
Abstract
Background and Aims:
Spinal anaesthesia (SA) stands as a widely utilised anaesthetic approach for patients undergoing surgeries involving the lower limb, lower abdomen, pelvis and perineum. This study aims to evaluate the safety of fractionated dose versus bolus dose injection of hyperbaric bupivacaine (0.5%) with buprenorphine in SA for lower limb surgeries concerning haemodynamic stability, total analgesia duration and the quality of sensory and motor blocks.
Results:
In our investigation, we observed that five minutes after administering SA, the sensory level was notably elevated in the fractionated group, with a majority of patients (62.9%) reaching a level of T10. Simultaneously, the corresponding motor block, assessed using the modified Bromage score, predominantly showed a score of 4 in the fractionated group, with 77.10% of patients exhibiting this level, compared to 62.90% in the bolus group. By the 20-minute mark post-SA, the majority of patients in the fractionated group had sensory levels at either T8 or T10, while in the bolus group, an equal number of patients (40%) had reached these levels, and around 5.7% even displayed a level at approximately T6.
Conclusion:
In conclusion, when comparing the patients in Group F [fractionated dose of bupivacaine and buprenorphine] to those in Group B [bolus dose of bupivacaine and buprenorphine], the patients in Group F exhibited a higher level of haemodynamic stability.
Introduction
Spinal anaesthesia (SA) stands as a widely utilised anaesthetic approach for patients undergoing surgeries involving the lower limb, lower abdomen, pelvis and perineum.[1] It is often favoured over general anaesthesia due to its attributes such as dense block provision, rapid action, minimal impact on mental status, reduced blood loss and protective effects against thromboembolic complications.[1] The sympathetic blockade induced by SA, via sympathetic denervation, results in prolonged and occasionally severe hypotension, primarily due to the swift extension of the sympathetic block impeding the cardiovascular system’s adaptation, thereby leading to significant morbidity and mortality risks.[1,2] A fractionated dose of spinal anaesthetic presents an alternative administration method, wherein two-thirds of the total calculated dose is initially administered, followed by the remaining one-third after a 90-second interval, ensuring adequate motor and sensory blockade.[3–5]
This approach offers a dense block with heightened haemodynamic stability. The dosage of hyperbaric bupivacaine is contingent upon factors like weight, height and spinal anatomy, determining the intensity and duration of the spinal block.[6] For surgeries lasting between 2 and 2.5 hours, intrathecal 0.5% bupivacaine with dextrose is deemed optimal.[6]
The inclusion of additives with local anaesthetics in SA serves to prolong the anaesthetic action, thereby extending surgical durations.[7] Notably, buprenorphine, a partial opioid receptor antagonist, when combined with bupivacaine, extends analgesic duration without significant alterations in blood pressure or pulse rate and without inducing physical or psychological dependence. Intrathecal administration of buprenorphine in smaller doses offers profound and prolonged analgesia due to its highly lipophilic nature, with fewer adverse effects such as nausea, vomiting and constipation compared to other opioids.[8,9] In light of existing literature, a prospective study is planned to compare the efficacy of bolus dose versus fractionated dose administration of hyperbaric bupivacaine in SA among adult patients undergoing lower limb surgeries.[5] This study aims to assess sensory and motor block characteristics alongside haemodynamic parameters, including onset, peak, regression of sensory block, motor blockade, vasopressor and atropine requirements and visual analogue scale (VAS) scores.
Previous studies comparing fractionated versus bolus dose administration of SA predominantly employed local anaesthesia without adjuvants.[5-8] Hence, this study seeks to ascertain the safety of fractionated versus bolus dose administration of SA with buprenorphine as an adjuvant in lower limb surgeries. The comparison will extend to haemodynamic stability, total analgesia duration and the quality of sensory and motor blocks.
Ultimately, this study aims to evaluate the safety of fractionated dose versus bolus dose injection of hyperbaric bupivacaine (0.5%) with buprenorphine in SA for lower limb surgeries concerning haemodynamic stability, total analgesia duration and the quality of sensory and motor blocks.
Materials and Methods
A randomised controlled trial was conducted from January 2023 to January 2024 after obtaining approval from the Institutional Ethics Committee, adhering to ethical standards throughout the research process. A sample size of 54 per group was determined accounting for potential dropouts, considering a dropout rate of 10%.[7] The criteria for participant selection were carefully established. Inclusion criteria encompassed patients who had undergone lower limb surgeries and had American Society of Anesthesiologists (ASA) physical status 1 and 2, were aged between 18 and 60 years, had a body mass index (BMI) falling within the range of 18.5 to 24.9 kg/m2 and had a height ranging from 150 to 180 cm. Conversely, exclusion criteria included patients with ASA physical status 3 and 4, pre-existing cardiovascular or cerebrovascular disease, allergies or hypersensitivity to local anaesthetic drugs, spinal deformities, history of laminectomy, contraindications to regional anaesthesia, inadequate sensory blockade necessitating conversion to general anaesthesia, increased intracranial pressure, altered mental status, BMI falling below 18.5 kg/m2 or exceeding 22.9 kg/m2 and patients unwilling to provide consent. No biological materials were required for the study, streamlining the logistical aspects and focusing primarily on procedural and statistical methodologies.
Before the surgery, patients were informed and consent was obtained. They were then randomly divided into two groups using a computer-generated method, ensuring a double-blinded process. Group B received a bolus dose comprising 2.8 mL of bupivacaine and 0.2 mL of buprenorphine (60 μg), whereas Group F received a fractionated dose. The fractionated dose involved administering 1.9 mL of bupivacaine + 0.1 mL of buprenorphine initially, followed by the remaining 0.9 mL of bupivacaine + 0.1 mL of buprenorphine after 90 seconds.
On the day of the surgery, patients were transferred to the operating room after providing consent and were assigned one of the two interventions. Standard monitors were attached to measure baseline systolic, diastolic, mean arterial pressures (MAPs), heart rate and oxygen saturation. SA was administered to patients in the sitting position using a 25G Quincke-Babcock spinal needle after infiltrating the skin with lignocaine (2 mL, 2%).
Following the observation of free flow and aspiration of cerebrospinal fluid, hyperbaric bupivacaine 0.5% heavy with adjuvants was injected based on the respective group (Group B or Group F). Group B patients received a single bolus dose, while Group F patients received a fractionated dose.
Fractionated SA involves administering the local anaesthetic in multiple small doses rather than a single large bolus, aiming for a controlled and gradual onset of anaesthesia. This technique begins with an initial spinal puncture and the injection of the first fraction of the anaesthetic dose, followed by careful assessment and incremental administration of additional doses. By allowing time between each injection to observe the effects, this method enhances control over the extent and height of the sensory and motor block, reducing the risk of high spinal block and improving haemodynamic stability. This approach can lower the incidence of adverse effects associated with large bolus doses, offering significant advantages in patient safety and outcomes.[4,5]
Patients were then placed in the supine position, and the onset, level and regression of sensory and motor blocks were assessed. Sensory block assessment was confirmed by the loss of sensation to pinprick, while the modified Bromage scale was used to assess motor block.
Haemodynamic parameters were recorded immediately after administering SA and subsequently at regular intervals throughout the surgery. Post-operatively, pain assessment was conducted using the VAS, and intravenous tramadol 50mg was administered as rescue analgesia if the VAS score exceeded 4. Additionally, the time taken for the first demand of rescue analgesia was noted for patients who did not require initial rescue analgesia. The outcome measures are the assessment of motor block by the Modified Bromage Scale and the assessment of postoperative pain by VAS Score.
Statistical analyses employed rigorous methods, including the independent t-test or Mann–Whitney test for quantitative variables and the chi-squared test or Fisher’s exact test for qualitative variables, with a significance threshold set at p < 0.05. Furthermore, quantitative data underwent analysis using unpaired t-tests, with statistical significance defined as p < 0.05, ensuring a comprehensive and reliable interpretation of the study outcomes. Through meticulous planning and methodological rigor, the study aimed to contribute valuable insights into the efficacy of different anaesthesia administration approaches in lower limb surgeries.
Results
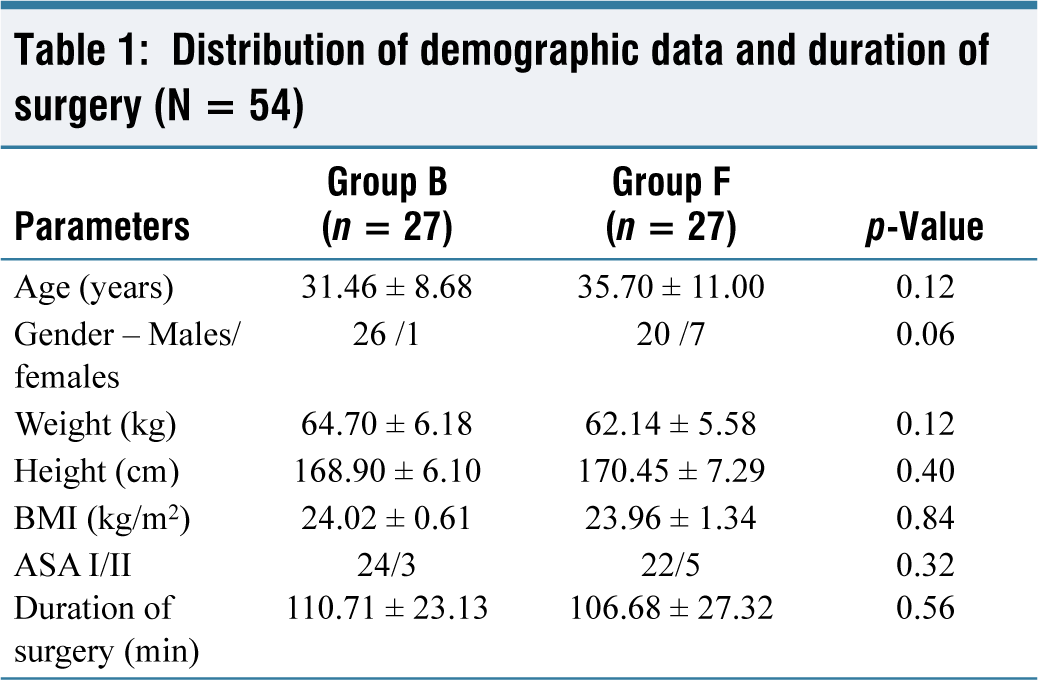
Demographically, the age, gender, height and weight of patients in both groups showed no significant differences. The majority of patients included in the study underwent orthopaedic procedures, and the average duration of surgery was similar across the groups as well (Table 1).
Distribution of demographic data and duration of surgery (N = 54)
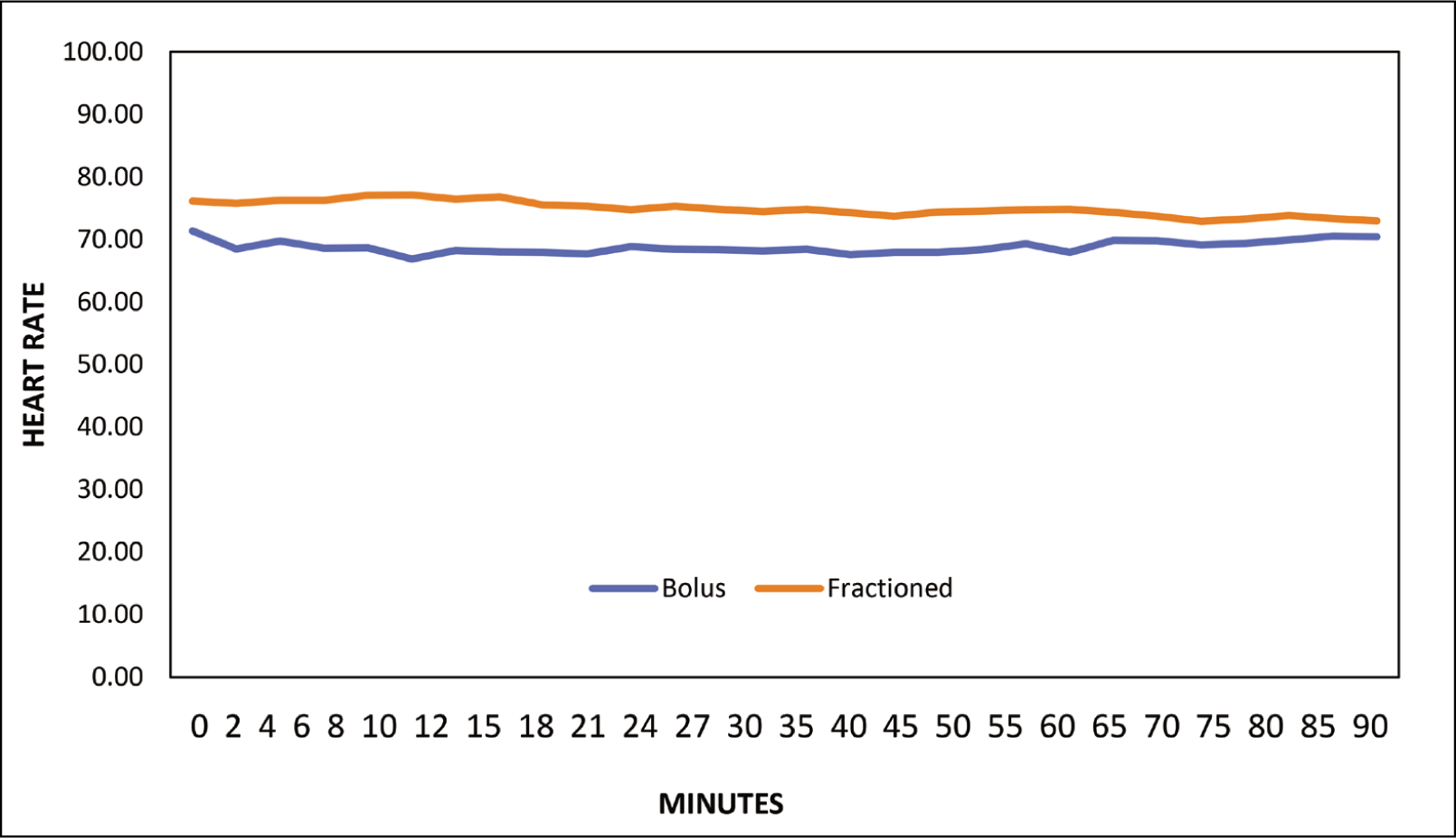
The heart rate data between the bolus and fractionated groups was analysed at various time points throughout the study. At baseline, there was no significant difference in mean heart rates between the two groups (71.37 in the bolus group and 76.11 in the fractionated group, p = 0.10). However, from 0 minutes onwards, the heart rates in the fractionated group tended to be consistently higher compared to the bolus group, with statistical significance observed at multiple time points (p < 0.05). This trend continued until around the 85-minute mark, after which the difference in heart rates between the two groups became nonsignificant (p > 0.05). Overall, the data suggest that patients in the fractionated group exhibited slightly elevated heart rates compared to those in the bolus group during the intraoperative period (Figure 1).
Distribution of heart rate among the study participants (N = 54)
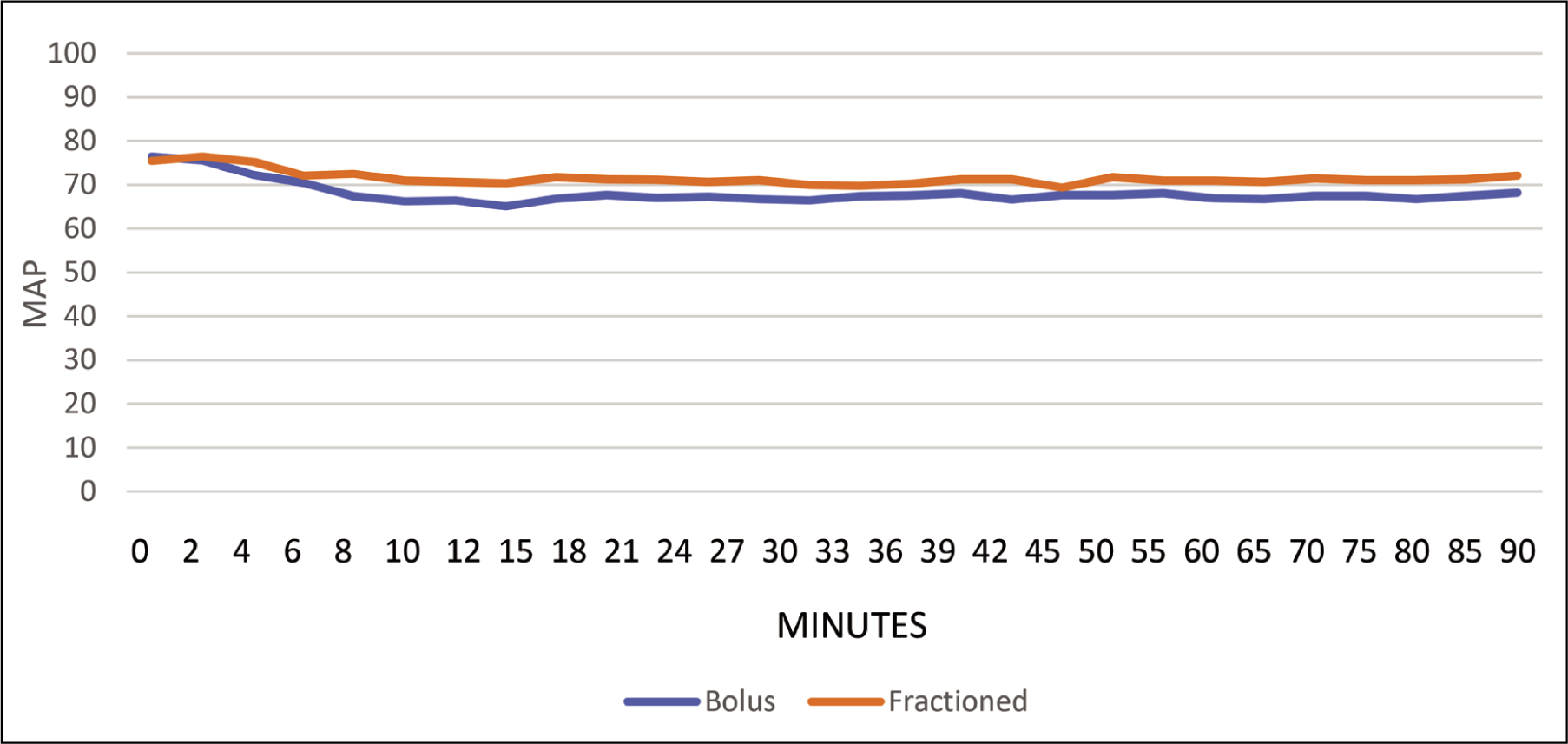
The MAP data between the bolus and fractionated groups were compared at various time points throughout the study. Initially, at baseline, there was no significant difference observed in the MAP between the two groups (93.71 in the bolus group and 96.54 in the fractionated group, p = 0.26). However, as the study progressed, differences in MAP between the two groups became apparent. From six minutes onwards, the MAP in the fractionated group was consistently higher compared to the bolus group, with statistical significance observed at multiple time points (p < 0.05). This trend continued until the end of the study, with the fractionated group maintaining higher MAP values compared to the bolus group. Notably, at eight minutes, the difference in MAP between the two groups became statistically significant (p = 0.01), and this significance persisted throughout the remainder of the study. Overall, the data suggest that patients in the fractionated group tended to exhibit higher MAPs compared to those in the bolus group during the intraoperative period (Figure 2).
Distribution of mean arterial pressure in the study (N = 54)
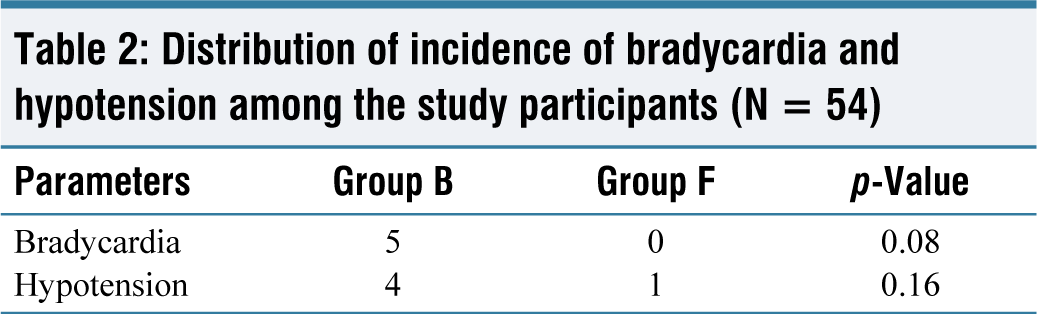
For bradycardia, five occurrences were noted in Group B, while none were reported in Group F. Although there appears to be a trend towards a higher incidence in Group B, the p-value of 0.08 suggests that this difference did not reach statistical significance. Regarding hypotension, Group B reported four cases compared to one case in Group F. However, similar to bradycardia, the p-value of 0.16 indicates that this difference was not statistically significant (Table 2).
Distribution of incidence of bradycardia and hypotension among the study participants (N = 54)
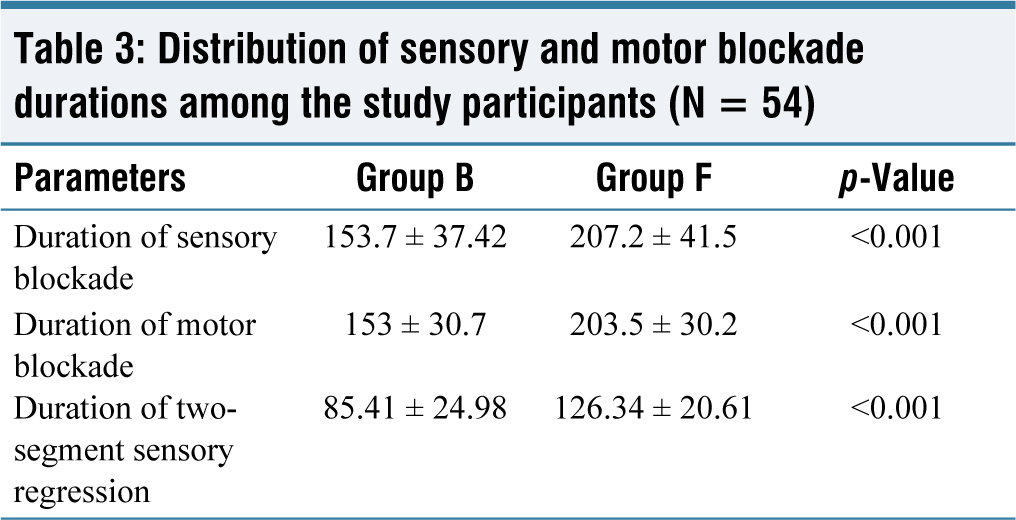
The comparison between Group B and Group F revealed significant differences in the duration of sensory blockade, with Group F exhibiting a longer duration (207.2 ± 41.5) compared to Group B (153.7 ± 37.42) (p < 0.001). Similarly, the duration of motor blockade was significantly longer in Group F (203.5 ± 30.2) compared to Group B (153 ± 30.7) (p < 0.001). Furthermore, the duration of two-segment sensory regression was notably longer in Group F (126.34 ± 20.61) compared to Group B (85.41 ± 24.98) (p < 0.001). These findings suggest that Group F experienced prolonged sensory and motor blockade durations, as well as a slower regression of sensory effects compared to Group B (Table 3).
Distribution of sensory and motor blockade durations among the study participants (N = 54)
Discussion
Patients having lower limb surgical operations can benefit from SA since it is one of the most recommended ways of central neuraxial blockade. SA gives patients anaesthesia that is intense, profound and effective. Due to the quick blocking of the sympathetic nerves, the use of SA does, however, carry with it the danger of hypotension that is both severe and prolonged. Additionally, this risk is associated with the use of SA.[4,10] According to several studies, reducing hypotension and bradycardia while simultaneously increasing the duration of analgesia can be accomplished by dividing the complete dose of SA into portions and then providing the dose at several short time intervals. Among senior patients undergoing hip operations, Favarel-Garrigues et al.[11] conducted a study to compare the haemodynamic effects of bolus and titrated doses of SA. They discovered that titrated doses offered a longer duration of action and greater circulatory stability. According to the findings of Badheka et al.[3] in their research, ‘fractionated dose of spinal anesthesia provides better hemodynamic stability and longer duration of analgesia compared to the bolus group’.
Although spinal block is dependent on a variety of parameters, including the drug, the method and the features of the patient, the most essential factors are the baricity, the dose and the position of the patient. The vast majority of the studies that have been undertaken on fractionation have been carried out on pregnant women who are undergoing lower segment caesarean section (LSCS). These women required a lower dose of the local anaesthetic in comparison to patients who were undergoing orthopaedic surgery for a longer period. Our research involved administering a set dose of 3 mL of hyperbaric bupivacaine at a concentration of 0.5% while the patient was seated. The two groups were compared concerning their mean height, weight, age, gender and the length of time they had undergone surgery. To investigate the effects of fractionation, Srivastava et al.[12] conducted a trial in which they administered 3 mL (15 mg) of 0.5% hyperbaric bupivacaine to patients who were undergoing lower limb procedures. Nearly all of the investigations that have been conducted on fractionated doses have demonstrated that the haemodynamic circumstances following SA are improved. When it came to bradycardia, our study of the data revealed that there were five instances reported in Group B, whereas there were none reported in Group F. Although it seems that there is a tendency towards a greater incidence in Group B, the p-value of 0.08 indicates that this difference did not reach the level of statistical significance that may be considered significant. The number of cases of hypotension that were reported by Group B was four, while Group F only reported one incidence. On the other hand, the p-value of 0.16 indicates that this difference was not statistically significant, which is identical to the situation with bradycardia.
It should be noted that the majority of the trials conducted on hyperbaric bupivacaine 0.5% did not include any additives, which may have contributed to the longer duration of sensory and motor block. When compared to a single bolus dosage, the fractionated dose group exhibited a longer duration of analgesic effects, as well as a late recovery of sensory and motor block when compared to the single bolus dose group.[13] As part of our research, we suggested the use of buprenorphine as a means of extending the duration of analgesia while simultaneously reducing the adverse effects associated with opioids. The sensory evaluation that was performed at five minutes in our research revealed that a greater proportion of patients had a block height of ten minutes, and at twenty minutes, the highest height of the block that was reached in the fractionated group was eight minutes. While the height of the block was equivalent at different levels over five minutes in the bolus group, the maximum level that was obtained was T6 after twenty minutes. This could be related to the increased bouts of hypotension and bradycardia that occurred in the bolus group, even though only a small percentage of the patients in the bolus group achieved a higher level of block.
During our research, we found that there were notable variations in the duration of sensory blocking between Group B and Group F. Specifically, Group F had a longer duration of 207.2 ± 41.5, in comparison to Group B, which exhibited a shorter period of 153.7 ± 37.42 (p < 0.001). In a similar vein, it was shown that the duration of motor blockade was substantially longer in Group F (203.5 ± 30.2) as compared to Group B (153 ± 30.7) (p < 0.001). Furthermore, it is worth noting that the duration of two-segment sensory regression was significantly longer in Group F (126.34 ± 20.61) as compared to Group B (85.41 ± 24.98) (p < 0.001). Based on these findings, it appears that Group F experienced longer periods of sensory and motor blockage, as well as a slower recovery of sensory effects in comparison to Group B. One of the drawbacks of our study is that patients with ASA 1 or ASA 2 physical conditions were given a fixed dose of the medication without having the amount calculated according to their weight or height. This is one of the reasons why our study has limitations.
Conclusions
In conclusion, when comparing the patients in Group F to those in Group B, the patients in Group F exhibited a higher level of haemodynamic stability. This was the case when hypotension and bradycardia episodes were taken into consideration. It was found that Group F experienced a sensory and motor obstruction that persisted for a much longer duration of time in comparison to Group B. In contrast to Group B, the duration of analgesia that was experienced by individuals in Group F was significantly longer than that of Group B. The use of bupivacaine in conjunction with an opioid such as buprenorphine results in analgesia that lasts for a longer period and reduces the requirement for additional pain medication as a rescue measure.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional ethical committee approval number
SJH/IEC/2022/076 dated 10-11-2022.
Informed consent
Obtained from all the participants in the study.
Credit author statement
Conceptualisation - RP Chandrasekaran Manuscript writing - TT Arulpari Manuscript revision - M Ganapathysubramanian Data analysis - TT Arulpari, M Ganapathysubramanian, RP Chandrasekaran Supervision - RP Chandrasekaran
Data availability
Data is included in the manuscript.
Use of artificial intelligence
Not applicable.