under the category of diseases called SpA, characterised by a negative rheumatoid factor and antinuclear antibody. In this large nationwide observational study, our objective was to evaluate associated comorbidities among AS and compare outcomes between patients with AS with and without a history of AU.
The analysis of patients admitted with AS revealed significant disparities in demographics and characteristics based on its association with AU. Patients with AU tended to be younger, with a mean age of 48 years versus a mean age of 60 in patients with AS without AU. Among patients with AS without AU, Caucasians represented 82% and African Americans represented 6%. Among patients with AS with AU, Caucasians represented 71% and African Americans represented 18%.
In terms of outcomes, patients with AU exhibited similar inpatient mortality rates (less than 1%) compared to those without (3%). AKI was more prevalent among patients with AU (24%) versus those without (16%) but was not statistically significant. The comorbidities commonly associated with AS irrespective of AU include hypertension, both complicated (23%) and uncomplicated (40%), along with diabetes presenting with and without chronic complications at rates of 17% and 11%, respectively. Chronic pulmonary disease is prevalent among 23% of patients, while obesity affects a similar proportion also at 23%. Additionally, drug abuse, alcohol abuse, and peripheral vascular disease are observed in approximately 6% of individuals with AS.
The prevalence of AU, a common extra-articular manifestation of AS, has been investigated concerning demographic and clinical factors. A US population-based study revealed that along with AS, increasing age, cigarette smoking, ulcerative colitis, and Crohn’s disease were positively associated with self-reported uveitis, with an adjusted prevalence of 5.4 per 1000 subjects.[12]
Studies have shown mixed results when comparing AS patients with AU in different racial groups. One study comparing disease severity among three ethnic groups found that African Americans with AS patients exhibited greater functional impairment, disease activity, and radiographic severity compared to white and Latino counterparts, along with a higher frequency of AU.[13] Another study by Singh et al. revealed that a higher percentage of African American patients (7.6%) experience AU compared to Caucasian patients (4%).[5] However, this finding is inconsistent with prior studies conducted at a major teaching hospital in Africa by Chalmers et al., which indicated a lower rate of uveitis in black patients compared to white patients.[6]
Our study demonstrates significant differences in racial distribution with African Americans representing 6% of patients with AS without AU compared to 18% with AS and a history of AU. Meanwhile, Caucasians made up 82% of patients with AS without AU and 71% of patients with AS and a history of AU. These findings underscore racial disparities in AU prevalence among AS patients, with African American individuals also showing higher rates of comorbidities such as hypertension, diabetes, and depression.[5]
In our analysis of comorbidities for patients with AS, we found a higher prevalence of complicated diabetes with (17%) and diabetes without chronic complications (11%), complicated (23%) and uncomplicated (40%) hypertension, chronic pulmonary disease (23%), coronary artery disease (21%) and obesity (23%). In a Turkish cross-sectional study by Garip et al., comorbidities were reported in 28.18% of the patients with AS, including hypertension (20%), lung disease (15.45%), diabetes mellitus (13.64%), and ischaemic heart disease (10%).[14] One US study demonstrated a prevalence of diabetes in AS patients at 17.3% in Caucasians and 27.2% in African Americans, with hypertension prevalence in AS patients to be 22% in Caucasians and 29% in African Americans.[12] In a meta-analysis done by Zhao et al. examining people with axial spondylarthritis, a total of 40 studies were analysed with a combined sample size of 119,427 patients. The most common individual comorbidities were hypertension (pooled prevalence 23%), hyperlipidaemia (17%), and obesity (14%).[15] These studies among others are consistent with our findings and provide insights into the prevalence of comorbidities in AS, highlighting the importance of managing these additional health concerns in patients with AS.
Findings from earlier research suggest a possible link between AS patients who have uveitis and cardiovascular abnormalities, though this connection remains indeterminate. Prior analyses have suggested an increased risk of cardiovascular disease risk for AS patients, but the universality of this risk remains uncertain.[16] In a cross-sectional study by Berg et al. analysing 159 patients with AS with uveitis, patients with uveitis had an increased odds ratio for hypertension and atherosclerosis, suggesting that AS patients with a history of uveitis may increase the risk of hypertension and atherosclerosis.[17] On the other hand, one study from Taiwan evaluating major adverse cardiovascular events in AS groups with and without AU showed an incidence rate of 323.48 per 100,000 person-years in the AU cohort versus 407.24 in those without acute AU. The comparative analysis yielded a relative risk of 0.79, alluding to no significant increase in major adverse cardiovascular events risk for uveitis patients within the AS population.[18] Our study demonstrates that in patients with AS, coronary artery disease was present in 8% in patients with AU, compared to 21% in patients without AU (P = .04). However, the higher prevalence of coronary artery disease seen in AS patients without AU may be attributed to the mean age of patients without AU being higher at 60 ± 1, compared to AS patients with AU at a mean age of 48 ± 4. Hence, a greater mean age could mean a higher chance of having more comorbidities, as well as, which could be contributing factors in the results seen.
In our study, the prevalence of ischaemic cerebrovascular accidents was <1% for both AS patients with and without AU. However, previous research shows an association between AS patients with uveitis and stroke. In one nationwide population-based longitudinal study in Taiwan by Tsung et al., 828 AS patients with uveitis and 3,312 without were observed. Results showed that 137 individuals with uveitis and 344 without suffered strokes during the observation period, establishing uveitis as a significant risk factor for stroke in AS patients (with an adjusted hazard ratio of 1.846, P < .001). Factors such as age, diabetes mellitus, hyperlipidaemia, hypertension, heart failure, pulmonary disease, asthma, coronary disease, and atrial fibrillation were linked to increased stroke risk, and some of these factors have been found more frequently in patients with AS.[18]
Limitations
This study’s retrospective design, utilising data from the 2020 NIS database, comes with inherent limitations. Such retrospective analyses can establish associations but not causality, and they are susceptible to potential coding errors, misclassifications, and missing data, which may impact data accuracy and completeness. Variations in healthcare practices, patient demographics, and hospital resources in different regions may influence outcomes differently, thus affecting the external validity of our results. Furthermore, the study primarily relies on in-hospital data, precluding an assessment of long-term outcomes beyond the hospitalisation period. Despite adjustments for several co-variates, unmeasured confounding factors may exist, which were not accounted for in our analysis. Additionally, the NIS database lacks information on outpatient care, post-discharge outcomes, and patient adherence to treatment regimens, limiting our ability to comprehensively evaluate the impact of interventions and longitudinal management strategies on patient outcomes. Nevertheless, our study utilised a robust database that accounts for millions of admissions nationwide each year, allowing us to select a large subset of tens of thousands of patients with a history of AS.
Conclusion
Our study highlights ethnic disparities in Ankylosing Spondylitis (AS) and Anterior Uveitis (AU) an their co morbidities. While our own statistical analysis revealed minor variations in results, it aligns with existing literature highlighting significant racial disparities in the prevalence of AU among AS patients. Specifically, we reaffirm the increased prevalence of AU in African American AS patients compared to their Caucasian counterparts. Moreover, our findings shed light on associated comorbidities, such as hypertension, diabetes, and chronic pulmonary disease, among individuals with AS. This underscores the need for improved risk assessment and early detection strategies tailored specifically to the AS population, and especially those of the African American race, to enable timely diagnosis and targeted treatment interventions. Addressing these disparities and advocating proactive management approaches can work towards reducing healthcare inequities experienced by various racial groups in AS and ultimately enhancing their overall health outcomes. A diagnosis of AS may present an opportunity for providers to integrate the co-management of silent comorbidities, in addition to AS, which may have significant impacts on patients’ overall health, and allow for the delivery of comprehensive care, while minimising racial disparities, and improving patient outcomes and quality of life.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval was not required for this article, as it is a review article based on various research studies rather than direct patient involvement.
Informed consent
Informed consent was not required for this article, as it is a review article based on existing research studies rather than direct patient involvement.
Credit author statement
All authors contributed to writing and editing the manuscript. All authors approve of the final version.
Data availability
Data is publicly available. Data can be provided upon request.
Use of artificial intelligence
The use of artificial intelligence was not applicable in this article, as it is a review article based on various research studies and does not involve AI tools or systems.