
Abstract
Introduction:
Sebaceous carcinomas are rare but potentially aggressive cutaneous malignancies. Surgical excision, albeit the primary modality of treatment, is associated with functional as well as cosmetic impairments. Radiotherapy offers an alternative treatment modality for those in whom surgical excision is not an option either due to medical reasons or patient preferences.
Materials and Methods:
Here we present a rare case report of an elderly Indian man with sebaceous carcinoma of the eyelid, for whom definitive radiotherapy was delivered as the primary modality of treatment.
Results:
There was a near complete response of the tumour to the definitive radiotherapy with acceptable toxicity.
Introduction
Sebaceous carcinoma (SC) is a rare but potentially aggressive cutaneous malignancy.[1] As the name suggests, any sebaceous gland in the skin can be the origin of this carcinoma. The head and neck region is the commonest region of its occurrence with the periocular region being the most common. Extraocular SCs are less frequent than the periocular variants which constitute up to 75% of all SCs. Generally, a disease of the elderly (median age of 72 years, affecting both sexes equally), SC is found to affect Caucasians more often, although the ocular variant is much more common in the Asian population. Periocular SC commonly arises from Meibomian glands and glands of Zeis, but can still arise from other parts of the eye like caruncle and pilosebaceous apparatus of hair follicles of the eyebrows. Ocular and extraocular SC have different behaviours and show different genetic signatures.[2] Since it can mimic benign conditions, a biopsy is inevitable for the diagnosis. Surgical excision remains the mainstay of treatment. Radiotherapy is primarily an adjuvant or palliative treatment option. In those who refused surgical intervention or in those where surgery is not feasible, radiotherapy can be employed as an alternate treatment tool. Here we report the case of a patient with SC of the eyelid with cervical lymph node metastasis in whom definitive radiotherapy was delivered successfully.
Case Report
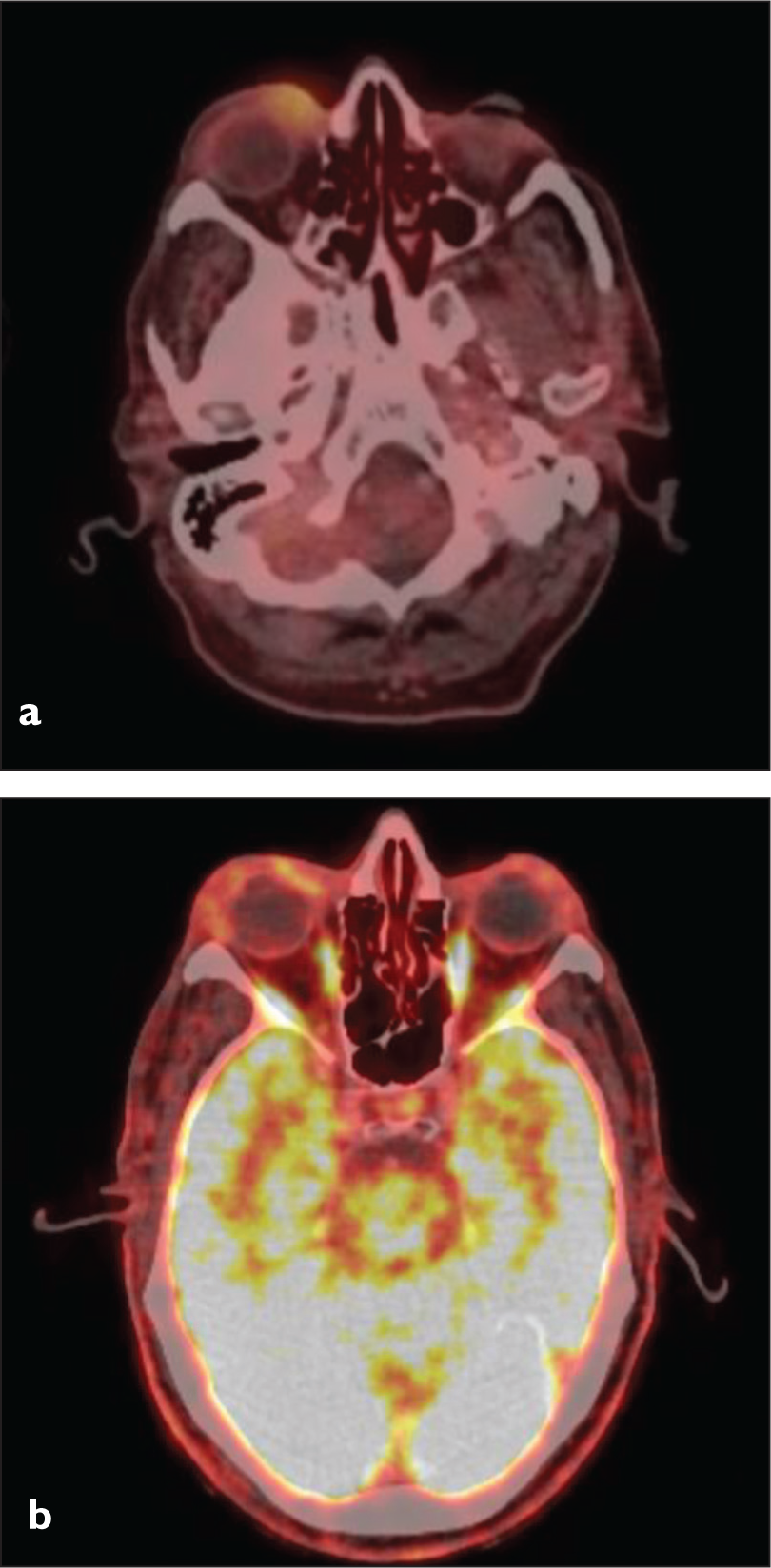
An 83-year-old hypertensive and diabetic gentleman, with a history of coronary artery disease and with European Cooperative Oncology Group- Performance Status 1, presented with a history of painless swelling in the right upper eyelid [Figure 1a]. On clinical examination, an enlarged submandibular lymph node and level V lymph node on the right side were noted. Biopsy from the right upper eyelid swelling was suggestive of poorly differentiated carcinoma, with a possibility of SC. He was then evaluated with an 18F-fluorodeoxyglucose positron emission tomography-computed tomography (FDG PET-CT) whole-body scan which showed a soft tissue lesion with necrotic areas in the right upper eyelid measuring 1.8 × 1.5 × 1.2 cm (SUVmax of 6.5), abutting the globe posteriorly with an indistinct fat plane but with no evidence of intraorbital extension, and prominent enlarged right intraparotid, level Ib and level V nodes [Figure 2a]. The patient was referred to the radiation oncology department. An opinion from the ophthalmologist and medical oncologist was sought before commencing the radiotherapy treatment. Ophthalmological examination revealed no remarkable abnormality in visual acuity or visual field.
Serial photographic appearance of the eyelid tumour over the course of radiotherapy (from left to right in order). (a) The initial appearance of the patient. Lump can be seen in the upper eyelid. (b) Appearance soon after the completion of radiotherapy. Significant regression in the lump can be appreciated. (c) Redness of the eyes and decreased thickness of eyebrows can be appreciated. Photographed during the immediate post-radiotherapy period. (d) Appearance at three months after radiotherapy. There is near complete regression of the eyelid tumour and improvement in the thickness of the eyebrows. However, there was a persistent redness of the eyes, which did not give the patient any distress

18 FDG PET-CT images. (a) Pre-radiotherapy and (b) post-radiotherapy
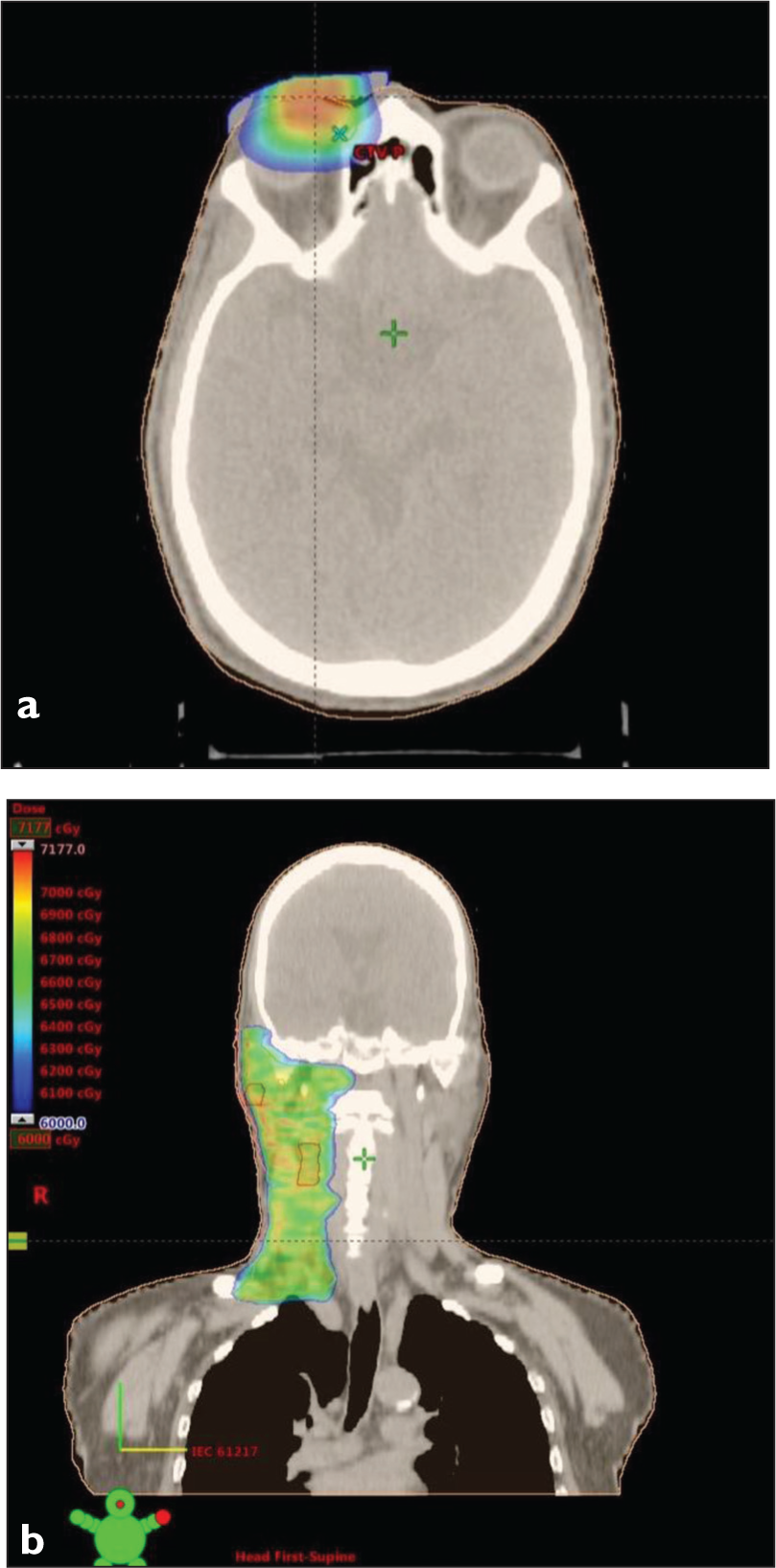
Patient was taken up for the radiotherapy treatment with a combined photon and electron approach. Patient was positioned in supine position with arms by the side. A planning CT scan of the head and neck was done without contrast. The target delineation was done after co-registration of PET-CT whole body and the planning CT scan. A cerrobend custom block was made for the electron treatment to the upper eyelid lesion. 6 MeV electrons were used to deliver a total dose of 60 Gy at 2.0 Gy per fraction to the right upper eyelid lesion. A customised lead shield was used for the protection of the globe. 6MV photons were used to deliver a total dose of 66 at 2.0 Gy per fraction to the clinical target volume (right neck nodes) using the volumetric modulated arc therapy technique [Figure 3a and 3b]. During the course of treatment, patient developed right eye discharge and tenderness in the right eyelid, which were treated conservatively under the guidance of the ophthalmologist. An interim follow-up CT scan of the neck was done after 23 fractions and it showed good response to the treatment. Rest of the treatment duration was uneventful, with patient tolerating the treatment satisfactorily. Apart from loss of thickness of eyebrows, redness, and discharge from eye, the treatment went on without the incidence of any high-grade dermatitis or other ocular toxicities. At the time of discharge, the eyelid lesion significantly reduced in size when compared to the initial presentation [Figure 1b and c].
Planning images (a) Axial view of the plan showing isodose colour wash covering the primary lesion. (b) Coronal view of the nodal irradiation plan
Patient was then followed up after three months. There were no additional side effects or worsening of redness of the eye. A physical examination revealed regression of the eyelid tumour and the nodes. There was an improvement in the thickness of the eyebrows. However, the redness of the eye was showing a slower resolution [Figure 1d]. The physical findings were backed up by the follow-up PET-CT whole-body scan which showed regression in size and metabolic activity of soft tissue lesion with necrotic areas in the right upper eyelid [Figure 2c]. There was a regression in size and metabolic activity of the involved nodes with near complete resolution of intra-parotid lymph nodes. The patient continues to carry out his day-to-day life activities without any burden of disease.
Discussion
Although surgical excision remains the primary treatment modality, in those who are deemed ineligible for surgical intervention, radiotherapy can be employed. Since surgery can cause functional and cosmetic impairment of the eyelid, radiotherapy offers a non-invasive and painless alternative.
In a study done by Hata et al., 13 patients with SC of the eyelid were treated with radiotherapy. Of the 13 patients, only one had cervical metastasis and none had distant metastasis. Five received radiation as a definitive therapy, whereas the remaining received it as an adjuvant therapy. Positive margins or close margins were the indication for adjuvant radiotherapy. Twelve patients received radiation using 5–11 MeV electrons and one patient received 6 MV X-rays. X-rays (4MV) were used to treat the ipsilateral neck in that single patient with cervical metastases. Gross disease (including metastatic cervical node) received a median dose of 66 Gy (range: 60–66.6 Gy) and those with positive or close margins received a median dose of 59.4 Gy (range: 50–61 Gy) to the tumour bed. The study reported a five-year local progression-free rate of 100% and disease-free rates of 89%. Five-year overall survival rate (OS) was 100%. In this study, none of the patients experienced any grade 3 or greater acute or late toxicities. Hence, the authors concluded that radiotherapy is a safe and effective treatment that can provide excellent tumour control and thus prolong survival.[3]
Yen et al. reported the findings of two cases of eyelid SC in which radiotherapy was employed. One case was a recurrence of the disease after an initial surgical intervention. Patient received a dose of 24 Gy in 12 fractions over 14 days using 100Kv X-ray, followed by 45 Gy in 25 fractions using 6MV X-ray beams. The total dose to the eyelid was 69 Gy. In the second case, patient received a dose of 59 Gy to the eyelid and a prophylactic dose of 50 Gy to the ipsilateral neck. The former patient remained disease-free till his death (39 months after radiation) and the latter patient also showed no evidence of disease recurrence 46 months after treatment. The authors concluded that radiotherapy is an effective curative treatment for eyelid SC using a dose >55 Gy.[4]
Takagawa et al. did a retrospective analysis of 83 patients with biopsy-proven SC of eyelid who were treated using radiation between 1983 and 2015. Seventy-eight per cent of the patients were treated with definitive radiotherapy, whereas the remaining patients received radiation as an adjuvant therapy due to recurrence of disease or positive surgical margins. All patients received a median dose of 60 Gy and the median follow-up period was 92.1 months. A seven-year local control rate of 60% was observed with doses in excess of 60 Gy in T1-T2 tumours. Interestingly, in this analysis, tumour size had an impact on the outcome of radiotherapy. Patients with a tumour size of <10 mm were found to have a better local control than those with tumour size of >10 mm. In addition to the local control, tumour size also correlated with neck nodal recurrence. The authors concluded that radiotherapy can be used as an effective alternative to surgery for tumours <10mm in size, while the latter is preferred in larger tumours of size >10 mm.[5]
Pardo et al. reported a local control rate of 90% at the primary site with follow-up ranging from 2 to 10 years, using a dose of 45–63 Gy. Overall five-year disease-specific actuarial survival was 96%. The authors concluded radiotherapy is an effective treatment for SC of ocular adnexa.[6]
The role of prophylactic nodal irradiation needs further study. Nevertheless, a total dose of 45–50 Gy seems to be appropriate for prophylactic neck nodal irradiation, especially for tumours of size >10 mm or T4 disease.[5]
Side effects of radiation include conjunctivitis, keratitis, dry eyes, loss of eyelashes, thinning of eyebrows, cataracts, and very rarely vision loss. Serious adverse effects (Grade 3 or more) are not usually encountered. With the advancement in the techniques of radiotherapy and with the availability of daily imaging and adaptive treatment, the side effects can be further minimised.
In our case, using a dose of 60 Gy (and 66 Gy to the nodes), a good reduction in the size and metabolic activity of the tumour was achieved within a short period with no severe adverse effects. Long-term follow-up is desirable to understand the additional benefits of radiation. Hence, our experience also adds to the value of radiotherapy as a comparable alternative to surgical excision of SC.
Conclusion
Radiotherapy is an effective treatment strategy for SC in those where surgery is not an option, particularly when there is involvement of nerve or lymph nodes. It offers excellent local control with good functional and cosmetic outcomes. Accurate delineation of the involved regions can help in sparing the normal tissue, while the availability of daily imaging can be exploited for minimal setup errors. In short, radiotherapy is an excellent tool that is non-invasive, painless and with no drastic adverse effects to tackle the clinical entity called SC.
Footnotes
Acknowledgements
The authors convey their deep-felt gratitude to all those who helped in the process of drafting the manuscript. We thank our colleagues, medical physicists, radiation technologists and sisters for all their work, dedication and cooperation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Informed consent
Informed consent for radiotherapy was obtained before the treatment.
Patient consent
The authors certify that they have obtained informed consent from the patient. The patient has given his consent for the usage of images, and other clinical information for publication in the journal. The patient understands that his name or initials will not be published, and while all attempts will be made to conceal his identity, complete anonymity cannot be guaranteed.
Credit author statement
Kesav Ajith was involved in data collection and compilation of the article.
R. Rathnadevi and B. Subathira contributed to guidance in compilation and final review of the article. This manuscript has been read and approved by all the authors. All the authors believe that the manuscript represents an honest work that contributes to the knowledge pool in the field of radiotherapy.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article.
Use of artificial intelligence
None.