
Abstract
Background and Aims:
Rhabdomyosarcoma (RMS) is the most common subtype of soft tissue sarcoma (STS) in children. Early diagnosis is the most favourable prognostic factor and thus physicians need to include RMS in the differential diagnosis of more common diseases developing within the head and neck region. This report highlights the same while describing a case of an eight-year-old child who presented with a chin swelling which turned out to be an RMS.
Methods:
We present a rare case of an eight-year-old child with a midline painless mass.
Results:
This child had a transoral resection of the mass. He undertook further chemotherapy and was completely cured with no tumour recurrence.
Conclusion:
In a painless rapidly increasing mass in the head and neck area, despite rare, but RMS should be included as a differential diagnosis. This is important as early diagnosis and proper resection and treatment are paramount in the prognosis of the disease.
Introduction
Rhabdomyosarcoma (RMS) is the most common subtype of soft tissue sarcoma (STS) in children, accounting for around 4.5% of all paediatric malignancies.[1] The head and neck (H&N) region are the most common anatomical location of paediatric RMS, being the primary tumour site in approximately 35% of cases.[2] They are divided into embryonal, alveolar, pleomorphic and spindle type based on histological morphology. The H&N RMS are divided into orbital, parameningeal and non-parameningeal based on the site of involvement.[2,3] The aggressiveness for invasion based on histology and amenability for complete resection and early presentation based on the site of involvement play crucial roles in prognosis. Non-parameningeal RMS comprise tumours developing within the oral cavity, nasal cavity, larynx, ear, cheeks and salivary glands, as well as the skin, subcutaneous tissue and muscles of the H&N.[2,3] They typically present as a firm, non-painful, non-movable mass, disfiguring the area of H&N. They are usually of embryonal histology and are more amenable to complete resection compared to parameningeal RMS; therefore, they carry more favourable prognosis.[1-3] Early diagnosis in a low, resectable stage is still the most favourable prognostic factor and thus physicians need to include RMS in the differential diagnosis of more common diseases developing within the H&N.[1-3] This report highlights the same while describing a case of an eight-year-old child who presented with chin swelling which turned out to be an RMS.
Case Report
An eight-year-old child presented with a discrete swelling on the chin 1.5 cm × 3.0 cm in size. The swelling was present for six months and was recently noticed when the skin over it became reddish in colour. On examination, it was a non-tender firm swelling which had well-defined margins and was freely mobile. However, the skin over the swelling was red and was not pinchable. There were no palpable cervical lymph nodes. The child had no speech or chewing difficulty.
An ultrasound of the swelling revealed a well-defined heterogenous swelling of 1.5 × 2.8 cm seen in the subcutaneous plane. On colour Doppler, it showed slightly increased vascularity, with findings more in favour of an infective aetiology. To rule out dental swellings and swellings arising from mandible, an X-ray skull was advised which was essentially normal [Figure 1].
Clinical, X-ray and ultrasound images

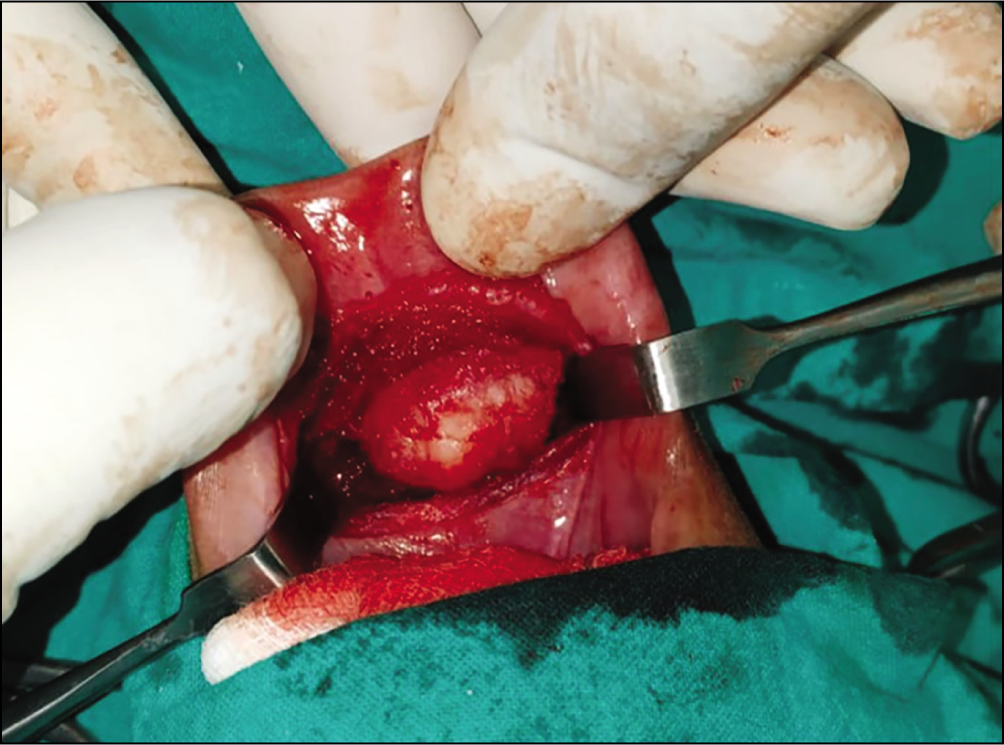
Due to its mobility and absence of any associated cervical lymph nodes, we suspected the lesion to be of benign origin and planned an intraoral excision for cosmetic concerns. Intraoperatively an incision was given 3 cm away from the gums on the inner mucosal side of the lower lip. It was deepened after incising the orbicularis oris muscle and mentalis muscle. The swelling was easily dissected laterally and inferiorly [Figure 2]. However, the swelling was densely adherent to the subcutaneous tissue and could be dissected from it with great difficulty. The skin over the swelling was very thin but careful dissection prevented any injury to it. The child was uneventfully discharged the next day.
Intraoperative image of swelling during intraoral excision
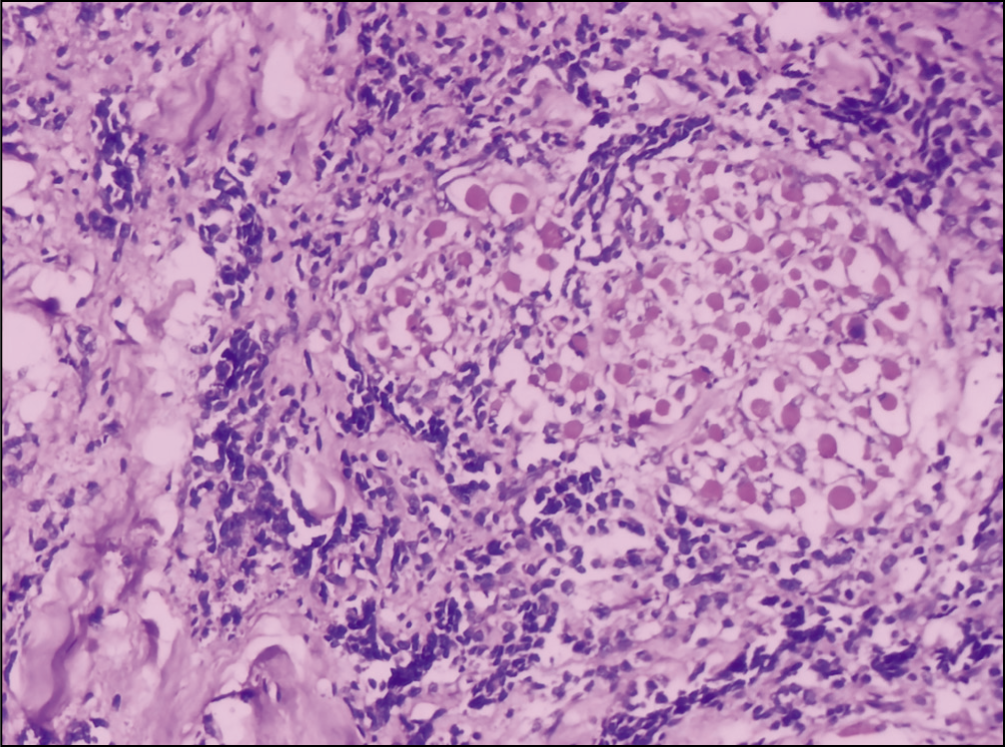
A biopsy of the swelling revealed it to be a small round blue cell tumour [Figure 3]. To further characterise the tumour, an immunohistochemistry was done. This revealed the tumour to be positive for desmin, MYOD1 and myogenin, while it was negative for NKX 2.2, CD 45 and Ki67. Based on the above, it was diagnosed as an RMS with mixed embryonal and alveolar histology.
Eosin and haematoxylin stained photomicroscopy showing round blue cells around skeletal muscle bundles
The child was referred to a paediatric oncologist who ordered a PET-CT scan (positron emission tomography with contrast-enhanced computerised tomography scan). It showed no abnormal FDG (fluorodeoxyglucose) uptake at the operative site or in the cervical region.
A three-drug VAC (vincristine, dactinomycin, cyclophosphamide) was started on the patient. After two cycles, the patient had a repeat PET-CT scan which was normal. The patient continues to be under close follow-up and has not had any tumour recurrence for the last six months after completion of the chemotherapeutic regimen.
Discussion
Non-parameningeal RMS are having a better prognosis because of early diagnosis because of early manifestation usually in the form of discrete palpable/visible painless masses and cranial nerve palsies.[1-4] They are amenable to complete resection too as are detected early and are more superficially located as compared to meningeal RMS.[4] In our case too, an early detection and complete resection made the prognosis better.
However, in our case, it was more a palpable mass rather than a visible mass. Parents noticed the swelling only after evident skin colour changes. It was suspected to be an infected dermoid because of its unrestricted mobility and non-fixity to surrounding structures. For cosmetic concerns, as the swelling was suspected to be clinically and radiologically benign, we resected it by a transoral route.
The differential diagnosis for midline chin masses includes post-traumatic haematoma, benign tumours, congenital malformations and infectious processes.[4,5] Close differentials are dermoid cyst, glioma, superficialis lipomatosus, skin tags, foetal rhabdomyoma, fibrous hamartoma of infancy and neuromuscular hamartoma (benign Triton tumour), embryonal RMS. Foetal rhabdomyoma, neuromuscular hamartoma, embryonal RMS and rhabdomyomatous mesenchymal hamartoma all contain skeletal elements in the dermis and/or subcutaneous tissue.[5] In rhabdomyomatous mesenchymal hamartoma, the striated muscle is well differentiated and randomly arranged, while in foetal rhabdomyoma, there are less differentiated and denser muscular elements. In neuromuscular hamartoma, the muscle fibres are intimately associated with nerve fibres. Embryonal RMS has a malignant histologic characteristic exhibiting an abnormal arrangement of dermal mesenchymal elements and prominence of skeletal muscle which makes it unique.[5]
In paediatric RMS, most relapses occur in the first two years post-therapy.[6] Thus, following completion of treatment, it is recommended to perform an ultrasound examination of the primary tumour, in case of superficial lesions like ours. In case of a suspicious nodule on radiography, CT is advised for characterisation. After two years, imaging is recommended only if new clinical symptoms develop because routine screening has limited added detection value.[6]
In a painless rapidly increasing mass in the head and neck area RMS should be included as a differential diagnosis. This is important as early diagnosis and proper resection and treatment are paramount in the prognosis of the disease. In doubtful cases, diagnostic biopsy of the tumour should be carefully planned by a paediatric surgeon experienced in childhood cancers. As it is common for these tumours with trivial symptoms to reach other specialities, it is imperative to educate paediatricians, family doctors, fellow paediatric surgeons, maxillofacial surgeons, laryngologists, to avoid delays and errors in management.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
None.
Informed consent
Taken from patients’ attendants.
Credit author statement
Saurabh Garge: Conceptualisation of paper.
Ashutosh Sharma: Review of literature.
Rajesh Kumar: Helped with the pathology literature.
Manish Kumar: Helped with proof reading and corrections.
Data availability
Available.
Use of artificial intelligence
None.