
Abstract
Introduction:
Over the past 20 years, Enhanced Recovery After Surgery (ERAS) has gained popularity in colorectal cancer surgery. In addition, single-port laparoscopic surgery has been shown to have advantages. In colon cancer surgery, single-port laparoscopic surgery and ERAS can improve short-term results. However, whereas the former depends on surgical ability, the latter requires multidisciplinary teamwork. The goal of this project is to investigate the application and outcomes of ERAS protocols throughout the whole continuum of care for colorectal cancer surgery. Examine the details of how ERAS protocols enhance surgical results, with an emphasis on comprehending the subtleties of its use in the treatment of colorectal cancer and the possible obstacles to its broad adoption.
Materials and Methods:
A literature review was conducted, spanning Medline, Embase, and Cochrane Library databases for research conducted between January 2007 and June 2022 and involved specific keywords. The analysis included studies that had to meet two essential criteria: least investigation period of 30 days and compliance with a minimum of four out of the five core components of ERAS.
Results:
Following a comprehensive assessment, five studies satisfied the inclusion criteria. Among these studies, there were two ‘Randomized Controlled Trials’ (RCTs) and three Observational studies. These studies collectively encompassed 1454 patients: 820 patients treated following ERAS protocols, and 634 patients treated with non-ERAS protocols.
Conclusion:
The evidence supporting ERAS’s potential to enhance patient outcomes and its implementation challenges is compiled in this article. That allows to guide future research, enhance treatment following colorectal cancer surgery, and influence clinical practice.
Introduction
On an annual basis, 4.8 million patients worldwide are impacted by gastrointestinal (GI) cancers, which represent approximately 25% of all cancer cases worldwide.[1] Colorectal cancer continues to be the second-most prevalent cause of cancer-related deaths worldwide, despite advances in our understanding of GI diseases.[2] Nonetheless, given the high rates of postoperative complications following liver resections, treatment strategies must be customised to prevent needless exposure to morbid therapies.[3] Patients and healthcare systems struggle with colorectal cancer, a global health issue. Surgery is still the mainstay of treatment, delivering cure and respite. Traditional perioperative care paths for colorectal cancer surgery have been linked to longer hospital stays, more postoperative problems, and slower recovery, affecting patients’ quality of life and healthcare budget allocation.
Enhanced Recovery After Surgery (ERAS) aims to minimise morbidity, accelerate convalescence, and reduce the length of hospital stay.[4] ERAS procedures have revolutionised colorectal cancer therapy in response to these limitations. It includes evidence-based preoperative, intraoperative, and postoperative therapies to reduce surgical stress, preserve physiological function, and speed mobilisation and return to regular activities. ERAS has grown in popularity in colorectal cancer surgery for the past 20 years, promising to transform the clinical experience for patients and doctors. In addition to its cosmetic benefits, single-port laparoscopic surgery has been shown to reduce intraoperative blood loss and the length of hospital stay following surgery by improving bowel movement recovery and further reducing the incision length when compared to traditional multi-port laparoscopic surgery.[5] Both techniques can enhance the short-term results of colon cancer surgery. However, one is a technical strategy that depends on the surgeon’s skill and the other is a systemic strategy that calls for collaboration from specialists in other fields.[6]
ERAS’ efficacy and complete implementation are still being studied. This systematic review examines the literature on ERAS with colorectal cancer surgery. It synthesises the evidence to demonstrate ERAS’s ability to improve patient outcomes and its implementation issues. These findings aim to inform clinical practice, direct future research, and improve colorectal cancer surgery care.
Background of the Study
Colorectal cancer is a global health issue with high rates and fatalities. For many colorectal cancer patients, tumour removal is essential. However, typical perioperative treatment has been related to longer hospital stays, more postoperative issues, and delayed recovery. Over the past 20 years, colorectal cancer surgery has increasingly been analysing the difference between laparoscopy and open colorectal cancer with ERAS methods to address the above concerns. The integrative, research-driven ERAS approach manages patients during surgery to maximise outcomes and speed recovery while minimising healthcare expenses. ERAS includes preoperative patient education, multimodal pain treatment, early oral intake, and mobility.[7] Many colon cancer surgery studies have examined ERAS. These trials have consistently shown improvements in patient satisfaction, hospitalisation time, and surgical complications. ERAS protocols can be complicated and vary among healthcare settings, which may affect their success. ERAS literature for colorectal cancer surgery must also be thoroughly and currently included. This synthesis attempts to provide a comprehensive understanding of ERAS’s effects on patient outcomes and uncover potential efficacy factors.
This systematic review seeks to address knowledge gaps by examining the distinctions between laparoscopy and open colorectal cancer ERAS protocols in colorectal cancer surgery. Through a meticulous analysis of pertinent dissertations and a comprehensive investigation of the disparities between laparoscopic and open colorectal cancer procedures, this study aims to yield valuable insights into the effectiveness of ERAS in enhancing patient outcomes. Additionally, the research endeavours to comprehend the challenges and methodologies associated with the implementation of ERAS. By undertaking this systematic review, the goal is to provide information that can guide clinical practitioners, shape future research initiatives, and contribute to the enhancement of patient care in colorectal cancer surgery.
Rationale of the Study
Surgery remains a critical component in the treatment of colorectal cancer, with advancements in surgical techniques and patient care contributing to therapeutic advancements. There is a growing recognition of the need to improve the perioperative experience for colorectal cancer patients, aligning with modern healthcare’s emphasis on patient well-being and preferences. Given the physical and mental stress often experienced by individuals undergoing colorectal cancer surgery, there is a need to explore techniques that enhance both clinical outcomes and patient satisfaction during the surgical process.
Global healthcare organisations are under pressure to allocate resources efficiently, and conventional approaches to colon cancer surgical care can lead to increased hospital stays, higher readmission rates, and elevated postoperative complications, all of which strain healthcare expenditures. A comparative analysis of laparoscopic and open colorectal cancer surgeries, along with ERAS methods, may indicate potential reductions in hospital stays and complications, offering potential cost savings for healthcare systems.
In the era of evidence-based medicine, interventions and care methods require thorough examination. While there is a growing body of research on ERAS in colorectal cancer surgery, a comprehensive systematic review, coupled with integrated research, is essential to understanding the effectiveness of ERAS and its implementation challenges. Adapting ERAS procedures for laparoscopic and open colorectal cancer surgeries to diverse clinical settings and patient cohorts requires a nuanced understanding of their complexities. Continuous quality improvement in healthcare procedures is imperative to advancing the quality of care in colorectal cancer surgery.
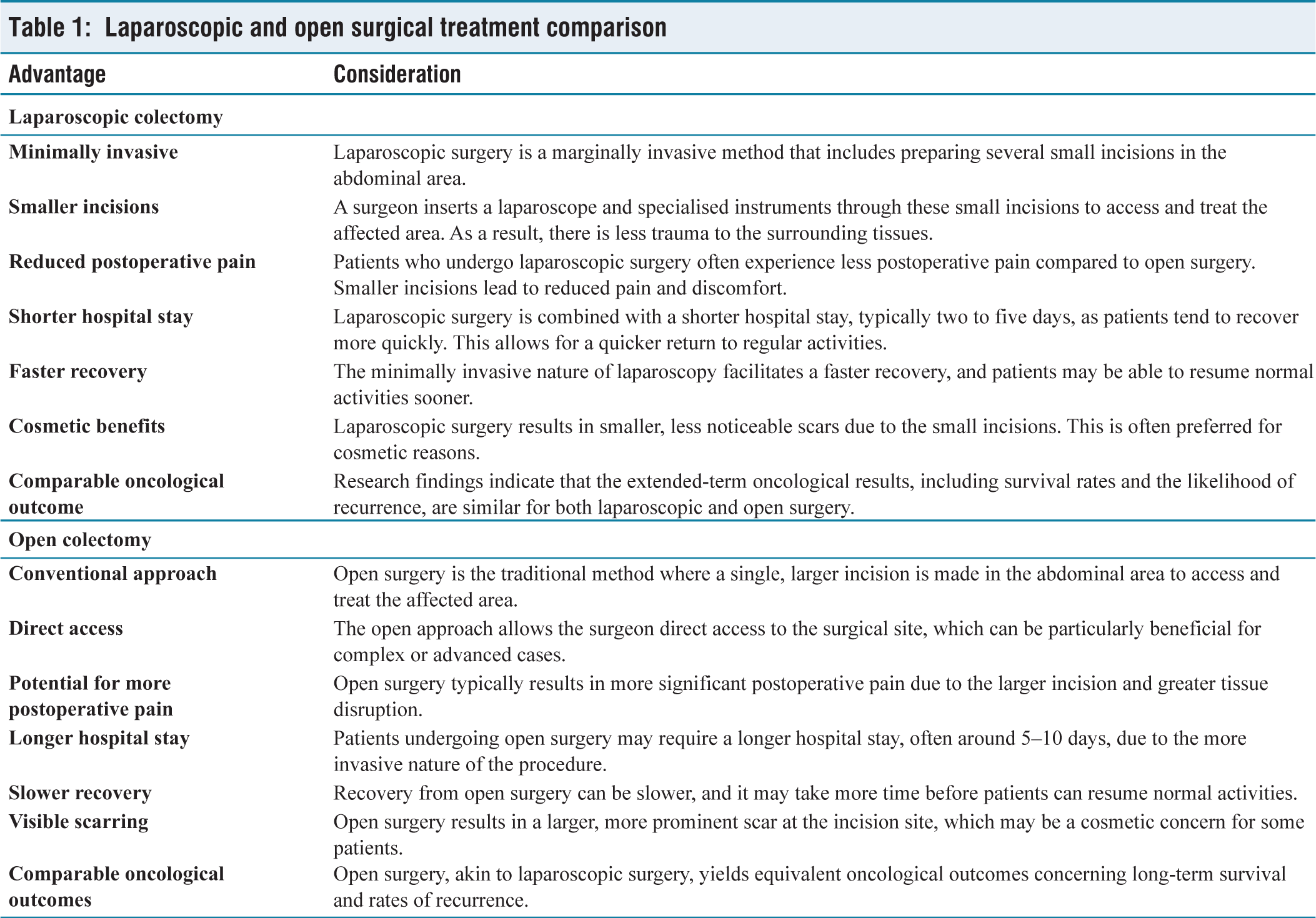
Comparison of Laparoscopic Surgery and Open Colorectal Cancer Surgery
Laparoscopic and open-surgical treatment are two approaches used for handling colorectal cancer. Each approach has its own advantages and considerations [Table 1]. The distinctions between laparoscopic and open surgery approaches for colorectal cancer can be outlined as follows:
Laparoscopic and open surgical treatment comparison
Methods
Screening Process
The systematic search was executed using established databases, including PubMed, MEDLINE, and Cochrane Library. The search strategy included a blend of controlled vocabulary terms (MeSH terms) and relevant keywords. Filters were applied to restrict results to studies published within the last decade, given the evolving nature of ERAS protocols.
Title and Abstract Screening
In the preliminary stage of the study selection procedure, a thorough examination of titles and abstracts was carried out to discover articles that may be pertinent to the research. The inclusion of this phase was crucial in effectively reducing the extensive collection of articles obtained through our systematic search. The screening method adhered to predetermined inclusion and exclusion criteria to guarantee the selection of studies that were in line with our research aims.
Relevance to the research question addressing colorectal cancer surgery and ERAS. Publication in English. The study design incorporates diverse research methods, which could encompass ‘Randomized Controlled Trials’ (RCTs), Cohort studies, or observational studies. Availability of title, also abstract.
Did not pertain to colorectal cancer surgery and ERAS. Were duplicates. Were conference abstracts, commentaries, or reviews without original data. Were not written in English.
Systematic Review
A literature review was conducted, spanning the Medline, Embase, and Cochrane Library databases. This review encompassed research conducted between January 2007 and June 2022. The search strategy involved the utilisation of specific keywords, including ‘enhanced’, ‘recovery’, ‘accelerated’, ‘rehabilitation’, ‘fast-track’, and ‘multimodal perioperative care’, alongside the terms ‘colon’ and ‘rectum’. The analysis included studies that had to meet two essential criteria: least investigation period of 30 days and compliance with a minimum of four out of the five core components of ERAS, as outlined by Kehlet and Wilmore[8] [Table 2].
Baseline characteristics of the included studies

The collected articles underwent an evaluation of their methodological quality using established and validated criteria. The study examined various outcome measures, including the number of patients, duration of hospital stay, and mortality rates. Additionally, this research involved systematic reviews and meta-analyses of event-related potentials (ERPs) by utilising data sourced from well-regarded surgical and anaesthesiology journals. To ensure a comprehensive search, further relevant publications were identified via manual exploration of digital references and citations in chosen articles. Furthermore, consultations were held with international experts who specialise in Enterprise Resource Planning (ERP) system implementation to ensure that no relevant work was overlooked. The data extraction process was independently conducted by two investigators.
Results
In total, the search strategy executed on the databases initially generated 250 articles. Following a comprehensive assessment, five studies satisfied the inclusion criteria [Figure 1]. Among these studies, there were two ‘Randomized Controlled Trials’ (RCTs) and three observational studies. These studies collectively encompassed 1454 patients, with 820 patients subjected to treatment following ERAS protocols, and 634 patients treated with non-ERAS protocols.
Consort diagram
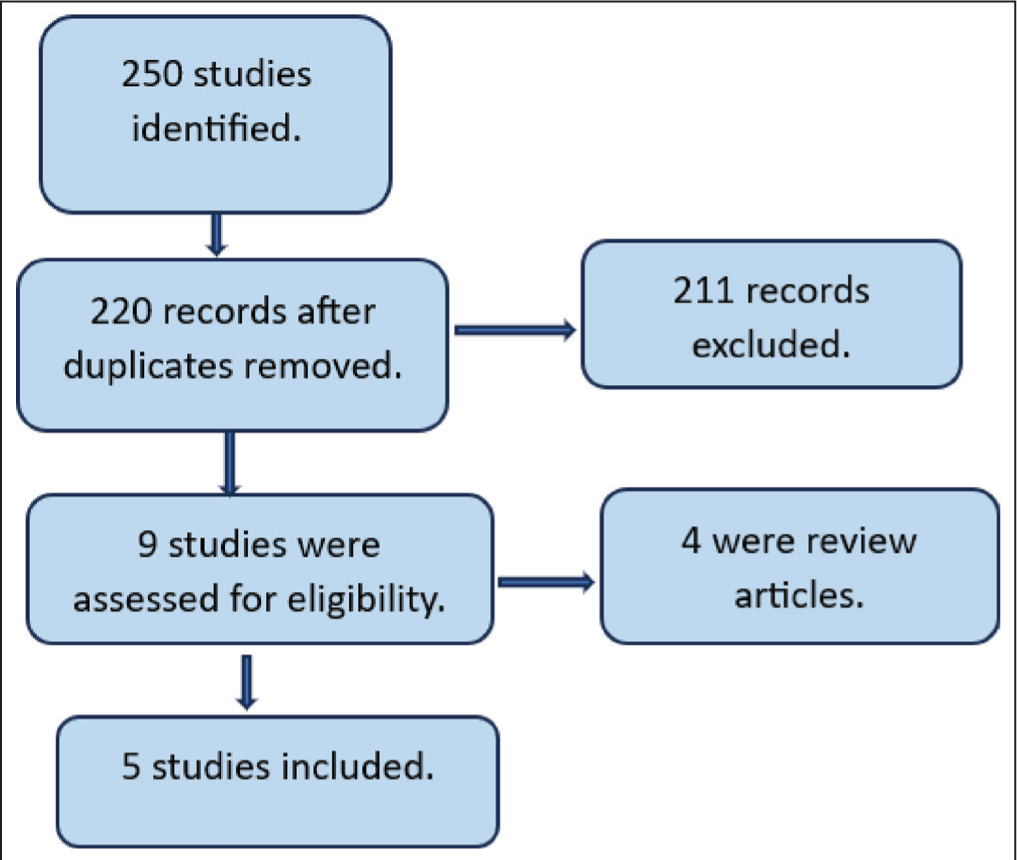
Table 2 functions as a succinct resource for comprehending the range of ERAS implementation studies, elucidating disparities in patient cohorts, research methodologies, and regional distributions. Comparisons of this nature hold significant value in the process of synthesising evidence pertaining to the efficacy of ERAS protocols in the context of colorectal surgery within diverse healthcare environments.
Odds of Bias Assessment
Two distinct tools were used to assess methodological quality:
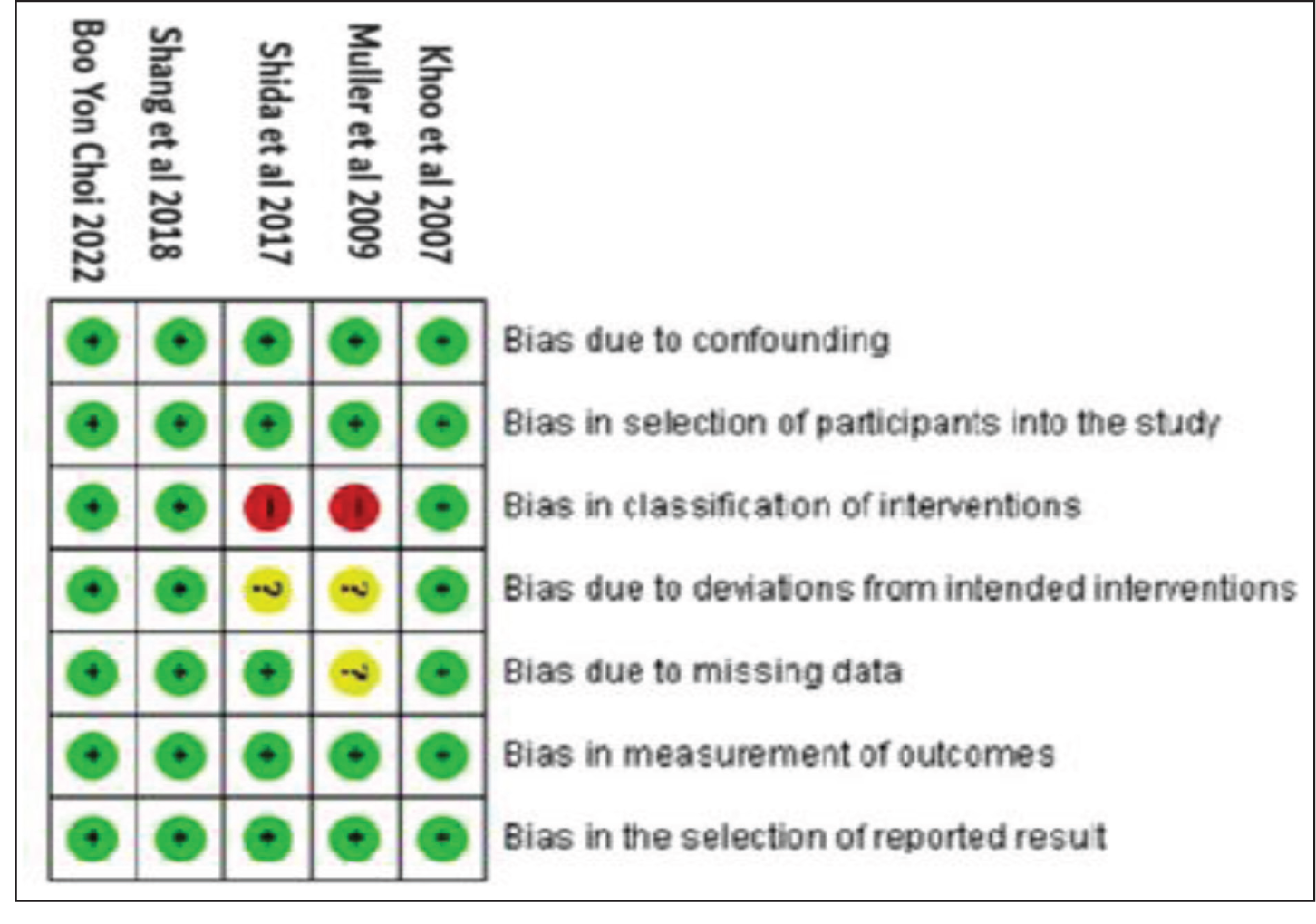
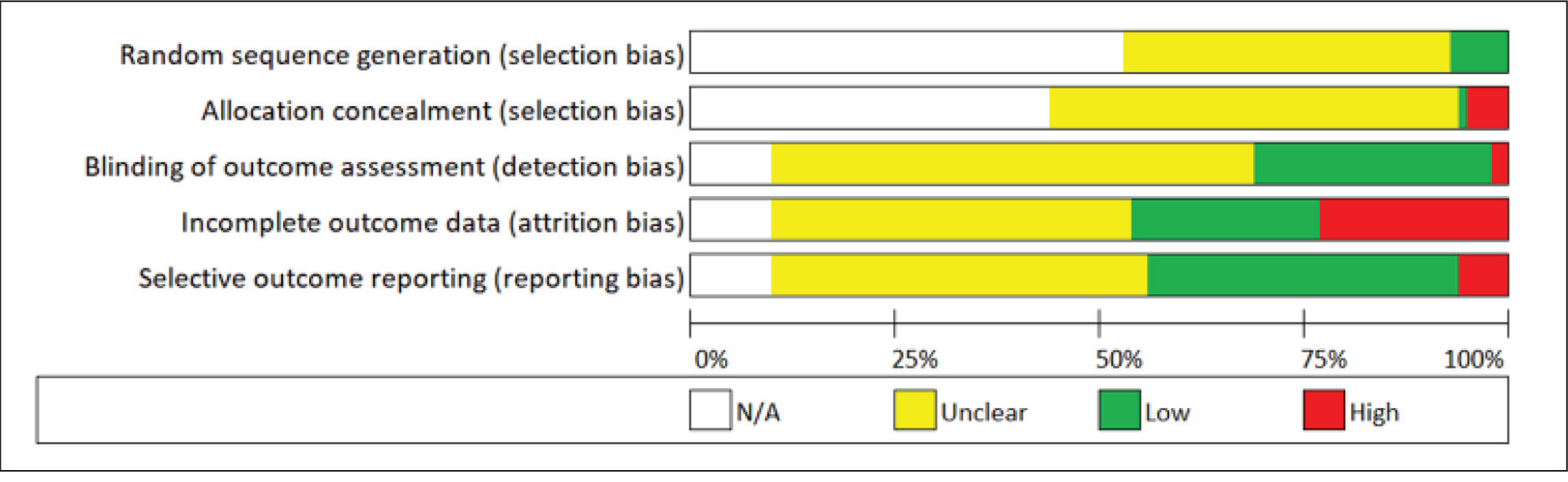
Cochrane Tool for RCTs: Evaluated the quality of randomised controlled trials, covering domains like selection, performance, detection, attrition, reporting, and potential biases [Figure 2]. Newcastle–Ottawa Scale[14]: Assessed non-randomised comparative studies in terms of patient selection, group comparability, and outcome assessments [Figure 3]. This scale is particularly useful for observational and cohort studies.
Risk of bias summary
Risk of bias graph: review authors’ judgments about each risk of bias item presented as 275 percentages across all included studies
Two individuals reviewed this, and in cases where it was deemed necessary, a third author was engaged to address discrepancies between the initial two reviewers.
Table 3 furnishes a comprehensive overview of patient attributes and observed results in research comparing cohorts undergoing ERAS protocols with those not employing ERAS protocols. This analysis provides valuable insights into the potential benefits linked to ERAS protocols, encompassing shorter hospitalisation periods and potentially lowered rates of morbidity. These aspects hold substantial significance when assessing the effectiveness of these protocols within the realm of colorectal surgery.
Baseline characteristics of the included population
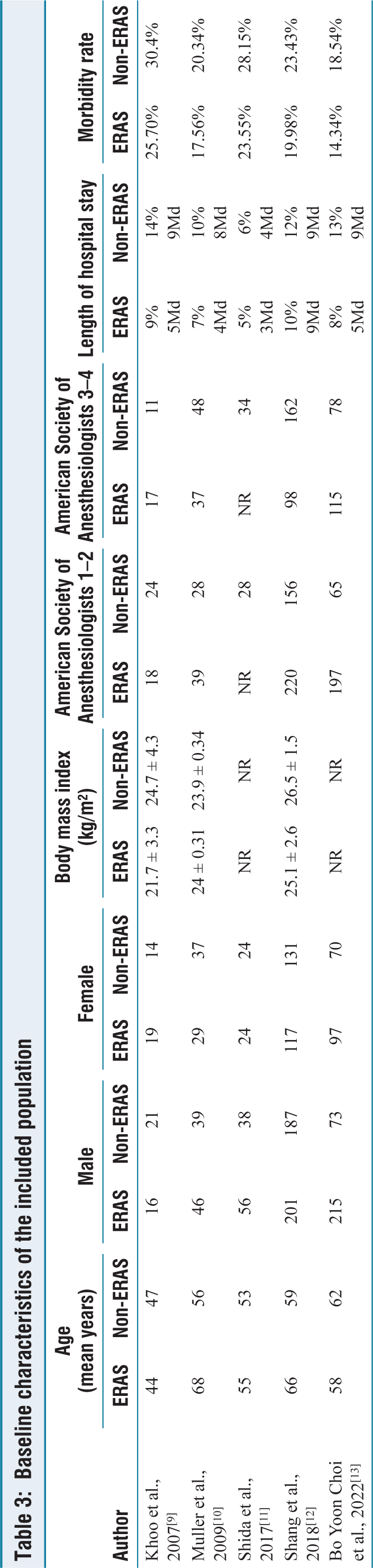
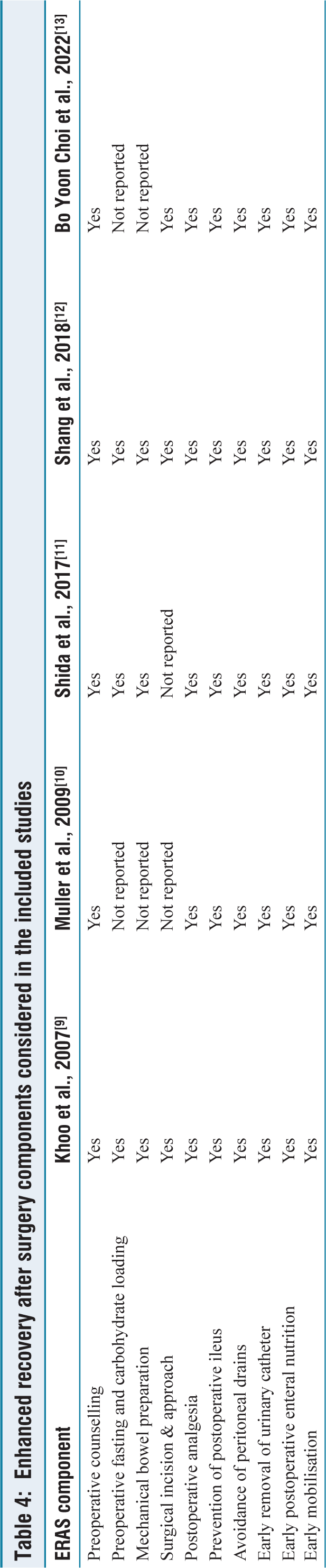
Table 4 illustrates that ERAS protocols are specifically crafted to improve perioperative care, expedite recovery, and lower the likelihood of post-surgical complications for patients.
Enhanced recovery after surgery components considered in the included studies
Data Synthesis
In more than a third of the studies, investigators calculated the odds ratio (OR) for binary results, mean difference (MD) for continuous outcomes, and risk difference (RD) in cases where no occurrences were noted in either group. These analyses were conducted using intention-to-treat data for all participants, and random effects models were employed when there was significant heterogeneity among the studies. The assessment of heterogeneity involved the utilisation of the Cochran Q test (version 2), and I2 was defined as:
Low heterogeneity: 0%–50% Moderate heterogeneity: 50%–75% 75%–100% indicates high heterogeneity.
The study planned to produce funnel plots for the included studies’ outcomes and assess their symmetry to determine publication bias as follows:
Duration of Hospital Stay
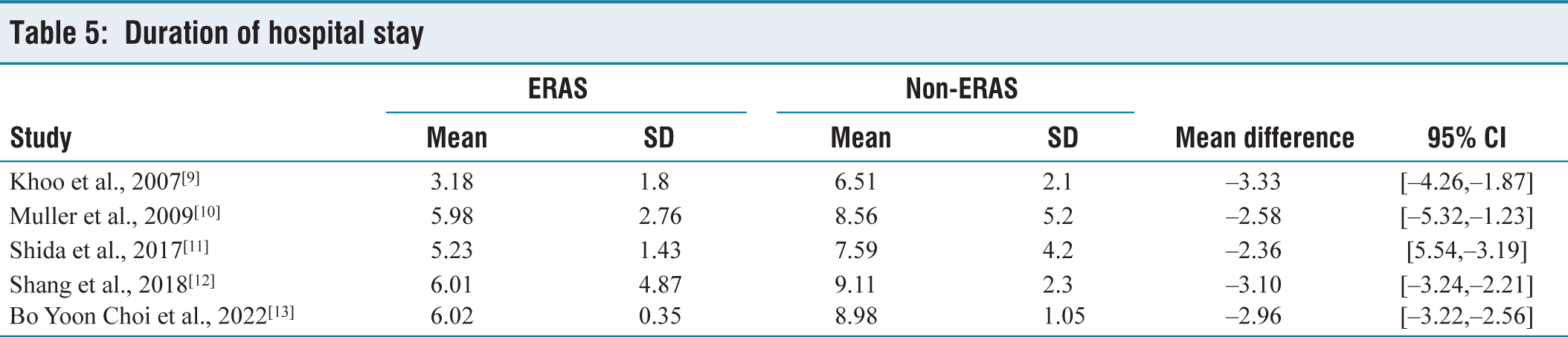
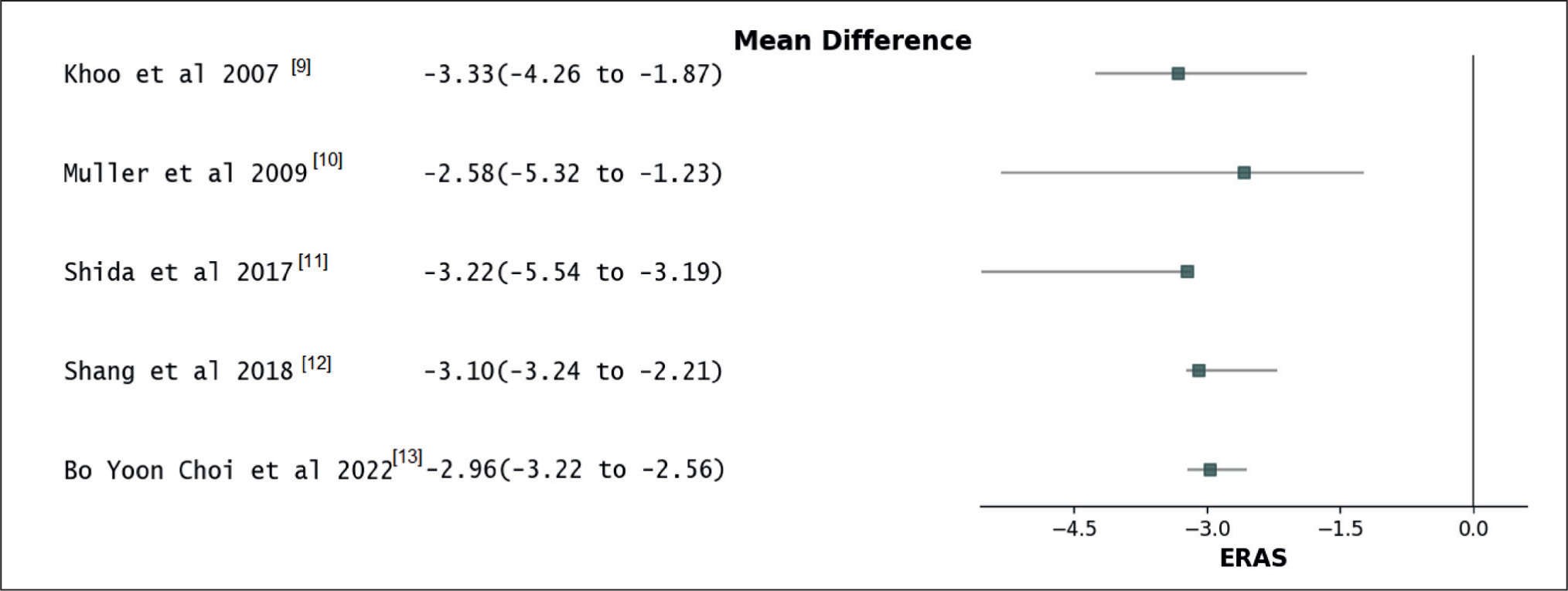
An examination of data from a combined total of 1454 patients across five separate trials demonstrated that incorporating ERAS protocols resulted in a notably shorter hospitalisation duration compared to non-ERAS protocols. The calculated mean reduction in the length of hospital stay was –2.87 days, with a 95% confidence interval spanning from –3.33 to –2.36 days [Table 5]. The observed variation was established as statistically significant, as indicated by a P value of <.00001. The degree of variation among the studies was modest, with an I2 value of 13% and a P value of .21 [Figure 4].
Duration of hospital stay
Forest plot for duration of hospital stay
Total Post-operative Complications
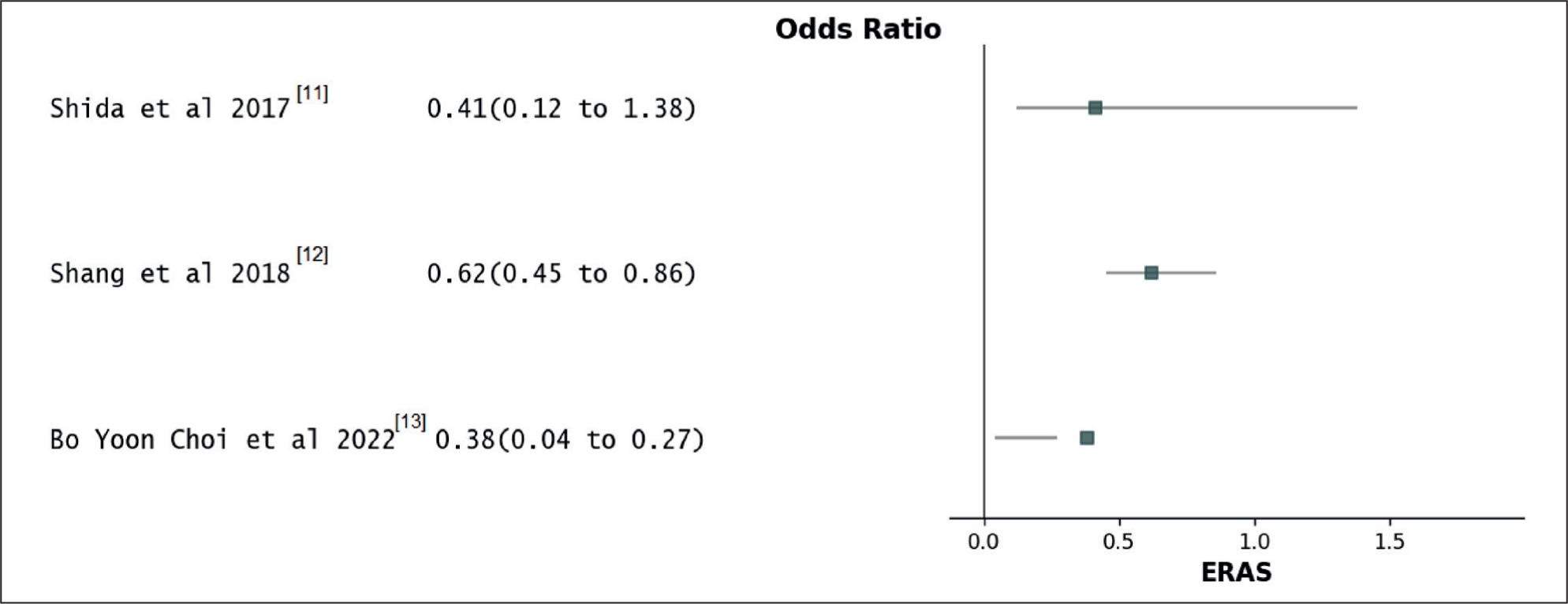
An examination of data from three distinct studies involving 1233 patients unveiled that the implementation of ERAS protocols directed to a reduced likelihood of experiencing postoperative complications in contrast to protocols outside the scope of ERAS. The OR was computed at 0.47, with a 95% confidence interval spanning from 0.34 to 0.61 [Table 6]. This discovery was statistically significant, as confirmed by a P value of <.00001. There was a moderate degree of diversity observed among the studies, with an I2 value of 67% and a significance level of .01 [Figure 5].
Total post-operative complications

Forest plot for total post-operative complications
Duration Until the Initial Oral Liquid Diet
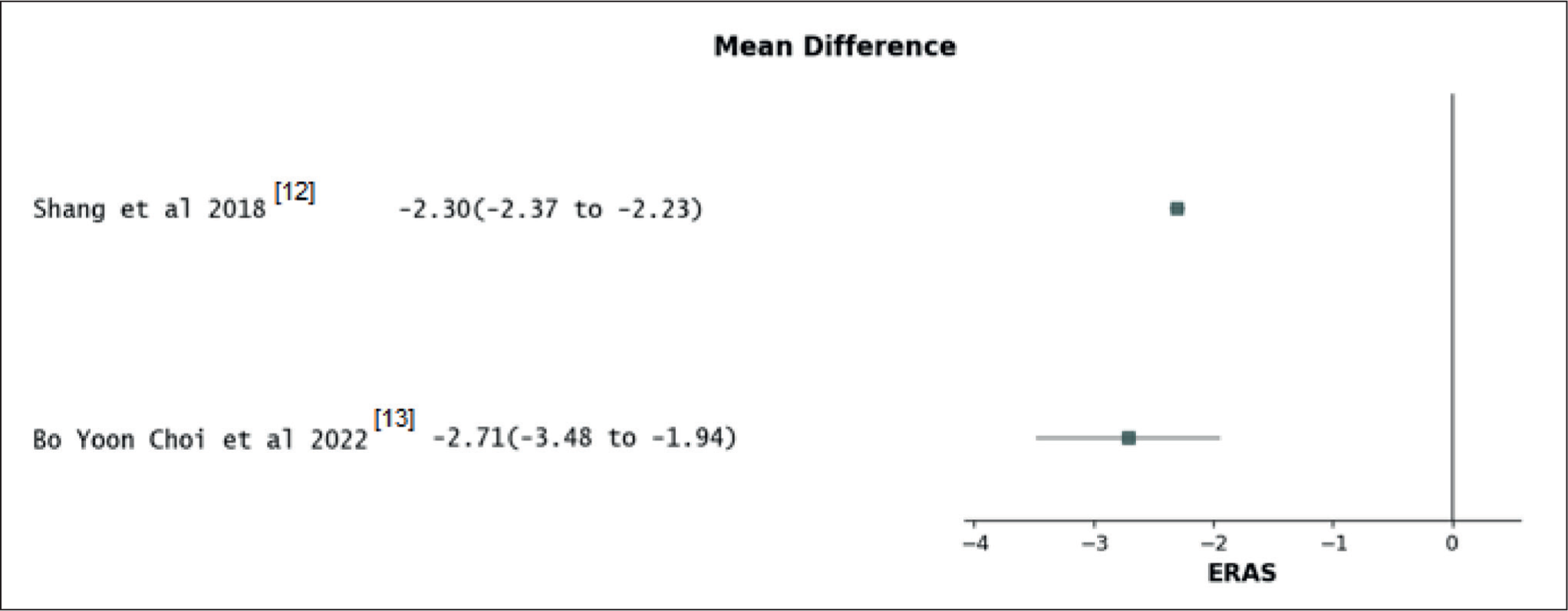
An examination involving 778 patients from two research studies revealed that the implementation of ERAS protocols drove to a notably reduced time before commencing a liquid diet via oral when as to non-ERAS protocols. The MD was computed at –2.28 (with a 95% confidence interval ranging from –2.22 to –2.36) [Table 7], and the P value was <.00001, signifying an exceptionally significant outcome. The degree of variability observed between the level of diversity in the studies was negligible, as determined by an I2 value of 11% and a non-significant P value of .26 [Figure 6].
Duration until the initiation of the initial oral liquid diet

Forest plot for time to initial oral liquid diet
Duration Until the Initiation of the Initial Oral Solid Diet
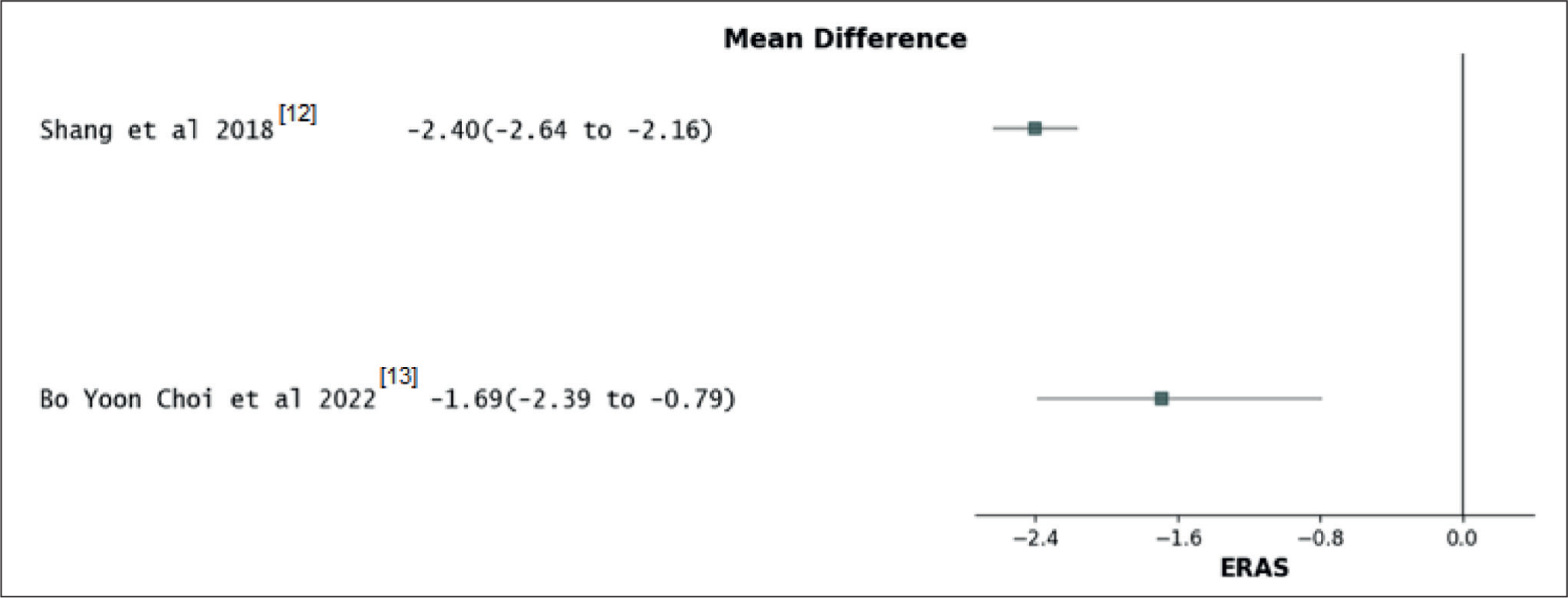
An analysis involving 778 patients from two clinical trials revealed that the adoption of ERAS protocols oversaw a significant reduction in the time required to initiate an oral solid diet compared to the utilisation of non-ERAS protocols. The calculated MD was –2.39, with a 95% confidence interval ranging from –2.18 to –2.61 [Table 8]. The resulting P value was <.00001, signifying an exceptionally significant outcome. The degree of variation observed between the degree of variation in the study was deemed reasonable, as evidenced by an I2 value of 68% and a statistically significant P value of .019 [Figure 7].
Time to initial oral solid diet

Forest plot for time to initial oral solid diet
Major Complications
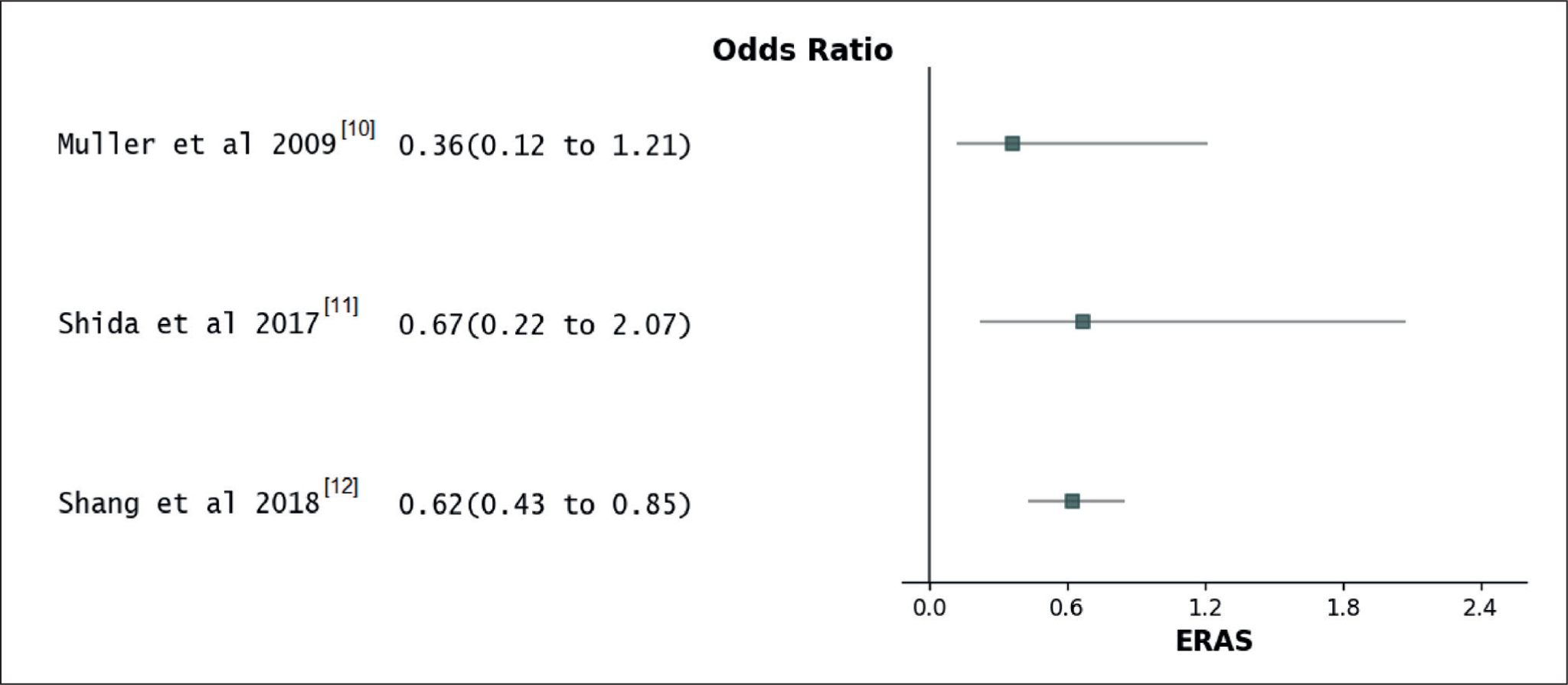
An examination of 929 patients from three separate trials discovered that the adoption of ERAS protocols resulted in a reduced likelihood of encountering substantial postoperative complications compared to non-ERAS protocols. The OR was computed as 0.59, with a 95% confidence interval spanning from 0.42 to 0.79, and a P value of .0008, signifying statistical significance [Table 9]. The degree of variation among the studies was minimal, with an I2 value of 0% and a P value of .69 [Figure 8].
Major complications

Forest plot for major complications
Comparison of Laparoscopic Surgery and Open Colorectal Cancer Surgery Correlated with Systemic Analysis and the Present Research Study
The association between laparoscopic and open surgery in the context of colorectal cancer can be linked to the current systematic review of ERAS in colorectal cancer surgery, with a specific emphasis on its effectiveness and application. A systematic review, as a method, compiles and consolidates existing research studies to offer an all-encompassing comprehension of a particular subject [Table 10]. This correlation between these two facets can be elucidated as follows:
Comparative analysis of laparoscopic and open colorectal cancer surgery
The comprehensive systematic review on the effectiveness and application of ERAS in colorectal cancer surgery has considered both laparoscopic and open surgical methods. This review has assessed the results, the extent of ERAS integration, and patient-centred viewpoints, offering valuable knowledge for healthcare providers and policymakers. This information can aid in enhancing the surgical journey for individuals diagnosed with colorectal cancer.
Discussion
An evaluation encompassing 1454 patients from five comparative studies demonstrated that the adoption of ERAS protocols resulted in decreased complications after the surgery, faster restoration of bowel function, and a briefer hospital stay, all beyond elevating the risk of readmission or the necessity for additional surgical procedures. The results underwent validation via sensitivity and subgroup analyses, confirming the reliability and uniformity of the outcomes.
Previous meta-analyses have examined the influence of ERAS protocols on outcomes after surgery in electoral surgeries. Remarkably, the outcomes observed in emergency surgery matched those of elective surgery studies. For instance, Ji et al.[15] found that ERAS procedures improved outcomes in elective pancreatic surgery, while Wang et al.[16] discovered similar results in elective gastric cancer surgery. Additional research has also documented positive results in individuals undergoing hepatectomy, oesophageal cancer surgery, and colorectal surgery.[17–19]
Certain preoperative elements within ERAS protocols, like support for nutrition and loading of carbohydrates, may not be practical in emergency circumstances. Nevertheless, numerous components of these protocols remain relevant and viable. While thorough preoperative counselling might face constraints, patients and their families can still receive information regarding the surgery, possible perioperative complications, stoma needs, and anticipated hospitalisation duration. Despite some limitations, the objective administration of intravenous fluids and antibiotics is indispensable and attainable in the context of emergency major abdominal surgery.
Moreover, numerous intraoperative and postoperative ERAS strategies can be effectively implemented under present circumstances. Nevertheless, it’s important to acknowledge that postoperative ERAS approaches might present difficulties for critically ill patients undergoing emergency abdominal surgeries, as they may necessitate extended periods of intensive care, mechanical ventilation, and circulatory support in contrast to those undergoing less intricate procedures.[20]
Although nearly all studies indicated the feasibility of the ERAS protocol components, subgroup analysis for critically ill postoperative patients requiring extensive respiratory and circulatory support was not performed. Therefore, future research should focus on assessing the applicability of ERAS protocols in this specific subgroup.
Although the study employed an objective methodology to present the most robust comparative evidence and evaluate bias, it is not exempt from constraints. Among the five suitable strategies in the databases, three were non-randomised observational studies, possibly introducing selection bias. Furthermore, the restricted number of eligible studies (fewer than 10) hindered the examination of potential publication bias.
Scope for Future Research
Future research could focus on designing and validating patient-specific ERAS protocols, investigating personalised routes based on age, comorbidities, nutrition, and genetics to enhance perioperative precision and effectiveness, potentially decreasing morbidity and improving recovery. Further investigation into ERAS’s long-term effects and impact on colon cancer survivors’ quality of life is needed, including parameters like disease-free survival, late complications, bowel function, and patient-reported outcomes. Additionally, exploring methods and challenges in implementing ERAS across diverse healthcare settings could identify strategies to optimise adoption and benefit more patients, ultimately improving care and outcomes in colorectal cancer surgery.
Conclusion
ERAS protocols are usually utilised in elective surgical settings. They have demonstrated improvements in cancer-related outcomes by reducing post-operative complications, accelerating bowel function recovery, and shortening hospital stays, all without increasing the likelihood of readmission or the necessity for additional surgical procedures. It is advisable to consider extending the application of ERAS protocols to emergency abdominal surgeries.
Supplemental material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Dr B. Krishna Prasanth, Department of Community Medicine, Sree Balaji Medical College & Hospital.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Research Project of the Jiangsu Commission of Health Research Approval Number: K2023062.
Informed consent
Informed consent was not applicable for this article, as it is a review article based on previously published research and does not involve any direct interaction with patients.
Credit author statement
The manuscript has been read and approved by all the authors, the requirement of authorship has been met, and all the authors believe it presents honest work.
Dr. Gaurav Tyagi: Research and Drafting. Dr. Yin Kai: Research and contributed to the article. Dr. Xu Zhang: Research and contributed to the article.
Data availability
Data availability is not applicable for this article, as it is a review article based on published research and does not involve any original data collection.
Use of artificial intelligence
The use of artificial intelligence tools is not applicable for this article, as it was prepared solely based on manual analysis and drafting from various research articles.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.