
Abstract
Background:
Oropharyngeal squamous cell carcinoma (OPSCC) associated with high-risk human papillomavirus (HPV) is a distinct form of head and neck squamous cell carcinoma (HNSCC) in its aetiology, morphology and prognosis. Identification of HPV status is helpful in assessing the prognosis of these tumours and in providing tailored treatment for these cases. P16 identification by immunohistochemistry (IHC) is the gold standard and highly sensitive method.
Methods:
Seventy-five cases of HNSCC were tested by IHC for p16. The results were evaluated using a chi-square test and correlated with histopathological and clinical parameters. A value of P < .05 was taken as significant.
Results:
Out of 75 cases, 14.6% were positive for p16, 1.3% were equivocal, and 84.1% were negative. The mean age of p16 positive cases was 55.72 years. Men to women ratio is 1.7:1. The oral cavity is the most commonly affected site among p16-positive cases, followed by the oropharynx and laryngopharynx. The majority of the cases (54.5%) were Grade III and non-keratinizing.
Conclusion:
P16 is an easily available, cost-effective Surrogate Marker for HPV-associated HNSCC. These cases were of high grade and mostly conventional non-keratinizing type, but they, still had better prognostic factors, like a lesser stage, decreased nodal metastasis, lesser depth of invasion (DOI), a lesser degree of the worst pattern of invasion (WPOI), and no involvement of the cortical bone or overlying skin. Therefore, routine staining for p16 IHC could be considered for all HNSCCs.
Keywords
Introduction
Squamous cell carcinoma (SCC) is the most common malignancy arising in the head and neck region. It arises from the mucosal epithelium of the oral cavity, pharynx and larynx. Its incidence is attributed to alcohol consumption, tobacco chewing, smoking, etc. In particular, pharyngeal SCC is more associated with oncogenic strains of human papillomavirus (HPV) infection, especially with HPV16 and, to a lesser extent, with HPV18.[1]
HPV-associated oropharyngeal squamous cell carcinoma (OPSCC) is a distinct type with respect to its aetiology, histomorphology and prognosis.[2] It typically occurs in the young men population.[3] It has a strong predilection for the base of the tongue and palatine tonsils and often presents at a higher stage with nodal involvement.[4] HPV and epidermal growth factor receptor (EGFR) status of tumours are the most predictive molecular markers for advanced-stage tumours. Overall, for head and neck squamous cell carcinoma (HNSCC), HPV status is the most valid, robust diagnostic and prognostic biomarker to date.[5]
Various methods for the demonstration of HPV are in situ hybridisation (ISH), immunohistochemistry (IHC), polymerase chain reaction (PCR) and Southern blot hybridisation, among which p16 IHC is highly sensitive and used as surrogate marker for HPV detection.[6]
Materials and Methods
This was a prospective observational study of all cases of SCC of the head and neck (both incisional biopsies and excision specimens) diagnosed in our Hospital from December 2018 to October 2019.
Cases with inadequate tissue and cases treated with radiotherapy/chemotherapy were excluded from the study.
Sample Size Calculation
Since the primary objective of the study is to find out the percentage of p16 positivity in HNSCC, we kept 74% (61) as the p16 positivity percentage for the calculation of sample size.
Using the following formula
n = Z2 pq/ d2
Z = Standard normal variate value = 1.96 (95% confidence interval)
p = expression rate of p16 by IHC in HNSCC, which is 75%
Q = 1-p i.e. 26% d = clinical allowable error = 10%
Using the above formula and calculation, the minimum required sample size was 75 cases.
Immunohistochemical Analysis
IHC was performed using the Ventana BenchMark XT instrument. 10% formalin-fixed paraffin-embedded specimens were cut at 4 μm thickness. Positive controls were run simultaneously. A strong brown nuclear immunoreactivity was considered positive staining.
The staining pattern of p16
Negative- <50% diffuse and strong nuclear with or without cytoplasmic staining.
Equivocal- <70% but > 50% diffuse and strong nuclear with or without cytoplasmic staining.
Positive- >/=70% diffuse and strong nuclear with or without cytoplasmic staining.[7]
Statistical Analysis
All the continuous variables were represented by mean plus or minus standard deviation. Percentages represented all the categorical variables. Comparison of the continuous variables, if any, was done by independent sample t-test. Comparison of the categorical variables was done by either the Chi-square test or Fischer’s exact test. Data entry was done in an MS Excel spreadsheet. Data analysis was performed by SPSS version 25.0 software. All P values <.05% were considered statistically significant.
Results
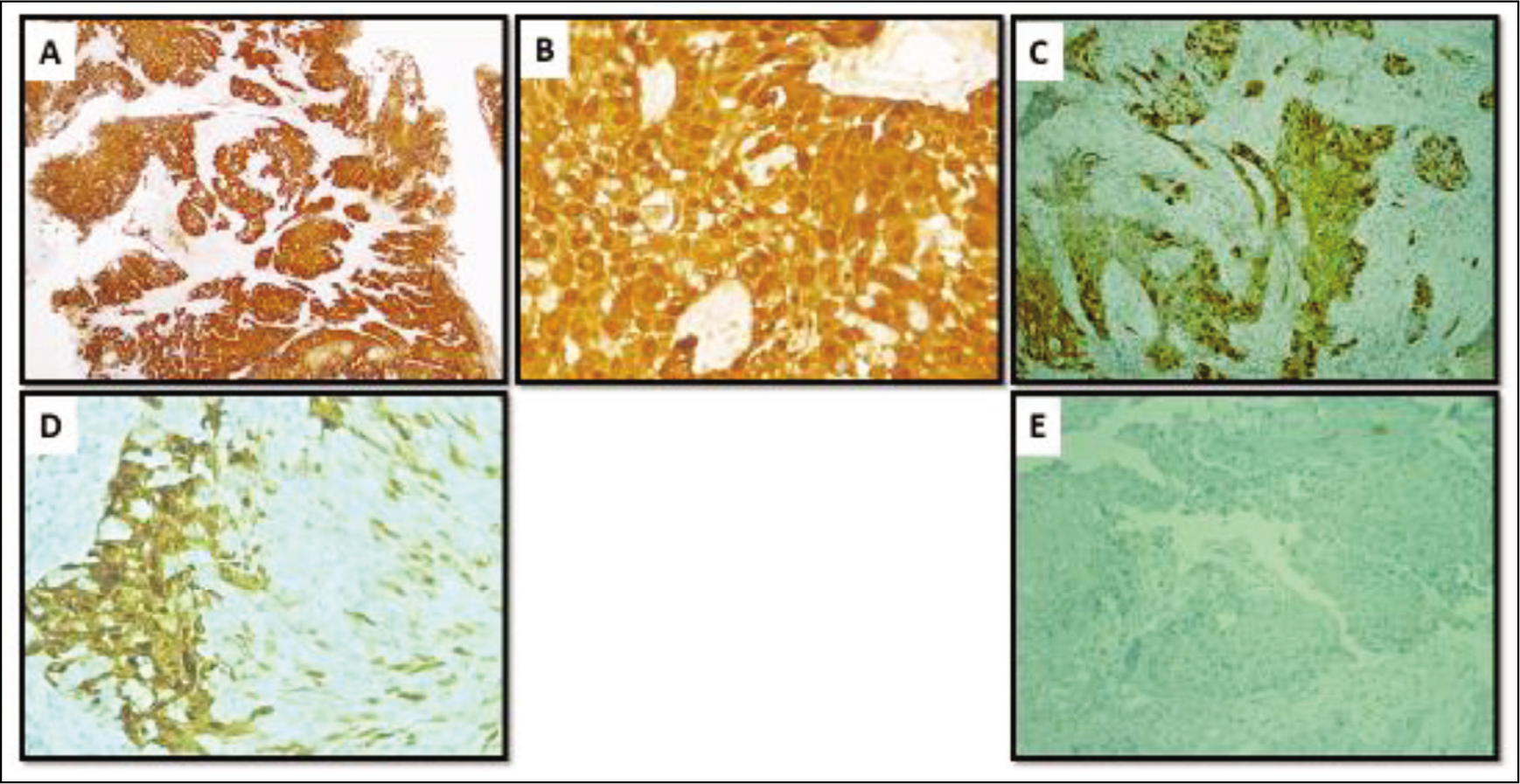
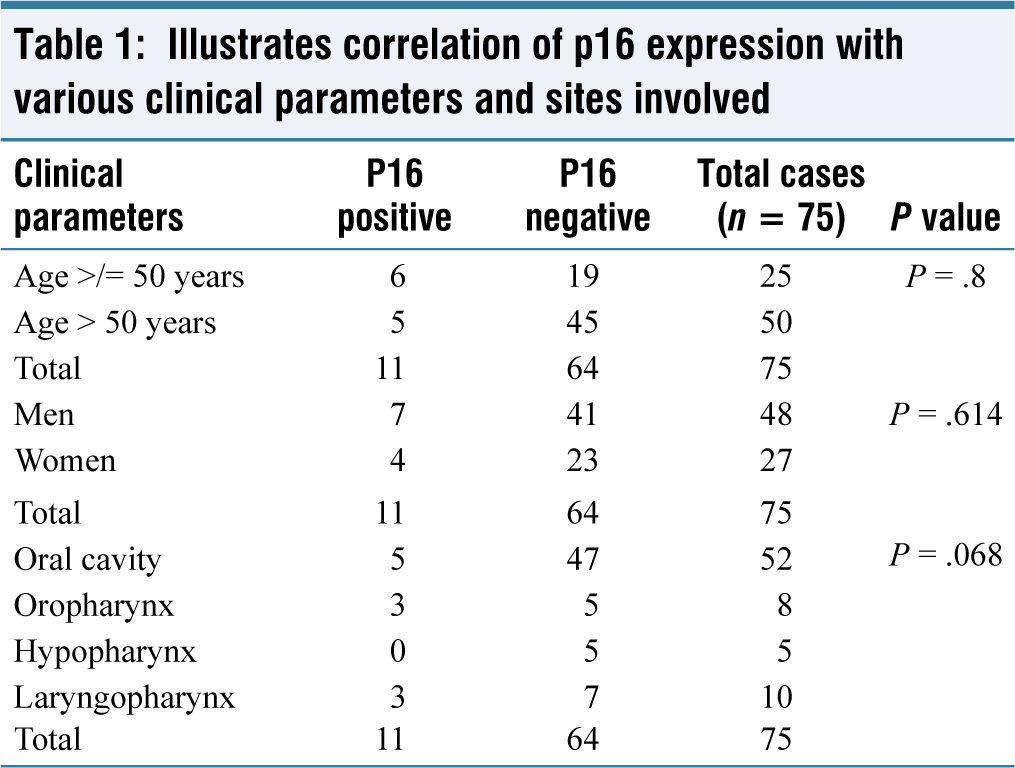
A total of 75 cases of SCC were included in the study. Among 75 cases, 14.6% of cases were positive for p16, 1.3% were equivocal, and 84.1% were negative [Figure 1]. The age of the patients ranged from 27 to 80 years with a mean age of 55.72 years. P16 positive cases ranged from 30 to 67 years with a mean age of 49.27 years. More than half of p16 positive cases (54.5%) were less than 50 years of age. There was a slight male preponderance with a ratio of 1.7:1 [Table 1]. Out of 75 cases, 12 were smokers, and 10 had a habit of tobacco chewing. Lip and oral cavity were involved in 69.3%, laryngopharynx in 13.3%, oropharynx in 10.7% and hypopharynx in 6.7% of the cases. Of this, 45.4% (n = 5) of the p16 positive cases were seen within the oral cavity, followed by the oropharynx (27.3%) (n = 3) and laryngopharynx (27.3%) (n = 3). None of the SCCs from the hypopharynx were positive for p16. One case from the oral cavity (n = 1) showed an equivocal staining pattern for p16 [Table 1].
P16 expression in head and neck squamous cell carcinoma. (A & B) P16 positivity with diffuse and strong cytoplasmic and nuclear expression in 90% of the cells in Squamous cell carcinoma (IHC; original magnification ×100 & 200). (C & D) Equivocal p16 staining with cytoplasmic and nuclear expression in 50% and 30% of the cells in Squamous cell carcinoma (IHC; original magnification ×200). (E) P16 negative (IHC; original magnification ×100)
Illustrates correlation of p16 expression with various clinical parameters and sites involved
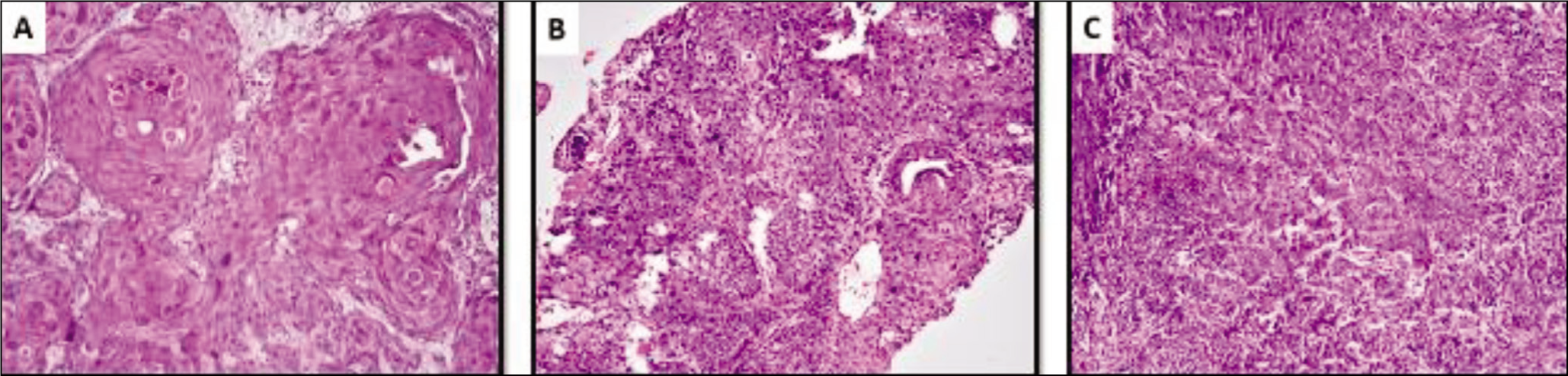
Although p16 positive oropharyngeal carcinomas need not be graded, we compared the grade of the p16 positive cases for our reference: 54.5% (n = 6) were Grade III, 36.4% (n = 4) were Grade II, and 9.1% (n = 1) were Grade I [Figure 2] [Table 2].
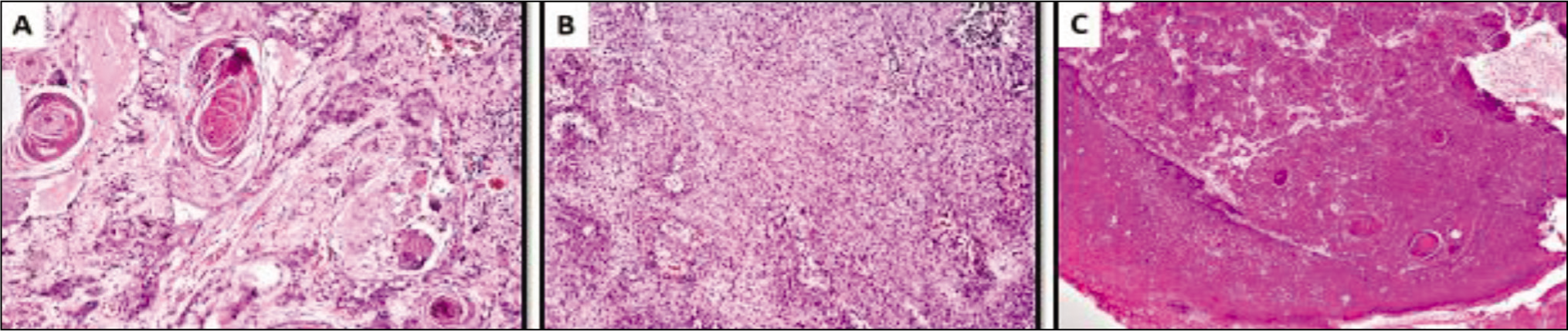
Histologic grades in p16 positive head and neck squamous cell carcinoma. (A) Grade I- p16 positive Squamous cell carcinoma exhibiting keratin pearls and intercellular bridges. (Haematoxylin and eosin stain; original magnification ×100). (B) Grade II- p16 positive Squamous cell carcinoma with individual cell keratinization. (Haematoxylin and eosin stain; original magnification ×100). (C) Grade III- p16 positive Squamous cell carcinoma composed of sheets of poorly differentiated tumour cells (Haematoxylin and eosin stain; original magnification ×200)
Illustrates correlation of p16 expression with various histologic grades and morphology
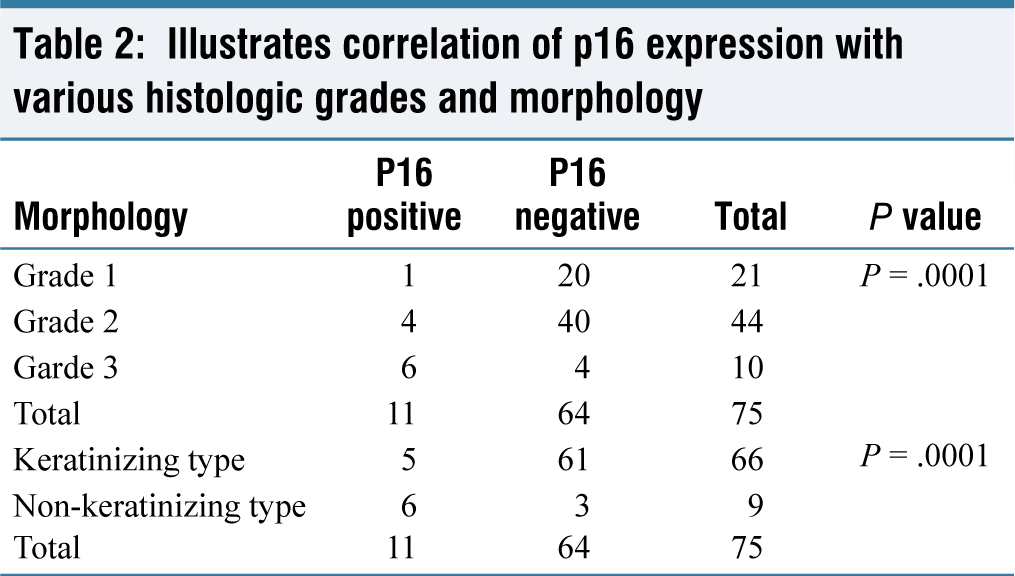
Among p16 positive cases, 54.5% (n = 6) were non-keratinizing SCC, and keratinizing SCC constituted 45.5% (n = 5). Among negative and equivocal cases, 4.7% were of non-keratinizing type where, as 95.3% of cases showed keratinisation [Figure 3] [Table 2]. Six cases (54.5%) of p16-positive HNSCC showed no dysplasia of the lining squamous epithelium [Figure 3].
Keratinizing and non-keratinizing subtype in p16 positive head and neck squamous cell carcinoma. (A) Keratinizing SCC – p16 positive Squamous cell carcinoma exhibiting keratin pearls and intercellular bridges. (Haematoxylin and eosin stain; original magnification × 400). (B) Non-keratinizing SCC-p16 positive Squamous cell carcinoma with no evidence of keratinization (Haematoxylin and eosin stain; original magnification ×400). (C) p16 positive squamous cell carcinoma with no dysplasia of the surface epithelium. (Haematoxylin and eosin stain; original magnification ×100)
All p16-positive cases were conventional SCC (100%). Among p16-negative cases, two cases were of spindle cell morphology (3.1%), and the remaining were conventional SCC (96.9%). Associated non-specific findings of candidal (n = 2) and actinomycotic infection (n = 1) were also seen in 2.7% and 1.3% cases, respectively.
Most of the cases involved the right side of the head and neck compared to the left in both p16 positive and negative categories, and all were unifocal. Lymphovascular invasion (LVI), perineural invasion (PNI) and peritumoral lymphoid response (PTLR) were assessed in all the cases. Among p16 positive cases, lymphovascular invasion was seen in 2 cases (18.2%). Perineural invasion was identified in 9% (n = 1) of the p16 positive cases and 20.3% (n = 13) of the p16 negative and equivocal cases. Peritumoural lymphoid response (PTLR) was categorised as mild, moderate and severe according to the number of lymphocytes present around the tumour. Most of the p16 positive cases had a mild and moderate response, which constituted 45.5% each, and only 9% had a brisk response.
Most of the diagnostic biopsies were followed up for one year. Resection was performed in 14 cases, including two p16-positive SCCs. Parameters like tumour size, type of infiltration, margin status, depth of invasion (DOI), worst pattern of invasion (WPOI), satellite nodules, and staging were noted for all the resected specimens (n = 25).
Of the total 39 resected cases, including the follow-up cases, four were positive for p16.
The maximum tumour size in the resected cases varied from 0.7 cm to 6 cm, with a mean size of 2.5 cm. An important criterion in defining “T” staging is the DOI. Among p16 positive resected cases (n = 4), tonsillectomy specimen was received in fragments. Therefore, DOI could be assessed only for three cases. Two cases had a DOI of 0.5 to 1 cm. One case had a DOI of less than 0.5cm, and none were more than one cm.
WPOI is a validated worse predictor in oral SCC and is interpreted at the invasive front of the tumour. In our study, among p16 positive resected cases, one case had the WPOI 5, while among p16 negative and equivocal category, six cases with the WPOI 5 were seen. Among p16 positive resected cases (n = 4), skeletal muscle involvement was seen in one case. None of the p16-positive resected cases had nodal metastases.
AJCC staging of resected specimens was done according to the CAP protocol. Three of the p16 positive cases were stage II (n = 3), and one was stage I (n = 1).
Discussion
In this study, 75 cases of HNSCC were reviewed, and p16 was found positive in 14.67% (n = 11) of the cases. In a systematic review analysis, Stein et al. demonstrated a significantly increasing trend of HPV-positive SCCs worldwide. Most of the countries had a prevalence between 39.5% and 75%, with the highest in Taiwan (75%) followed by Canada (61%) and the lowest in Spain (6.1%). The present study has a lower prevalence comparable to other studies in India.[8,9]
P16 positivity inversely correlated with age, with higher prevalence in the age group of <50 years (54.5%). This pattern of occurrence in younger individuals is similar to the study by Ang et al.[10] and Gillison et al.[11] in which the commonest age group was 50-56 years, and in another study, the age group was 40-73 years with a mean age of 55 years.[12]
The present study has a men-to-women ratio of 1.8:1. Among the p16 positive cases, 63.7% were men, and 36.3% were women (n = 7), with a ratio of 1.7:1, which is similar to that of p16 negative cases. Wilson et al. and Smith et al. showed p16 positivity in 68.5% and 67% of men, respectively.[13,14]
The expression of p16 by IHC was observed most frequently in the SCCs of the oral cavity (45.4). Although it was thought that the oropharynx is the most commonly involved region in HPV HNSCC, oral cavity involvement has been on the rise in recent years, especially in younger individuals.[15,16] This association is due to physical contact and oral sex prevailing in this age group. Balaram et al. Kojima et al. Ostwald et al. found p16 positivity of 74%, 66%, and 62%, respectively, in oral SCCs.[17] Though these studies had a higher incidence of oral p16-positive SCCs, earlier studies showed more oropharyngeal involvement.
Out of 11 positive cases, six were non-keratinizing type (54.54%), and others were keratinizing. Chernock et al. studied 118 SCCs from the head and neck and found that all the non-keratinizing SCCs were positive for p16, and 69% were high-risk HPV DNA positive. In contrast, only 36% and 8% of the keratinizing SCC were positive for p16-positive and high-risk HPV DNA, respectively.[18] El Mofty et al. found 91.3% of HPV-positive cases were non-keratinizing, and most of them were of oropharyngeal origin.[19]
The histological grade is a means of quantifying the degree of differentiation by applying a set of histological criteria. In our study, the maximum number of p16 positive cases belonged to Grade 3 (54.5%). Grade 2 and 1 tumours constituted 36.4% and 9.1% of cases, respectively. In the present study, p16 expression had a significant correlation with the histological grade of the tumour (P = .0001). Our findings were in agreement with those of various studies that also observed p16 expression in higher-grade tumours, while a few studies showed opposite results.[20]
Recommendations
Routine staining for p16 IHC should be considered for all HNSCC, especially for poorly differentiated carcinomas seen in relatively younger individuals since they are more likely to be HPV-associated. Careful examination of the tonsil is recommended in all cases of unknown primary with nodal metastases. Rates of HPV-induced head and neck carcinomas are on the rise, so widespread vaccination is recommended to reverse the trend. Careful and extensive clinical examination is recommended as these carcinomas present in younger individuals with none of the usual risk factors and could go unnoticed. Further molecular techniques, such as PCR, could be done on p16-positive cases to characterise the HPV subtypes affecting the Indian population.
Conclusion
In the present study, we evaluated p16 expression in HNSCC since it is a marker of HPV infection. Our data revealed low p16 positive cases (14.67%) in HNSCC in our setup, therefore indicating the low prevalence of HPV in our region. These patients were younger and predominantly men. The oral cavity showed a higher incidence, followed by the laryngopharynx and oropharynx. The hypopharynx was not involved at all. Though these cases were of higher grade and mostly conventional non-keratinizing type, they still had better prognostic factors like a lesser stage, decreased nodal metastases, lesser DOI, a lesser degree of WPOI and no involvement of the cortical bone or overlying skin.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Approval was obtained from the Institutional Ethical Committee on AMH/DNB 041/11-18.
Informed consent
Informed consent has been obtained from the patients who met the eligible criteria.
Credit author statement
Hemalatha Kuppan participated in conceptualization, methodology, data duration, analysis and investigation, manuscript preparation and manuscript editing.
Swetha Lakshmi Narla participated in data analysis, investigation, manuscript preparation and editing.
Sheeba Jacob participated in conceptualization and supervision. All the authors have reviewed and approved the manuscript.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon request.
Use of artificial intelligence
No AI was used in this research.