
Abstract
Background:
Rhinosporidiosis (RS) is a chronic granulomatous infection that primarily impacts the mucous membranes of the nose and nasopharynx. The diagnosis of RS is usually done by the clinical presentations and confirmed by histopathological study. The diagnosis of RS may be delayed when the extra-nasal sites are involved. Wide and complete excision of the lesion by thorough electro-cautery is usually recommended.
Conclusion:
Rhinosporidiosis (RS) is an enigmatic disorder with a debatable mode of infection and the nature of the etiological agent. Atypical and extra-nasal cases of RS should be carefully diagnosed, managed, and monitored throughout their clinical course.
Introduction
Rhinosporidiosis (RS) is a chronic granulomatous condition affecting the nasal cavity, caused by Rhinosporidium seeberi.[1] Over recent decades, there has been debate about the exact nature of the etiological agent, as microorganisms are difficult to isolate and culture microbiologically.[2] RS usually affects the mucous membrane of the nose and nasopharynx but sometimes involves the lacrimal sac, conjunctiva, lips, palate, vulva, larynx, maxillary sinus, trachea, skin, penis, vulva, and vagina.[3] The clinical presentation of RS is a reddish or pinkish, friable, polyp-like mass seen inside the nasal cavity and nasopharynx. However, sporadic involvement may be found in some extra-nasal sites.[4] The extra-nasal sites often make a challenge for diagnosis for clinicians as in this case. The most successful treatment of RS includes wide excision with cauterisation of the base.[4] The medical treatment includes Dapsone which may be added following surgical procedure to prevent recurrence.[4] Here, we present a case of giant RS arising from the nasopharynx protruding towards the oropharynx and oral cavity.
Case Report
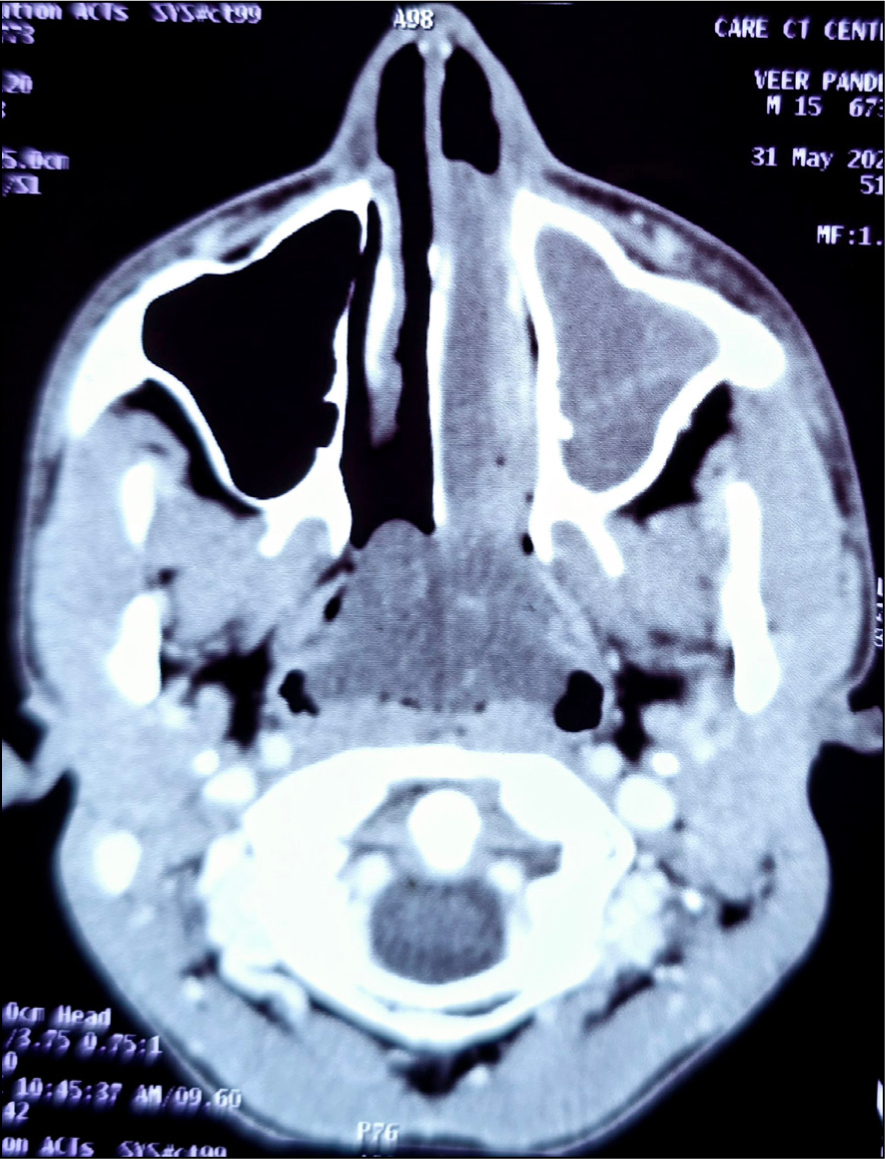
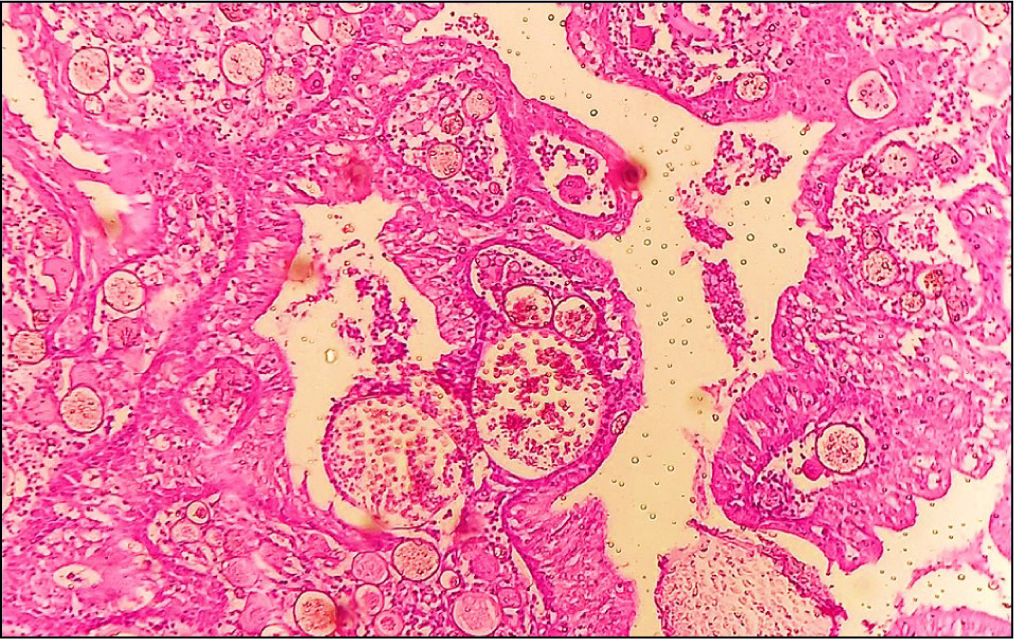
A 25-year-old male patient attended the outpatient department of otorhinolaryngology with a chief complaint of swallowing difficulty and sensation of foreign body in the oral cavity and oropharynx for three months. He was a milkman by profession, staying in a rural village. He also had an occasional irritating dry cough. Examination of the oral cavity showed a lobulated reddish-pink mass [Figure 1] over the tongue coming from the oropharynx. The patient also presented regression of the mass from the oral cavity during swallowing or taking food. The mass was non-pulsatile and did not bleed during the physical examination. The patient had no systemic symptoms, nasal block, nasal discharge, or epistaxis. Anterior rhinoscopy revealed no abnormality. With the help of a tongue depressor, the oropharynx was examined, and found the origin of the mass from the nasopharyngeal region. Provisionally, the lesion was provisionally diagnosed as nasopharyngeal RS. A small piece of tissue from the mass in the oral cavity was taken for biopsy. The histopathological analysis revealed many double-walled sporangial cysts in the stroma, which contained endospores at various developmental stages, surrounded by polymorphonuclear leukocytes and eosinophils. The final diagnosis of RS was established. A contrast-enhanced CT scan of the face and neck showed a large, lobulated soft tissue mass originating from the nasopharynx, extending into the left nasal cavity and oral cavity via the oropharynx [Figure 2]. The mass was excised completely under general anaesthesia and the area of attachment was cauterised. The anaesthetist had carefully done intubation by not traumatising mass. The gross specimen was a polypoidal soft friable mass with an outer surface appearing pinkish, and smooth surface. There were small yellowish spots scattered on the surface of the mass. The histological analysis supported the previous diagnosis by revealing the same microscopic characteristics [Figure 3]. A tissue sample stained with Periodic Acid Schiff (PAS) showed prominent sporangia within a fibromyxoid stroma. Following surgery, the patient was put on 100 mg of Dapsone (diaminodiphenylsulphone) once daily. He is currently on a three-month follow-up and has not seen any recurrence.
A large reddish mass of Rhinosporidiosis protruding into the oral cavity

A contrast-enhanced CT scan showing a radio-opaque mass of Rhinosporidiosis in the nasopharynx, left nasal cavity, and oropharynx
Photomicrograph showing sporangia with endospores and inflammatory cells (H&E, ×100)
Discussion
RS is a chronic and localised infection of the mucus membrane that manifests with polypoidal masses at the nose, nasopharynx, oropharynx, larynx, ear, skin, and even genitalia in both genders.[5] Important infection reservoirs include soil and water.[5] Endospores are injected into the mucosa of the nasal cavity through traumatic inoculation, where these develop sub-epithelially and rupture later on to release sporangia into surrounding tissues.[6] RS is a worldwide illness that affects both humans and animals. It is most prevalent in hot, tropical temperatures found in endemic areas such as East Africa, parts of America, India, and Sri Lanka. It is also widespread among expatriate populations in the West.[7] In a few Indian states, including Tamil Nadu, Kerala, Odisha, West Bengal, and Chhattisgarh, RS is hyperendemic.[8] People who bathe in stagnant, murky waters, as well as, those who work in paddy fields, frequently have RS. The patient had a habit of bathing regularly in pond water. The precise nature of Rhinsporidium is debatable and poorly understood. Swimming in ponds or stagnant water, diving, and mucous membrane trauma are significant risk factors for developing RS.[9] It is unclear and controversial what Rhinosporidium seeberi’s precise nature is. As of right now, fish and amphibian pathogens are included in the new DRIP clade (Dermatocystidium, rosette agent, icthyophonus, and psorospermium) that Rhinosporidium seeberi belongs to.[10]
The important clinical presentations of RS are bleeding polypoidal mass, nasal blockage, and breathing difficulty. It could affect the larynx, trachea, conjunctiva, bone, skin, lip, palate, uvula, penis, vagina, scalp, etc. When more than one nasal site is affected, diagnosis of RS is typically late.[11] Males are four times as likely as females to have RS.[4] In this case, the RS was arising from the nasopharynx that extends towards the oropharynx and oral cavity. Here, clinicians should keep in mind the differential diagnoses of mycotic granuloma, nasopharyngeal angiofibroma, and nasopharyngeal carcinoma.[11] For managing the RS, accurate occupational history and personal history are essential. It is necessary to distinguish RS from other organisms when it appears as an oral oropharyngeal mass. A report featured an antrochoanal polyp and a visible oropharyngeal or oral lump that appeared to be juvenile angiofibroma.[12] Consistent hypertrophic tonsillitis can be mistaken with oropharyngeal or oral cavity RS due to its involvement site, dysphagia symptoms, persistent throat irritation, and yellow pus patches on the surface. A vascular benign tumour that originates in the nasopharynx and can spread into the oral cavity, nasopharyngeal angiofibroma mimics radiologically and clinically RS in this instance.[12] However, nasal obstruction and recurrent nasal bleeding are often seen in the nasopharyngeal angiofibroma, but these symptoms are absent in this case. Nasopharyngeal angiofibroma may extend to adjacent paranasal sinuses. The absence of extension into paranasal sinuses helps to differentiate RS from polyps and papilloma.[13] To distinguish nasopharyngeal malignancy from RS, consider the malignancy’s rapid progression, destructive growth, persistent pain, and the presence of metastatic neck lymph nodes at diagnosis. A contrast-enhanced CT scan is used to assess the extent of the lesion. On this scan, the mass associated with RS appears as a lobulated soft tissue mass with moderate to minimal enhancement.[13] In this case, contrast-enhanced magnetic resonance imaging (MRI) was performed to define the extent of the mass, revealing it as an intensely enhancing lesion compared to the surrounding tissues, likely due to the rich blood supply in rhinoscleroma (RS). In contrast, MRI of sinonasal malignancies typically shows a heterogeneous appearance with areas of necrosis, while inverted papillomas exhibit a cerebriform pattern.[13] The histological examination confirms the diagnosis of RS. Microscopic analysis reveals subepithelial, thick-walled, cysts or sporangia containing numerous daughter spores at various stages of development.[14] After the endospores transition from the trophozoite stage, they develop into sporangia.[14] These features can be observed with routine haematoxylin and eosin staining, as well as, with methenamine silver and PAS stains. The lesion typically shows granulation tissue with lymphocytes, plasma cells, focal aggregates of histiocytes, and neutrophils. Additionally, fibrosis, granulomatous reactions, and pseudocystic abscess formations are also characteristic of this condition.[14] The treatment of choice for RS is surgical excision. The rigid nasal endoscope can be used to ensure the complete excision of the mass under vision. The cauterisation at the base of the lesion is preferred following surgical excision. Limited cauterisation may cause bleeding, recurrence, and dissemination.[7] However, the RS extending into the oropharynx and oral cavity needs a more extensive approach. Dapsone can be used as an adjunct to the surgical excision as it prevents the maturation of the sporangia and enhances the fibrosis.[15] Coblation is an important surgical tool for resection of the recurrent RS. Coblation-assisted surgery enables the surgeon to get better resection of the lesion by constant suctioning along with minimum lateral thermal injury.[16] Coblator-assisted surgical excision of the RS along with medical treatment by Dapsone 100mg once daily for six months provide promising results in point of decreasing the recurrence.[17]
Conclusion
RS is an enigmatic disorder with a debatable mode of infection and the nature of the etiological agent. The diagnosis of RS depends on the clinical presentations and the histological picture of the mass that demonstrates the sporangia. It is well-known for having a greater likelihood of recurrence. Clinicians may see an unusual presentation of RS such as a giant oral mass with its clinical course. Atypical cases of RS should be carefully diagnosed, managed, and monitored throughout their clinical course.
Footnotes
Acknowledgements
Author is thankful to Swagatika Swain for the language corrections of the manuscript.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Patient consent
The author has obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Institutional ethical committee approval number
The study did not require approval from the Institutional Ethical Committee, and therefore, no specific approval number has been provided.
Informed consent
Consent form was taken and duly signed by of patient.
Credit author statement
SKS: Conception, design, data analysis, data interpretation, drafting and final approval of the manuscript.
Data availability
Data openly available in a public repository that issues datasets with DOIs.
Use of artificial intelligence
Artificial Intelligence was not used in any part of the study.