
Abstract
Background:
Paget’s disease is rare and arises from the apocrine glands of skin. Perianal Paget’s disease is very rare form of extramammary Paget’s disease.
Method and Results:
Patient presented with complaints of perianal itching which on examination had patchy depigmented nodular skin in perianal region. Biopsy showed Paget’s cells, and immunohistochemical staining was positive for CK7, CEA and GCDFP-15, confirming the diagnosis of primary perianal Paget’s disease. Further, patient was staged and was planned for surgery and underwent wide local excision of perianal skin preserving internal and external anal sphincters. Reconstruction of the defect was completed with a local flap.
Conclusions:
Surgery remains most effective and only curative option for perianal Paget’s disease. As it is a rare disease, a high degree of suspicion is required for early diagnosis and treatment.
Keywords
Paget’s disease is an apocrine gland tumour and considered as an intraepithelial adenocarcinoma which was first described by Sir James Paget in 1874 in the breast.[1] The presence of Paget’s cells which are malignant intraepithelial adenocarcinoma cells within epidermis of skin is hallmark of Paget’s disease.[1] The first case of perianal Paget’s disease (PPD) was reported in 1893 by Darier and Couillard. Paget’s disease occurs most commonly in breast (nipple, areola, skin). Most common extramammary site is vulva, accounting for 65% of all extramammary Paget’s cases followed by skin of perianal region, scrotum, penis, and axilla.[2] PPD is a rare form of extramammary Paget’s disease with only a few cases reported and its precise incidence is unknown.[2]
Depending upon cause, it is divided into primary—arising from the skin and secondary—due to cutaneous metastases of anorectal or genitourinary malignancy. Average age at the diagnosis is 63 years with female preponderance and predominately occurring in Caucasians.[2] Patients usually present with perianal itching, pain and rarely with burning, tenderness and oedema.[2] The diagnosis is confirmed by histopathology through the presence of specific tumour cells called Paget’s cells. Because of rarity of the disease, there is no large study available regarding optimum treatment, but general consensus is that surgical resection with clear margins is the standard of care. We report here a case of PPD managed by surgical resection and reconstruction at our centre.
A 69-year-old female patient came to our hospital in October 2023 with complaints of itching around the perianal region for the last month. The patient did not have any history of rectal bleeding, change in bowel habits or weight loss. Local examination revealed nodular skin thickening with patchy depigmentation over the nearby right perianal region. Patchy depigmentation was also noted over the left perianal skin. The lesion had a butterfly-shaped configuration sparing the anal canal skin [Figure 1A]. Per rectal examination was normal with normal sphincter tone. No enlarged inguinal lymph nodes were detected.
These lesions are routinely treated as benign skin conditions but are refractory to local treatments. Therefore, any such perianal lesion that persists despite local medical treatment given for eczema should undergo a biopsy to rule out Paget’s disease. The differential diagnoses are superficial spreading melanoma, Bowen’s disease, neuroendocrine carcinoma, mycosis fungoides, psoriasis, leucoplakia, eczema and fungal infection. Another important differential diagnosis is pagetoid effect which is intra-epidermal spread of visceral carcinoma. The patient underwent a tissue biopsy, which indicated extramammary Paget’s disease. This diagnosis was confirmed through immunohistochemistry, revealing positive markers for CK7, CEA (carcinoembryonic antigen), and GCDFP-15 (Gross cystic disease fluid protein 15), while CK20 and CDX2 were negative. Immunohistochemical profile is suggestive of primary Paget’s disease over secondary spread. Immunohistochemistry panel (CK7, CK20, GCDFP-15 and CDX2) is useful to predict underlying malignancy. GCDFP15 is only expressed in primary PPDs as compared to CDX2, which is expressed in secondary pagetoid spread by rectal adenocarcinoma.[3] In addition, high molecular weight cytokeratin (CK5/6, P40, P63) is expressed in squamous intraepithelial neoplasm and S-100P/HMB45 is expressed in melanoma.[3] The role of immunohistochemistry is not only limited to diagnosis purposes but also in predictive marker for underlying malignancy.[3]
Patient was further investigated with magnetic resonance imaging (MRI) pelvis with contrast which showed altered signal intensity thickening in perianal region on right side with max thickness of 3 mm with post-contrast enhancement. Staging was completed with contrast-enhanced computed tomography (CECT) upper abdomen and chest which was unremarkable. The patient also underwent a screening colonoscopy to exclude lower gastrointestinal (GI) malignancy. All blood investigations were normal.
After written informed consent, she underwent surgery. Patient was placed in lithotomy position under general anaesthesia. Surgery consisted of wide local excision of perianal skin lesion with 5-10 mm margin [Figure 1D]. The perianal skin was excised as marked in Figure 1A up to anal verge preserving external and internal sphincters. The defect size was approximately 7×6 cm on right side and 5×3 cm on left side. Using a handheld Doppler, a good perforator was found around 3 cm lateral and posterior to the edge of the defect on the right side. A V-Y advancement flap was planned based on this perforator (Figure 1D shows the marking of the V-Y flap centred on the identified perforator). The flap was raised subfascially, and the perforator was carefully identified and preserved. The V-Y flap could be advanced till the midline both anterior and posterior to the anus. On the left side, the defect was narrower, and the skin was undermined (marked with multiple ‘x’ in Figure 1D) in order to be advanced and sutured with the anal mucosa. However, anteriorly, the defect was wider and could not be closed in this fashion. Hence, a posteriorly based transposition flap was used to reconstruct the skin defect between the anal opening and the introitus. The transposition flap was sutured to the V-Y flap from right side in the midline [Figure 1E]. Patient had an uneventful post-operative recovery. She was discharged on sixth post-operative day, on a normal diet and lubricant laxative.
(A) Perianal skin excoriation (R>>L). (B and C) Paget’s cells are large, hyperchromatic with pale cytoplasm and prominent nucleoli. (Haematoxylin and eosin; (B) 40×; (C) 400×; (D) surgical defect after resection; (E) Post-reconstruction; (F) after four months
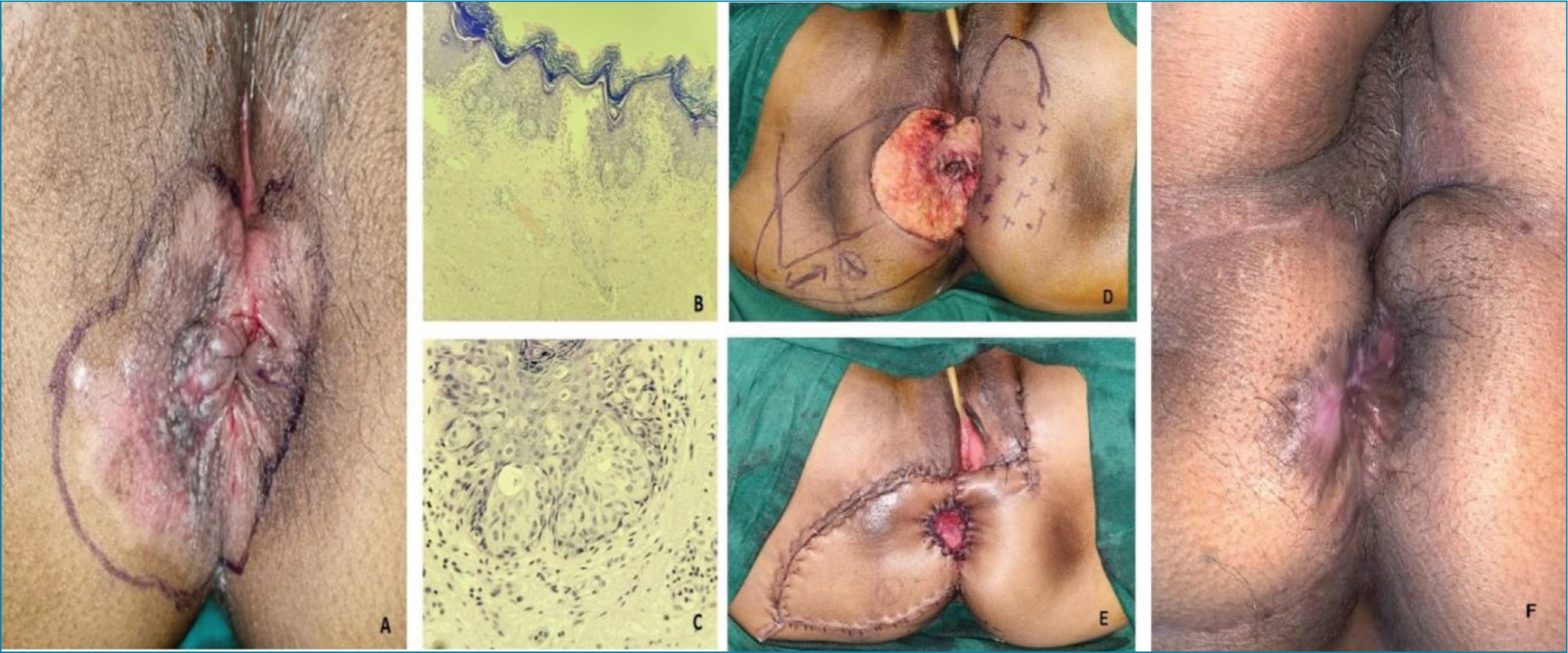
Final histopathology report confirmed the diagnosis of PPD without invasive malignancy and all margins and base free of tumour. Patient has been under follow-up since then without any locoregional symptoms. Figure 1F shows the outcome after four months.
It is often challenging to identify margins for surgical resection so intraoperative multiple biopsies may be done to identify the margin involvement. Other treatment options for PPD have been suggested for patients not fit for surgery or in cases who refuse surgery. For patients with PPD who are unfit for surgery or decline it, alternative treatments include radiotherapy at doses of 50 Gy or higher[4], and topical therapies such as 5-fluorouracil (5FU), retinoic acid, or imiquimod 5% cream, either alone or in combination. Photodynamic therapy is also a potential option.
Primary PPD is a rare entity. Diagnosis is usually delayed. A high degree of suspicion and knowledge about the existence of such an entity is required for early diagnosis. Biopsy can accurately diagnose the disease. Surgery is curative.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed consent
Informed consent taken.
Ethical approval
Not required.
Credit author statement
Sharma SV, Dave A, Dave VN were involved in conceptualization & writing the original draft. Shah HJ was involved in review & editing of the manuscript.
Data availability
Not applicable.
Use of artificial intelligence
None.