
Abstract
Background:
A foetus-in-fetu (FIF) is a very rare congenital abnormality (incidence of 1 in 5.00,000 live births) in which a mass of tissue, a malformed foetus grows within the body of the foetus. It is an unusual cause of the abdominal mass in neonates. We here report a case of FIF in a newborn male for its rarity and interest in its evolution.
Case report:
A one-day-old male term neonate was referred for evaluation of abdominal mass. Antenatal ultrasonogram at 32 weeks of gestational age revealed a complex multi-septated cystic lesion with internal echogenic components. Clinical examination revealed a distended abdomen with an ill-defined mass filling the entire abdominal cavity. Plain X-ray abdomen revealed a mass on the right side of the abdomen with few long bone-like densities and few vertebrae. An ultrasonogram showed ill-defined hetero echoic lesions, measuring 10.9 × 11.1 Centimeters, with solid and cystic components and few calcifications in the mass. The CT scan of the abdomen showed an ill-defined mass lesion on the right side of the abdomen, measuring 11.3 × 6.6 × 9.9 Centimeters, with internal soft tissue, distorted long bones, and few vertebrae in the subhepatic region of the right hypochondrium. The 3-dimensional reconstruction of the CT scan confirmed the diagnosis of FIF. On laparotomy, the mass had a covering membrane attached to the adjacent abdominal wall and was connected by a cord-like structure with vessels. Excision of the mass was done in toto and the post-operative period was uneventful.
Conclusion:
FIF is considered a benign condition that causes mass effects on the adjoining organs and should be considered a differential diagnosis in neonates with abdominal distension.
Introduction
A foetus-in-fetu (FIF) is a very rare congenital abnormality (incidence of 1 in 5.00,000 live births) in which a mass of tissue, a malformed foetus grows within the body of the foetus. It is an unusual cause of the abdominal mass in neonates.
Case Report
A one-day-old male term neonate of birth weight of 3.2 kgs, delivered by labour natural, was referred to our hospital for evaluation of abdominal mass [Figure 1]. There was no history of twin pregnancy in the family. An antenatal ultrasonogram done at 31 weeks of gestational age showed a heterogeneous cystic lesion seen in the foetal abdomen with multiple echogenic foci, dilated bowel loops, dilated left pelvicalyceal system (PCS) (8mm) with the left megaureter. At 32 weeks of gestational age, an ultrasonogram was repeated, which revealed a complex multi-septated cystic lesion with internal echogenic components. Calcifications were noted in the lower abdominal cavity with a size of 6.8 × 5.2 cm. The left kidney was minimally distended. Hence, a provisional diagnosis of FIF was made.
Neonate with abdominal distension

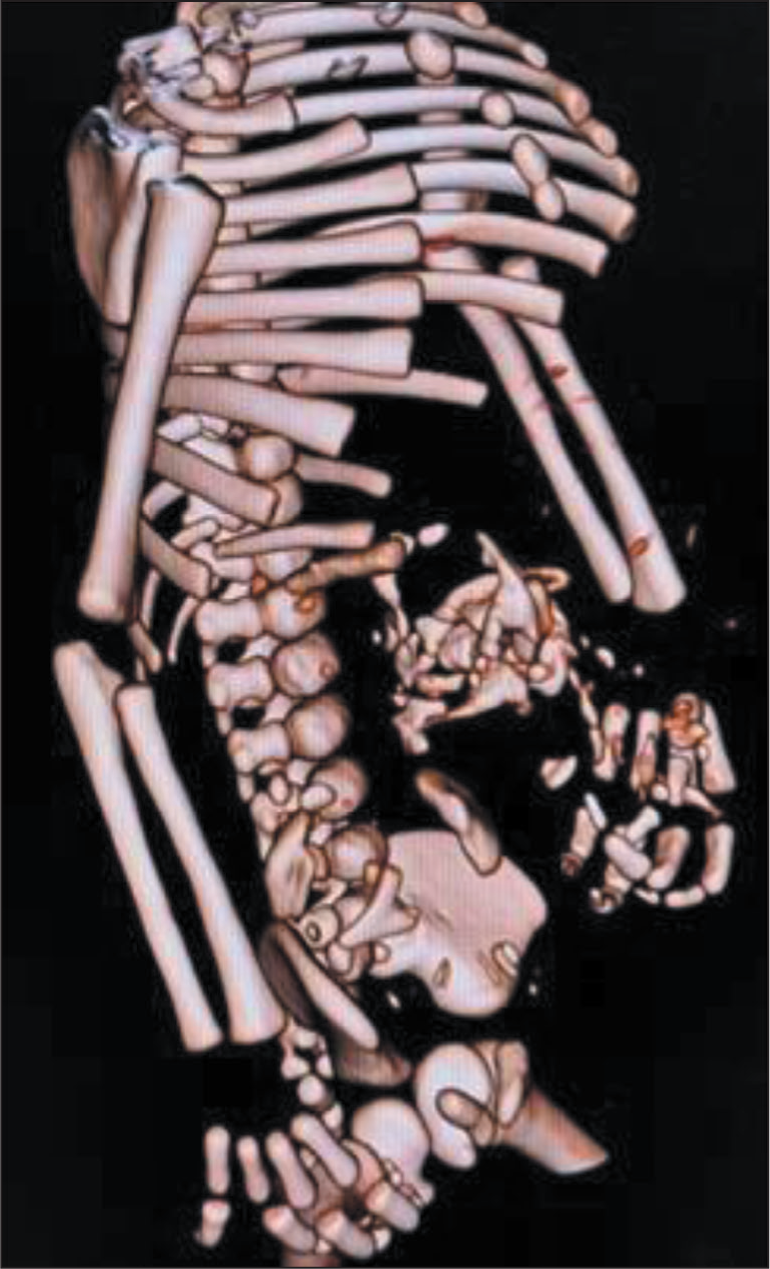
Post-natally, the baby passed meconium and urine within 24 hours. Clinical examination revealed a distended abdomen. On palpation, an ill-defined mass was felt filling the entire abdominal cavity, from the right hypochondrium, lumbar, and iliac areas extending to the left iliac region. A plain X-ray abdomen revealed a mass on the right side of the abdomen with few long bone-like densities and few vertebrae [Figure 2]. An ultrasonogram of the abdomen and pelvis showed ill-defined hetero echoic lesions, measuring 10.9 × 11.1 cm, with solid and cystic components and few calcifications in the mass. The left PCS was dilated. The CT scan of the abdomen showed an ill-defined mass lesion on the right side of the abdomen, measuring 11.3 × 6.6 × 9.9 cm, with internal soft tissue, distorted long bones, and few vertebrae in the subhepatic region of the right hypochondrium. The lesion was causing a mass effect over the adjacent structures and displacing the bowel loops anteriorly. The lesion was also found to cause a mass effect over the left ureter with upstream dilatation of the left ureter and left PCS. The 3-dimensional reconstruction of the CT scan confirmed the diagnosis of FIF [Figures 3 and 4]. Serum levels of Alpha-Feto-Protein (AFP), Beta-Human Chorionic Gonadotropin (β-HCG), and Lactate Dehydrogenase (LDH) were normal.
Plain X-ray showing right-sided mass with bony densities and vertebra-like structures

Three-dimensional reconstruction of CT scan in anteroposterior view showing bony components in the mass

Three-dimensional reconstruction of CT scan in lateral view showing bony components in the mass
The neonate underwent laparotomy through a transverse supraumbilical incision. A 15 × 8 cm mass retroperitoneally occupied the entire abdominal cavity. The mass had a covering membrane. A cord-like structure connected it with vessels to the aorta. On opening the covering membrane, the mass was found to have malformed limb buds with poorly differentiated fingers, toes, and some internal organs [Figure 5]. The cord-like structure was ligated and sectioned, and excision of the mass was done in toto [Figure 6]. The post-operative period was uneventful, and the neonate was discharged after 2 weeks.
Per-operative image showing the mass being delivered out of the covering membrane

Mass removed in toto with poorly differentiated limbs, fingers/toes, and internal organs

Discussion
FIF is an extremely rare congenital abnormality with an incidence of 1 in 5,00,000 live births and less than 200 are reported in medical literature worldwide.[1,2] It is usually retroperitoneal but may also present in the liver, scrotum, Pelvis, and cerebral ventricles. Different organs that can be seen inside the FIF are the vertebral column (91%), limbs (82.5%), CNS (52.5%), GIT (45%), and vessels (40%). The FIF complex is typically covered by a fibrous membrane resembling an amniotic membrane, contains some fluids resembling amniotic fluid, and a foetus suspended by a cord or pedicle. A true placenta is usually absent. The absence of an independent circulatory system explains the subsequent growth retardation.[3] FIF is usually a diamniotic monozygotic twin due to embryonic duplication or twinning. Now it is generally accepted that the presence of an axial skeletal system determines the distinction between FIF and teratoma. The presence of the vertebra indicates that the lesion has passed through the primitive streak stage and has developed like a foetus. In addition to the vertebra, the FIF possesses its amniotic membrane with a vascular connection usually to the mesenteric vessels of the host foetus. Retroperitoneal location with well-developed limbs, malformed viscera, and a benign nature differentiates it from mature teratoma. Two main theories are proposed for the pathogenesis of FIF.[4] (1) Teratoma Theory considers FIF as a highly differentiated form of mature teratoma and (2) Parasitic Twin Theory which proposes FIF as a parasitic twin foetus growing within its host twin usually of monozygotic diamniotic twin. The parasitic twin is usually anencephalic and lacks most internal organs. The parasitic twin usually will not be able to survive on its own. The 3-dimensional reconstruction of CT scan is superior in displaying vertebral column and long bone and is now the preferred diagnostic tool for FIF.[5] The distinction between FIF and teratoma is largely determined by whether an axial skeletal system is present indicating passing through the primitive streak stage of foetal development. Symptoms of FIF are usually due to the mass effect it causes on the adjoining organs. Treatment is complete excision and regular follow-up.
Conclusion
FIF is considered as a benign condition, that causes mass effects on the adjoining organs and should be considered as a differential diagnosis in neonates with abdominal distension.
Footnotes
Acknowledgements
The authors would like to thank the parents of the neonate described here.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Not applicable.
Patient consent
Patient consent obtained in written format for the publication of data and phographs.
Informed consent
Informed consent has been obtained in written form for the publication of the data and photographs.
Credit author statement
All the authors have participated sufficiently in the work and take public responsibility for appropriate portions of the content.
All the authors read and approved the final version before submission.
Data availability
The data that support the findings of this case report are available on request from the corresponding author.
Use of artificial intelligence
Not used in this study.