
Abstract
Background:
Dengue fever can present with symptoms that mimic drug-related reactions, especially in patients with complex medical histories, such as those with bipolar disorder on multiple medications.
Case details:
We report a 62-year-old female with a known history of bipolar disorder who was admitted with altered mental status, vomiting, and a rash. Given her psychiatric treatment, there was an initial concern for a drug-related reaction.
Investigations:
Through investigation was conducted. Results revealed a positive serology for dengue fever, alongside leukopenia and thrombocytopenia.
Discussion:
This case highlights the diagnostic challenge of differentiating between adverse drug reactions and infectious diseases like dengue in patients on multiple medications.
Conclusion:
Clinicians must maintain a high index of suspicion for tropical diseases like dengue, particularly in patients with complex comorbidities. This case underscores the importance of comprehensive evaluations in emergency settings and the need for a broad differential diagnosis approach.
Introduction
Dengue fever causes a high-grade fever with various associated symptoms including headache, myalgia, rash (sparing the palms and soles), retro-orbital pain and even swollen glands. Severe dengue might present with certain warning signs like severe stomach pain, persistent vomiting, bleeding, shortness of breath and restlessness. About 50%-82% of dengue-positive patients develop a cutaneous rash which typically starts three to four days after fever with positive predictive value of NS1 antigen testing during this period being 100%.[1] Skin rash starts with diffuse flushing followed by maculopapular rash coalescing together in the form of white islands in the Red Sea.[1] Drug reaction eosinophilia and systemic symptom (DRESS) syndrome is a potentially fatal drug-induced hypersensitivity reaction that not only includes skin manifestation but also has varied systemic manifestations.[2]
Case Presentation
A 62-year-old female, with a known case of bipolar disorder, was being treated with lithium, olanzapine and carbamazepine for 1 month. She presented to the medical emergency department with the chief complaints of altered mental status, dizziness, vomiting for 1 day and constipation for 2 days. There was no history suggestive of yellowish discolouration of eyes, abnormal body movements, loss of consciousness, intoxication, drug overdose, trauma or any source of infection. There was no travel history. Family history and past medical history for comorbidities were not significant. At admission, her oxygen saturation was 95% by pulse oximetry, heart rate of 115 beats per minute, blood pressure of 98/72 mm Hg. She was febrile to touch along with extensive blanchable rash present all over her body [Figures 1 and 2]. Her Glasgow Coma Scale score was E4V4M5. The neck was supple with no meningeal signs. There was no lymphadenopathy. The abdomen was soft, non-tender with no organomegaly. On auscultation of chest bilateral air entry was present with normal vesicular breath sounds heard all over the chest, anteriorly and posteriorly. Heart sounds were normal with no murmur or additional heart sounds. The rest of the systemic examination was unremarkable.
Figure showing extensive maculopapular blanchable rash on the bilateral lower limbs
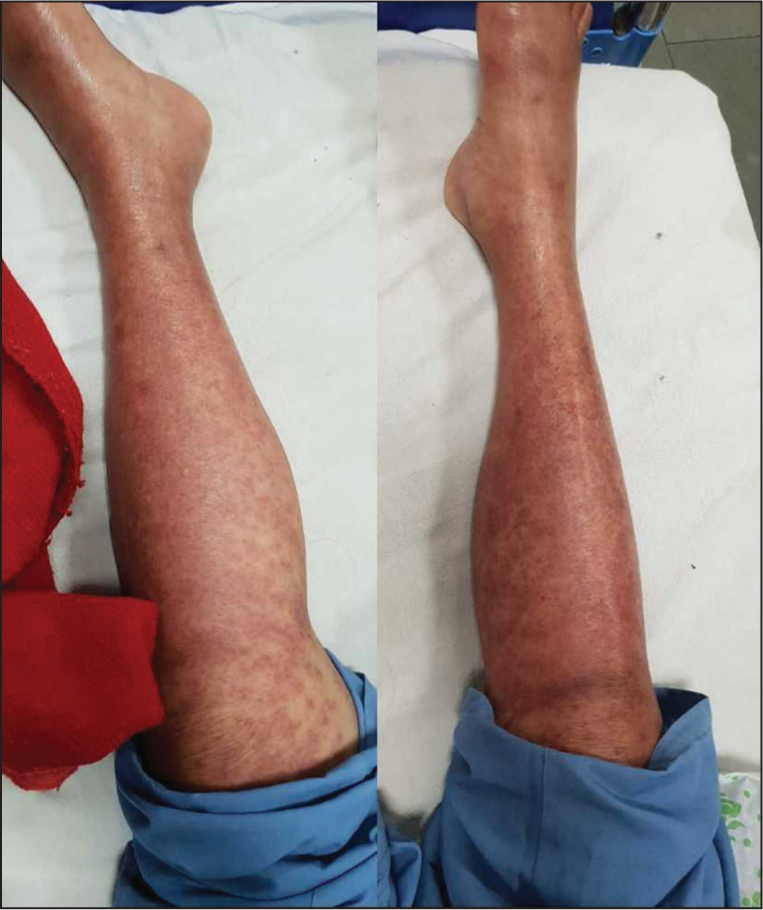
Figure showing the resolution of the rash

Further investigation like electrocardiogram was suggestive of Sinus tachycardia, chest roentgenogram was normal. Non-contrast computed tomography (NCCT) of head was also normal. Laboratory investigations are shown in Table 1. Blood and urine cultures came out to be sterile after specific incubation periods. Serum lithium levels were 0.66 mEq/L [range 0.6–1.2 mEq/L]. Eventually, during her hospital stay in view of thrombocytopenia, she tested positive for dengue IgM on day 6, while other tests including malaria, scrub typhus, leptospirosis all came out negative. The patient tested negative for hepatitis B, hepatitis C, and human immunodeficiency virus by ELISA method. The patient was initially being managed conservatively but had to be intubated in view of worsening GCS and deteriorating shock. The possibility of DRESS was kept in view of the history of consumption of carbamazepine and lithium with elevated eosinophil count, characteristic maculopapular rash and symptoms depicting multisystem involvement however, the diagnosis was later modified to dengue infection after she was being tested positive for IgM against dengue. She was being managed on the lines of acute febrile illness arising due to the dengue virus to which she gradually responded and got extubated. The platelet count started showing a rising trend and the eosinophil count dropped to 0%-1% following which she was discharged home with stable vitals and was followed up in the medicine outpatient department.
Complete laboratory investigations of the patient

Discussion
Due to heterogeneity of clinical presentation DRESS syndrome is often misdiagnosed. It has an incidence of about 1 per 1000 to 10000[2] with a characteristic triad of rash, systemic symptoms and eosinophilia.[3] The cutaneous and mucosal manifestations are the first clue to diagnosis which may start from maculopapular eruption which may progress to a coalescing erythema. The case fatality rate is 10%–20%.[4] The drug-specific immune response and herpes reactivation, especially HHV-6 triggers the expansion of a T cell population which cross-reacts with drug leading to cutaneous and visceral symptoms.[2] Steroid therapy along with stoppage of drug remains the mainstay of therapy.[2] There are seven J-SCAR criteria for diagnosis of DRESS syndrome. (a) Maculopapular rash developing 3 weeks after beginning treatment with causative drug; (b) prolonged clinical symptoms after discontinuing the causative drug; (c) fever >38 °C; (d) hepatic abnormalities; (e) leucocyte abnormalities; (f) lymphadenopathy; (g) HHV-6 reactivation. If all seven are present then typical drug-induced hypersensitivity syndrome, if only first five are present then atypical drug-induced hypersensitivity syndrome.[5] On the contrary, dengue being one of the most common tropical illnesses worldwide and is managed symptomatically with intravenous fluids, antipyretics and platelet transfusion when required.
Conclusion
The diagnostic dilemma not only arises due to the fact of quite similar dermatological eruptions but also systemic manifestations which include fever, lymphadenopathy, haematological abnormalities and various organ injuries which in the case of both diseases might manifest as transaminitis, acute kidney injury leading to proteinuria in DRESS while in dengue as pre-renal acute kidney injury during shock and altered mental status arising as a result of shock and metabolic derangements in dengue. Thus, the clinicians should keep a high index to suspicion to diagnose the two entities with similar presentation.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient consent
A written informed consent was duly signed by the patient. The consent was obtained after explaining to the patient that no identity will be revealed and the case information, including pictures will be used for education purpose only. The patient gave positive consent for publication and authors certify that written patient consent is present, procured for publication.
Credit author statement
AD: Case presentation, data collection, investigations and writing of original draft.
JK: Literature review, writing of original draft including conclusion, references.
YS: Intellectual content, literature search, manuscript final editing and review.
Data availability
None.
Use of artificial intelligence
None.