
Abstract
Introduction:
The Oxygen Saturation Index (OSI) has emerged as a non-invasive monitoring alternative to the traditional Oxygenation Index (OI) in neonates with respiratory diseases requiring mechanical ventilation. This study aims to evaluate the utility of OSI over OI, given the critical need for improved monitoring strategies in neonatal intensive care units (NICUs).
Methods:
A prospective observational study was conducted in the NICU, Department of Paediatrics, from August 2022 to February 2024. Fifty neonates diagnosed with various respiratory diseases requiring mechanical ventilation were included. OSI and OI were calculated using non-invasive and invasive parameters, respectively. The correlation between OI and OSI was assessed using Pearson’s correlation coefficient, and a regression model was developed to predict OI from OSI measurements.
Results:
The study found a moderate positive correlation (r = 0.491, p < .001) between OI and OSI, with the correlation strengthening within the oxygen saturation range of 85%–95%. A linear regression model (OSI = 0.391*OI + 4.2341) was developed, facilitating the estimation of OI from OSI measurements. This model underscores the potential utility of OSI in neonatal respiratory monitoring.
Conclusion:
OSI presents as a viable, non-invasive alternative to OI for monitoring neonates with respiratory failure. The significant correlation and the development of a predictive regression model highlight OSI’s potential to improve clinical monitoring and decision-making in NICUs, potentially reducing the need for invasive procedures.
Keywords
Introduction
The utility of the Oxygen Saturation Index (OSI) over the Oxygenation Index (OI) in the monitoring of neonates with respiratory diseases is underscored by the critical need to improve neonatal care outcomes and enhance the efficiency of healthcare delivery systems globally.[1] The neonatal mortality rate (NMR) is a pivotal indicator of healthcare quality and country development, with respiratory failure in neonates requiring mechanical ventilation being a significant concern. The estimated incidence of this condition is approximately 18 per 1000 live births, emphasising the importance of effective monitoring strategies.[2]
Historically, the OI has been a cornerstone in the clinical management and evaluation of neonatal respiratory diseases.[3] However, its limitations, including the need for invasive arterial catheters for arterial blood gas (ABG) sampling, increased cost, and the intermittent nature of oxygenation status measurements, necessitate the exploration of alternative monitoring methods. The OSI, a non-invasive monitoring parameter, has emerged as a promising alternative, offering several advantages over OI.[4] These include the elimination of recurrent ABG sampling, reducing the risk of phlebotomy-induced iatrogenic anaemia, and the need for indwelling catheters, thereby decreasing sepsis risk in neonatal intensive care units (NICUs). OSI enables continuous monitoring of oxygenation status, potentially leading to better clinical outcomes and reduced healthcare costs. Studies have shown a strong correlation between OSI and OI in neonates, indicating the reliability of OSI as a non-invasive measure for assessing the severity of hypoxic respiratory failure and lung injury.[5,6] The evidence supports the utility of OSI as a non-invasive, cost-effective alternative to OI for monitoring hypoxic respiratory failure in neonates on mechanical ventilation. The implementation of OSI in clinical settings could lead to significant improvements in neonatal care, particularly in resource-constrained environments. Further research is warranted to explore the full spectrum of OSI’s benefits and its potential impact on neonatal health outcomes and healthcare systems worldwide.
This study aims to critically evaluate the OSI for its potential to replace the more traditional and invasive OI in monitoring neonatal respiratory failure. By analysing 100 paired readings from neonates with various respiratory diseases, the study aims to quantify the correlation between OI and OSI, validate the OSI’s effectiveness, and develop a regression model to aid clinicians in the NICU. This could potentially lead to improved respiratory management protocols and better outcomes for neonates requiring mechanical ventilation.
Materials and Methods
Study Design and Setting
This prospective observational study was conducted at the NICU, Department of Paediatrics from August 2022 to February 2024. The study aimed to evaluate the utility of the OSI compared to the traditional OI in monitoring neonates with respiratory diseases requiring mechanical ventilation.
Inclusion Criteria
Neonates (both preterm and term) admitted to the NICU, Department of Paediatrics, between August 2022 and February 2024.
Neonates diagnosed with respiratory diseases requiring mechanical ventilation, including but not limited to Meconium Aspiration Syndrome (MAS), Congenital Pneumonia, Respiratory Distress Syndrome (RDS), and Persistent Pulmonary Hypertension of the Newborn (PPHN).
Exclusion Criteria
Neonates with cyanotic congenital heart disease.
Neonates who had received blood transfusions prior to study enrollment.
Neonates diagnosed with metabolic acidosis.
Neonates admitted to the NICU for non-respiratory reasons that require mechanical ventilation.
Sample Size
For the purpose of this study, a total sample size of 50 neonates was selected using convenience sampling. This approach facilitated the efficient recruitment of participants meeting the study criteria within the specified study period.
Data Collection
Demographic and clinical data were systematically collected using a predesigned proforma. The data included but were not limited to age, sex, birth weight, gestational age, and the specific respiratory condition diagnosed. Clinical management details, including ventilatory support parameters and duration of mechanical ventilation, were also recorded.
Measurement Procedures
Oxygen saturation (SpO2) was continuously monitored using a MASIMO RADICAL 7 Pulse Oximeter (Masimo Inc, Irvine, CA), ensuring a stable 60-second waveform before recording to avoid movement artefacts and hemodynamic instability. SpO2 readings were taken immediately before ABG sampling to mitigate the potential for prick-induced hypoxia. Under strict aseptic conditions, 0.5 cc of arterial blood was collected in a pre-heparinised syringe, preferably from a preductal site, and promptly sent for blood gas analysis using an ABG analyser.
Ventilator settings, including Peak Inspiratory Pressure (PIP), Positive End Expiratory Pressure (PEEP), Inspiratory Time (Ti), Total Time (Tt), and the Fraction of Inspired Oxygen (FiO2), were documented for each neonate. These parameters were used to calculate the Mean Arterial Pressure (MAP) as per the formula: MAP = [(PIP - PEEP) × Ti + PEEP] / T(total).
Calculation of Oxygenation Indices
The OI and OSI were calculated using the formulas:
OI = (MAP × FiO2 × 100) / PaO2 OSI = (MAP × FiO2 × 100) / SpO2
These indices provided quantitative measures of the neonates’ oxygenation status and the efficiency of gas exchange, serving as critical indicators for the severity of respiratory failure.
Statistical Analysis
Data were analysed using appropriate statistical methods to assess the correlation between OI and OSI, their predictive value for clinical outcomes, and the utility of OSI as a non-invasive alternative to OI. Correlations were evaluated using Pearson’s correlation coefficient, and regression analysis was used to further explore the relationship between these indices and clinical outcomes.
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Review Board (IRB). All procedures were carried out in accordance with ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments. Informed consent was obtained from all individual participants’ legal guardians included in the study.
Results
Participant Demographics and Clinical Characteristics
Our study population consisted of 50 neonates admitted to the NICU requiring mechanical ventilation for various respiratory diseases. Among these, a higher preponderance of preterm neonates was noted, with 29 preterm babies compared to 21 term babies. The gender distribution was predominantly male, with 37 male neonates and 13 female neonates included in the study [Table 1].
Demographic data
Prevalence of Respiratory Conditions
A significant variety of respiratory conditions necessitating mechanical ventilation were documented. The frequency of conditions presented as follows: Hyaline Membrane Disease (HMD) was observed in 24 neonates, MAS in 14, pneumonia in 9, and RDS in 3 [Table 2].
Frequency of respiratory conditions
Correlation Between Oxygenation Indices
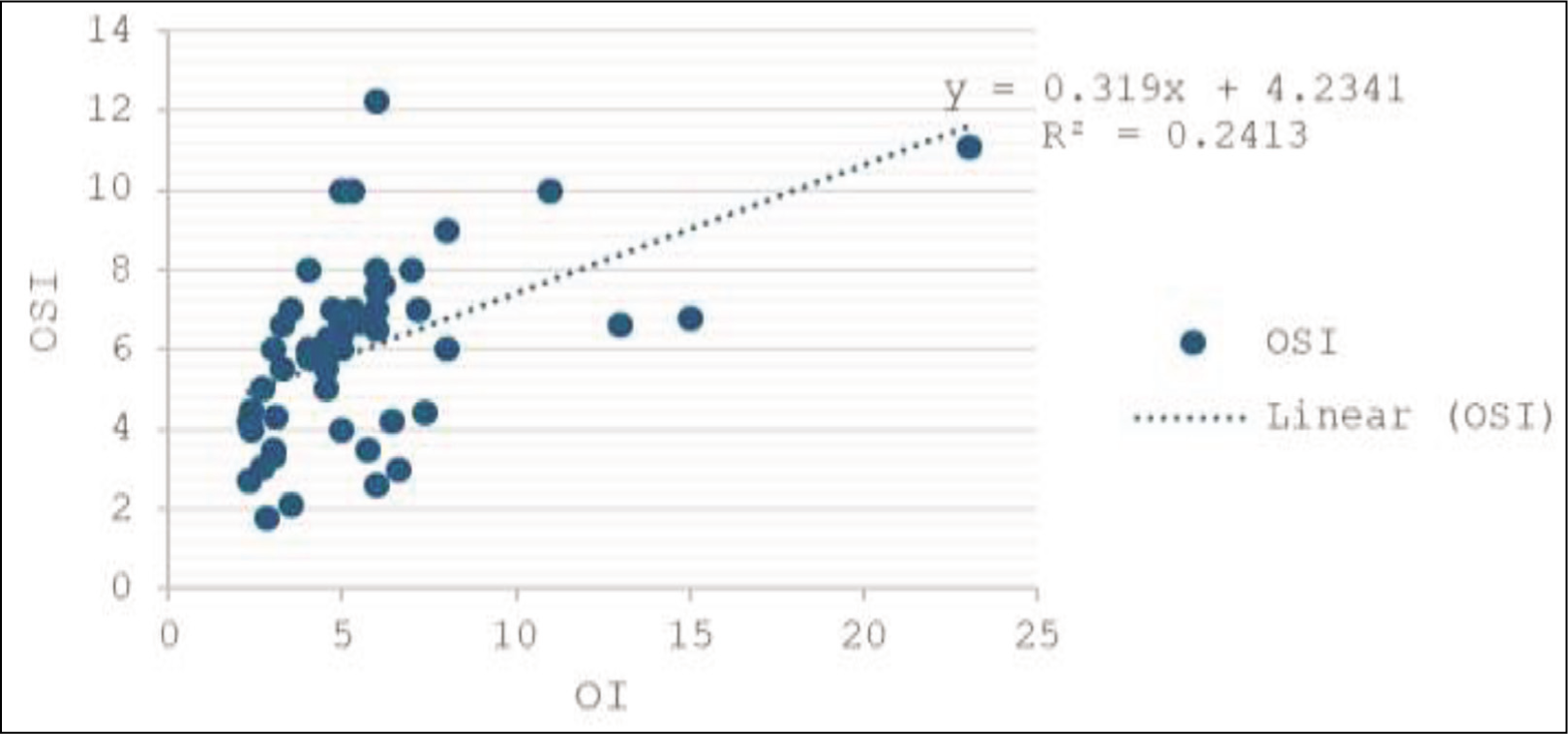
The core of our study revolved around the analysis of the OI and OSI across 100 paired readings. A Pearson’s correlation coefficient (r) of 0.491 indicated a moderate positive correlation between OI and OSI, which was statistically significant (p < .001). This correlation notably strengthened within the critical oxygen saturation range of 85%–95%, suggesting increased reliability of OSI in this interval. The relationship between these indices is graphically represented in a scatter plot, identified as Figure 1, which illustrates the trend of correlation and provides a visual representation of the data spread and linearity.
Regression Analysis
The linear regression model derived from our data resulted in the equation OSI = 0.391*OI + 4.2341, providing a method to estimate one index based on the other. This predictive model is pivotal for clinicians who require a quick assessment of the neonate’s respiratory status without the invasiveness of frequent arterial blood sampling.
The moderate yet significant correlation between OI and OSI could support the integration of OSI into routine clinical monitoring protocols for neonates with respiratory failure in the NICU, thereby reducing the need for invasive blood gas analyses.
Discussion
The integration of the OSI as a non-invasive monitoring tool in NICUs marks a significant advancement in the management of respiratory failure in neonates.[6] Our research builds upon the growing body of evidence suggesting the OSI’s reliability and utility across various patient populations, including those with acute respiratory distress syndrome (ARDS) and neonates experiencing respiratory failure. The concept of non-invasive monitoring in neonatal care is not novel; however, the quest for a reliable and safe index like OSI has gained momentum due to the inherent risks associated with invasive procedures in this vulnerable population.[7–9] Invasive measures, while informative, are fraught with potential complications including iatrogenic anaemia and the heightened risk of sepsis within NICUs, underscoring the need for alternative monitoring strategies. The OSI, calculated based on non-invasively obtained parameters, emerges as a promising candidate, offering a glimpse into the neonate’s oxygenation status without the associated risks of direct arterial intervention.
Our study centred on neonates with various respiratory conditions, found a significant correlation between OSI and OI, especially within the oxygen saturation range of 85%-95%. This finding is in concordance with previous studies, such as those cited in the European Respiratory Journal and Neonatology, which highlight OSI’s correlation with OI and its potential in predicting clinical outcomes in ARDS patients and continuous monitoring in neonates with Congenital Diaphragmatic Hernia (CDH), respectively.[5,10] The significant linear correlation reported between OSI and OI (r = 0.73; p = .002) in ARDS patients, along with the strong correlation coefficients ranging from 0.88 to 0.93 in a study involving 636 measurements from 68 neonates across different respiratory failure conditions, further attests to OSI’s reliability as a monitoring tool.[5,6] Furthermore, the utility of OSI extends beyond neonatal care, as demonstrated by its applicability in assessing the severity of Paediatric Acute Respiratory Distress Syndrome (PARDS) and its prognostic value in ICU mortality among mechanically ventilated patients. These findings suggest that OSI’s relevance spans different age groups and clinical scenarios, offering a versatile tool in the management of respiratory distress.[11,12]
Our contribution to the existing literature is the development of a linear regression model that facilitates the estimation of OI based on OSI values. This model represents a crucial step forward, potentially enabling clinicians to estimate invasive OI values from non-invasive OSI measurements, thereby reducing the need for invasive procedures. This approach aligns with the principles of patient-centred care, emphasising the reduction of risk and the enhancement of safety in clinical practices. The predictive derivative equation showcased in the work by Muniraman et al., which demonstrates a strong linear association and good agreement in both derivation and validation data sets, lends further credibility to the accuracy of OSI as a predictive tool for neonatal care.[1] The strong correlation observed, particularly in preterm infants and within the critical oxygen saturation range, underscores OSI’s potential in guiding therapeutic strategies based on non-invasive oxygenation indicators.
Our findings suggest that OSI could serve as a useful, non-invasive, continuous monitoring tool that may complement or, in some cases, replace traditional OI in neonatal care, particularly in settings where invasive procedures pose a higher risk. The significant correlation between OSI and OI, particularly in critical situations, points to the reliability of OSI as a monitoring tool. The development of a linear regression model for estimating OI from OSI measurements adds a valuable tool to the clinical arsenal, potentially reducing the need for invasive procedures. As neonatal care continues to evolve, the OSI stands out as a beacon of hope for enhancing patient monitoring, supporting clinical decision-making, and ultimately improving patient outcomes.
While this study has provided valuable insights into the utility of the OSI as a non-invasive alternative to the OI in neonates with respiratory diseases, several limitations must be acknowledged. The study’s sample size, while sufficient for preliminary findings, is relatively small and may limit the statistical power and generalizability of the results. Larger, multicentre studies are needed to validate these findings across more diverse neonatal populations. The diversity of respiratory conditions represented in the sample, while beneficial for assessing OSI’s applicability across a range of clinical scenarios, may also introduce variability that could affect the strength and interpretation of the correlation between OSI and OI. The study’s observational design, while appropriate for establishing correlations and exploring potential causative relationships, does not allow for the determination of causality. The findings indicate a significant correlation between OSI and OI, but further experimental and longitudinal studies are required to understand the directionality and causality of this relationship. Another limitation arises from the sole reliance on a single type of pulse oximeter (MASIMO RADICAL 7) for SpO2 measurements. While MASIMO pulse oximeters are widely regarded for their accuracy, different models or brands may yield slightly different results, potentially affecting the OSI’s calculated values and, by extension, the study’s findings. The calculation of the OSI and OI involves multiple variables, including MAP and FiO2, which are subject to fluctuations due to changes in ventilatory support settings or the neonate’s condition. These fluctuations might introduce additional variability into the OSI and OI calculations, potentially impacting their correlation and the study’s conclusions. The study’s timeframe and setting, confined to a single NICU at tertiary care centre, may also limit the generalizability of the findings to other settings and populations. Differences in clinical practices, patient demographics, and healthcare infrastructure across regions and institutions could influence the applicability of the study’s results elsewhere.
Given these limitations, future research should aim to address these gaps and further explore the utility of OSI in neonatal care. Larger, multicentre studies involving diverse neonatal populations and a variety of clinical settings would help validate the findings of this study and enhance their generalizability. Experimental studies designed to assess the impact of implementing OSI-based monitoring protocols on clinical outcomes, healthcare costs, and patient safety would provide valuable evidence to support the integration of OSI into routine neonatal care. Future studies could also explore the use of different brands and models of pulse oximeters to assess the consistency of OSI measurements across devices, which would help establish OSI as a reliable monitoring tool regardless of the specific equipment used in clinical settings. Investigating the applicability of OSI in other paediatric populations, such as children with ARDS or undergoing surgery, could broaden the scope of OSI’s utility in clinical practice. Furthermore, the development of advanced analytical models and algorithms that account for the dynamic nature of neonatal physiology and respiratory management could enhance the predictive accuracy of OSI for clinical outcomes. Finally, longitudinal studies tracking neonates monitored using OSI over time would offer insights into the long-term benefits and potential risks associated with this non-invasive monitoring approach, as well as explore the relationship between OSI measurements and developmental outcomes, providing a comprehensive understanding of OSI’s impact on neonatal care.
While our study provides important insights into the utility of the OSI over the OI in neonates with respiratory diseases, further research is necessary to strengthen these findings. We recommend increasing the sample size in future studies to improve statistical power and the generalizability of results. Additionally, future studies should segregate preterm and term neonates to allow for a more nuanced understanding of how gestational age may influence the relationship between OSI and OI. Conducting disease-specific analyses, such as focusing on neonates with MAS, RDS, and PPHN, will provide more precise insights into the utility of OSI in different respiratory conditions, facilitating tailored respiratory management strategies.
Conclusion
Our study demonstrates that the OSI is a viable, non-invasive alternative to the OI for monitoring neonates with respiratory diseases. The moderate correlation between OSI and OI, particularly within critical oxygen saturation ranges, supports its potential use in clinical settings. The regression model developed may further assist clinicians in estimating OI from OSI values. Future research is needed to confirm these findings in larger populations.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The ethical approval was obtained from the SDM, Medical College and Hospital (SDMIEC/2022/253 dated 27 July 2022).
Informed consent
Obtained from all the parents of the participants in the study.
Patient consent
Informed and written consent has been obtained.
Credit author statement
All authors contributed equally to the manuscript.
Data availability
Data is included in the manuscript.
Use of artificial intelligence
This article does not incorporate the use of artificial intelligence in any part of its development or analysis.