
Abstract
Background and Aims:
Influenza, a lethal disease presenting with acute respiratory illness (ARI), has taken its toll on mankind through successive epidemics and pandemics. This study was conducted amidst the H1N1 influenza outbreak that struck central India in the latter half of 2022.
Materials and Methods:
Records of all patients admitted from 1 August 2022 to 7 September 2022 at a tertiary care centre of central India were reviewed and all patients admitted with acute respiratory failure who were suspected and tested for H1N1 influenza were included.
Results:
Thirty-two patients with respiratory failure were included in the study. They had a median age of 46 years, among which 50% patients were males. The median duration of illness was 6.8 (+/– 4.0) days, in which majority of patients were having fever (90.62%) and dyspnoea (93.75%). The median duration of hospital stay was nine days. Overall, 37.5% of the individuals had comorbidities, with diabetes mellitus (21.87%) and systemic hypertension (18.75%) being the most common. About 28.13% patients were confirmed positive for H1N1. The median oxygen saturation (SpO2) at presentation was 83% (with 13 patients having a saturation below 80% at room air) with a median respiratory rate of 25 breaths per minute. In 31 (96.8%) patients, chest imaging revealed an involvement in at least two zones. Eighteen (56.25%) patients had severe acute respiratory distress syndrome (ARDS). Overall mortality among the patients was 31.25%. All patients received full course oseltamivir.
Conclusion:
Our study H1N1 influenza virus-associated ARDS had a mortality rate of 31.25% with diabetes being a significant risk factor for severe disease and mortality.
Introduction
Influenza, a lethal disease presenting with acute respiratory illness (ARI), and at its worst, progressing to respiratory failure, caused by viruses belonging to the Orthomyxoviridae family, has been known to afflict mankind since as early as the time of Hippocrates in fifth century BC. Over the centuries, it has taken its toll on mankind through successive epidemics and rare pandemics. The last pandemic occurred in 2009, caused by the virus H1N1. Subsequently, it has resorted to local epidemics.[1]
This study was undertaken during the latest epidemic of H1N1 influenza in central India in the latter half of 2022, to assess the clinical profile of patients presenting to our hospital with pneumonia associated with respiratory failure and to assess their outcomes, as related data pertaining to central India is limited.
Materials and Methods
This is a record-based retrospective, single-centre study done during the previous outbreak of H1N1 influenza and includes patients admitted from 1 August 2022 to 7 September 2022 at a tertiary care centre of central India. The medical records of all these admitted patients with ARI who were suspected for H1N1 were initially selected. The patients were classified as possible, probable or confirmed cases of H1N1 influenza and all were treated as H1N1 pneumonia.[2] These patients underwent reverse-transcription polymerase chain reaction (RT-PCR) test. All patients were treated in influenza isolation unit. They received empirical antibiotic coverage in view of presumed lower respiratory tract infection, inotropic support for shock and ventilatory support as per patient requirements as well as full course of Oseltamivir.[3] Subsequently, patients who did not develop respiratory failure during the course of treatment were excluded from the study. All the remaining patients also underwent coronavirus disease 2019 (COVID-19) RT-PCR testing to rule out COVID-19-related acute respiratory distress syndrome (ARDS). The illness severity as per the patient’s clinical profile on day 1 of admission was defined as mild (only upper respiratory tract infection (URTI) symptoms, no shortness of breath or hypoxia), moderate (respiratory rate of ≥24/min or oxygen saturation (SpO2) between 90 and ≤93%) and severe (respiratory rate of ≥30/min or SpO2 <90%).[4] The Berlin ARDS criteria were used to define the severity of ARDS based on the partial pressure of oxygen/ fraction of inspired oxygen (PaO2/FiO2) ratios.[5] Additionally, all our patients with severe ARDS received parenteral steroids as per the DEXA-ARDS trial.[6] The data of remaining patients was subsequently analysed. The data extracted from the medical records of these patients was tabulated into Microsoft Excel (2019) for further analysis, including the calculation of medians and standard deviations to summarise the data and present the findings.
Results
A total of 32 cases were included in the study as described earlier who underwent H1N1 reverse-transcription polymerase chain reaction (RT-PCR) test at our hospital. Out of these, nine (28.13%) patients were found to be positive and 23 (71.87%) tested negative. The patients presenting had a median age of 46 (+/_ 16.10) years. Sixteen patients were males (50%) and the rest were females (
The clinicodemographic profile of patients with H1N1 pneumonia
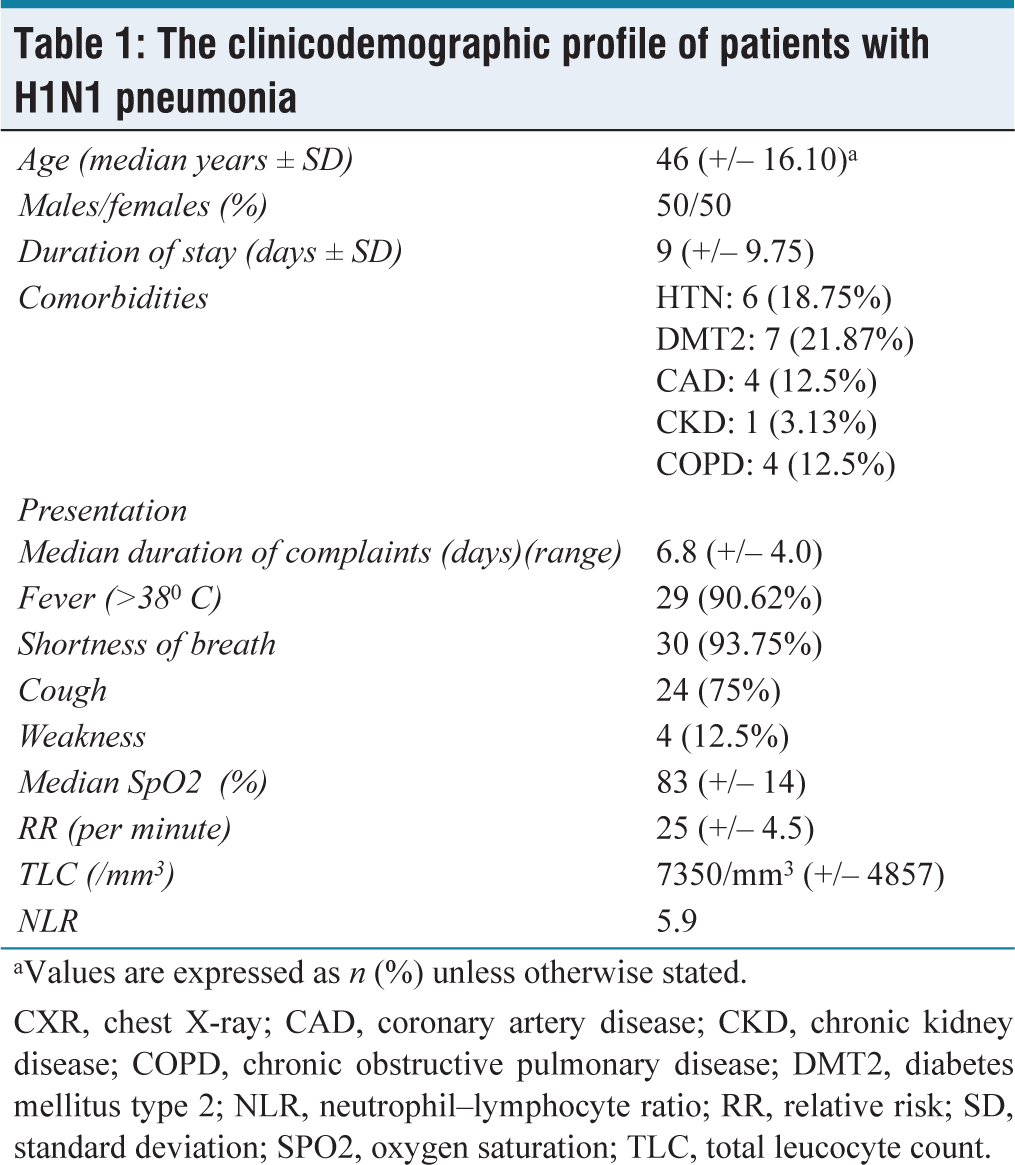
aValues are expressed as n (%) unless otherwise stated.
CXR, chest X-ray; CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DMT2, diabetes mellitus type 2; NLR, neutrophil–lymphocyte ratio; RR, relative risk; SD, standard deviation; SPO2, oxygen saturation; TLC, total leucocyte count.
The median duration of hospital stay was found to be nine (+/– 9.75) days. Among these patients, 12 (37.5%) patients had one or more comorbidities, diabetes mellitus type 2 (DMT2) being the topmost, followed by systemic hypertension (HTN), chronic obstructive pulmonary disease (COPD), coronary artery disease (CAD) and then chronic kidney disease (CKD). The median duration of complaints at presentation was 6.8 (+/– 4.0) days, during which majority patients had shortness of breath (93.75%) and fever (90.62%) at presentation, followed by cough (75% patients).
The median SpO2 and respiratory rate at presentation were 83% at room air and 25 breaths per minute, respectively, whereas, the median PaO2/FiO2 ratio at presentation was 66 (+/– 74.40). A median total leucocyte count (TLC) of 7350/mm 3 was seen among the patients during presentation with a neutrophil–lymphocyte ratio (NLR) of 5.9. A total of 43.75% patients had involvement of at least two zones on chest X-ray, 34.38% had four zones involved, 18.75% had three zones involved and only 3.13% had 1 zone involved.
In total 53.13% patients presented with respiratory failure with high (>6L/min) oxygen requirement. About 40.63% patients had low oxygen requirement (<6l/min) and 6.25% patients were put on mechanical ventilation (
The severity profile and outcomes of patients with H1N1 pneumonia
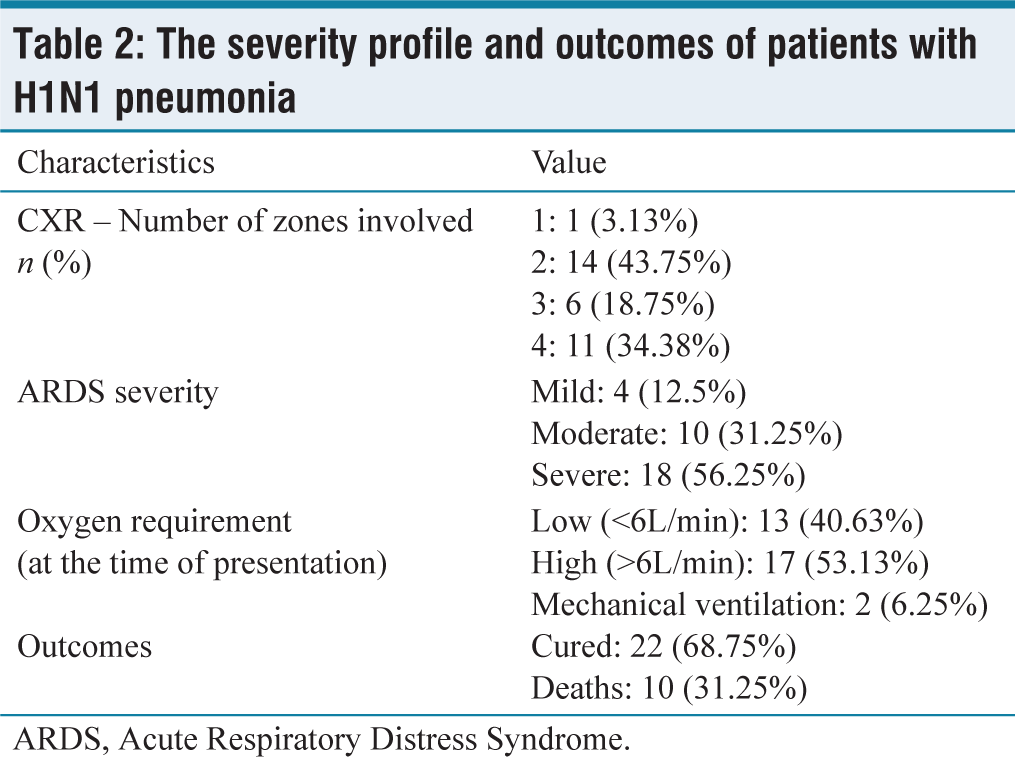
ARDS, Acute Respiratory Distress Syndrome.
Subsequently, 56.25% patients developed severe ARDS, while 31.25% had moderate ARDS and 12.5% had mild ARDS. All patients with mild and moderate ARDS were cured and discharged. Out of all patients with severe ARDS, 8 (44.44%) patients were cured and 10 (55.5%) died.
However, overall mortality in all patients with ARDS was 31.25%, with a cure rate of 68.75%. All patients received tablet oseltamivir 75 mg twice daily (BD) for five days and only patients with severe ARDS received parenteral steroids.
Discussion
Influenza, an ever-looming threat, has perpetually challenged global health systems with its recurring epidemics and occasional pandemics, leaving a profound impact on human health. Among its various strains, H1N1 stands out for its ability to cause severe ARI and has proven particularly devastating in past outbreaks. In the latter half of 2022, central India experienced a significant surge in H1N1 influenza cases, prompting urgent investigation due to limited regional data on its clinical manifestations and outcomes.
The most common presenting complaints were shortness of breath, fever and cough which were similar to another study from central India by Arbat et al.[7] which found cough, fever and additionally throat irritation to be the chief complaints. Likewise, the duration of hospital stay and that of chief complaints at presentation was also similar. Sardar et al.[8] found similar gender distribution, presenting complaints and duration of hospital stay in a study done in Kolkata. Another study by Sharma et al.[9] in central India during 2015 H1N1 outbreak found similar presenting complaints.
The presenting complaints and the positivity rate (28%) of our study were also similar to a study performed in Surat by Bhatt et al.[10] The positivity rate was also similar to another study performed by Singh et al[11] in Rajasthan in 2012. The findings were also similar to study by Siddharth et al.[12] done during 2010 H1N1 pandemic. Moreover, 29.58% of patients in their study tested positive, which was comparable to ours (28.13%). The presenting complaints and positivity rate were also similar to that in a study by Dwibedi et al.[13] from Odisha from 2009 to 2017.
The median TLC at presentation was 7350/mm3, which was very similar to that found by Kshatriya et al.[14] The NLR in our study was found to be 5.9 which was similar to a study done by Yıldız et al (8.8).[15]
In our study, nearly 53.13% presented with respiratory failure with high (>6L/min) oxygen requirement. About 40.63% had low oxygen requirement and 6.25% patients were put on mechanical ventilation. In our study, 12 patients (35.29%) had one or more comorbidities, DMT2 being the topmost, followed by systemic HTN, COPD, CAD and then CKD.
Overall mortality in all patients with ARDS was 31.25% in this study. This was found to be less compared to a study by Villar et al.[16] where the intensive care unit (ICU) mortality rate was found to be 42.7%. The difference may be explained by the fact that our study population consisted of younger patients (45.75 vs. 58 years) and wide variation in presenting PaO2/FiO2 range [66 (+/– 74.40) vs. 114 (+/– 40) mm Hg]. Our study included more proportion of females (50 vs. 29.4%) and also had a shorter duration of overall hospital stay (10 vs. 35 days).
In a study done in Kasturba Medical College Hospital, Manipal, India by analysing the medical records of 141 patients with H1N1 influenza, the study population had a mean age of 32±16.2 years. On the basis of disease severity, 53.2% of the patients were put on mechanical ventilation among which the mortality rate was found to be 29.1% which was found to be comparable to our mortality rate of 31.25%.[17]
A study done by Kumar et al.[18]in southern India to investigate the profile and outcomes of H1N1 patients admitted to the ICU showed a 62.5% mortality rate in patients developing respiratory failure due to H1N1 influenza among which serum procalcitonin level estimation was found as a useful tool in determining outcome; however, serum procalcitonin could not be done in some of our patients due to financial limitations.
A study conducted in France by Fuhrman et al.[19] during the 2009 H1N1 pandemic found the ICU mortality rate to be 20%, which is lower than the result of our study. This may have been due to the fact that many deaths occurring outside ICUs and outside hospitals were missed, and those with deaths indirectly due to their comorbidities were also not counted, as highlighted by the authors themselves in the study. Moreover, their study had only 49% of patients with ARDS (compared to ours with 100%), and 7% of their patients received extracorporeal membrane oxygenation (ECMO) (which was not available at our centre). Also nearly 94% of their cases were confirmed positive, as opposed to our 28.13%.
Our mortality rate was similar to that in a study done by Louie et al.[20] in California during the 2009 H1N1 pandemic; their ICU mortality was 24-42%. Compared to a study by Bellani et al.[21]in 2014 on patients with ARDS in ICUs), the prevalence of mild ARDS was found to be mild (30%; vs. 12.5% in our study), moderate (46.6%; vs. 31.25%) and severe (23.4%; vs. 56.25). ARDS was underdiagnosed in their patients as reported by themselves, which, had they been included may have significantly altered the results. The authors report that their convenience sample may have been prone to selection biases that may limit generalisability, which may also explain the differences in our results. The mortality rate in this study was better compared to another Indian study by Siddharth et al.[12] during the 2010 H1N1 pandemic in Northern India (31.25 vs. 54.9%). They attribute their high mortality to their hospital being a tertiary care centre, causing loss of crucial time.
Around, 14-46% of hospitalised patients died during the 2009 Influenza pandemic as per the WHO.
Conclusion
In conclusion, in our study the ARDS mortality rate was 31.25% which highlights the critical importance of demographic factors, such as the relatively young age of patients (median age 46 years) and the low prevalence of comorbidities, in shaping outcomes of H1N1 influenza in central India. These findings highlight the need for comprehensive, multi-centred studies across India to further elucidate the complex interplay between patient characteristics, disease severity and treatment outcome in H1N1-related pneumonia.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
EC/MGM/FEB-24/05.
Credit author statement
Data availability
Data available on request from the authors.
Use of artificial intelligence
During the preparation of this work, the authors did not use artificial intelligence.