
Abstract
Background and Aims:
This study aims to investigate the clinicopathological profile of cervical lymphadenopathy in a tertiary referral centre. The findings will contribute to a deeper understanding of the disease spectrum, aid in accurate diagnosis, and help in improving patient treatment and outcomes.
Methodology:
This is a prospective study conducted in the Department of ENT, Head and Neck Surgery, Apollo Hospital, Chennai, between June 2022 and May 2023. The clinicopathological profile of all patients was analysed. The final histological diagnosis and the preoperative Fine Needle Aspiration Cytology (FNAC) were correlated. The primary tumour was identified in cases with metastatic secondary tumours in the neck.
Results:
Among the 80 patients in our study, 67% had a benign aetiology (most common was tuberculosis), and 33% had a malignant aetiology (most common was Hodgkin’s Lymphoma). Gender distribution was equal, with those between the ages of 35 and 60 more frequently affected. The nasopharynx (30%) was the most likely location of the occult primary, followed by the thyroid (20%) and larynx (20%). In detecting TB, FNAC had a sensitivity of 75.5% and a specificity of 98%; in detecting lymphomas, it was 64% and 100%; in detecting metastatic secondaries, it was 80% and 100%; and in detecting reactive lymphadenitis, it was 79% and 86%.
Conclusion:
Cervical lymphadenopathy is a common entity requiring careful evaluation and treatment. PET scans prove invaluable in detecting occult primary tumours. FNAC is an initial, cost-effective diagnostic tool. However, biopsy is indicated in specific conditions to obtain accurate diagnosis to enable prompt treatment.
Introduction
Cervical lymphadenopathy is a prevalent clinical condition that is seen by medical practitioners worldwide. About 1/3rd of our body’s lymph nodes are situated in the neck region.[1] The presence of cervical lymphadenopathy can indicate various underlying pathologies, ranging from benign reactive processes to malignant neoplasms. In 3%–5% of head and neck cancer cases, cervical lymphadenopathy accounts for metastasis with an unknown origin. It can also be an indication of extrapulmonary tuberculosis.[2,3] In India, the high population density, diverse socio-cultural factors, and endemic infectious diseases contribute to the complexity of diagnosing and managing cervical lymphadenopathy. The clinical evaluation alone often fails to provide a definitive diagnosis, necessitating the integration of various diagnostic modalities and techniques. With its minimal invasiveness and cost-effectiveness, Fine Needle Aspiration Cytology (FNAC) has become a valuable frontline study that allows for fast and precise diagnosis.[4] Even with its benefits, FNAC’s effectiveness depends on the sample’s representativeness and the calibre of the preparation, which makes it difficult to get results that are consistently reliable. In this context, the present study aims to investigate the clinicopathological characteristics of cervical lymphadenopathy in a tertiary referral centre. The findings of this study will contribute to a deeper understanding of the disease spectrum, aid in accurate diagnosis, and provide insights for improving patient care and outcomes.
Materials and Methods
This prospective study was conducted at the Department of ENT, Head and Neck Surgery in a Tertiary care Hospital in Chennai, India, for 1 year between June 2022 and May 2023. The primary aim of our study was to analyse the clinical profile, distribution of etiological factors, and pattern of clinical presentation among patients with cervical lymphadenopathy.
Additionally, we sought to evaluate the effectiveness of FNAC in relation to various etiological causes of cervical lymphadenopathy. and its correlation with histopathology and to find out the commonest aetiology of occult primaries.
The study consists of 80 cases. A minimum sample of 73 cases was needed to study the clinical profile, distribution of etiological factors, and pattern of clinical presentation among patients with cervical lymphadenopathy, considering that the prevalence of lymphadenopathy was 26% and precision 10%.
The sample size of the study was calculated from the reference article,[4]
Prevalence/Incidence of Cervical Lymphadenopathy: 26%[4] n = Z2 pq/e2 Z = Z score from 95% confidence interval=(1.96)2=3.84 e = marginal error = 10% n = 73 minimum required sample size Rounded off to n = 80
Patients above 18 years of age, presenting to our hospital with cervical lymphadenopathy and willing to participate in the study were included. Patients with a prior diagnosis of a confirmed head or neck cancer were excluded. The diagnosis was based on clinicopathological findings. Oral and written consent was taken from all patients. A thorough history was taken from all the patients and a complete ear, nose, and throat examination was done. FNAC and histological examinations were performed on patients with cervical lymphadenopathy. A correlation between the final histological diagnosis and the preoperative FNAC was made. In cases of neck lymph nodes suspected of being secondaries, an effort was undertaken to identify the primary tumour. The clinicopathological profile of all patients included in the study was analysed and compared with recent literature.
The statistical analysis was conducted using mean ± standard deviation for all continuous variables. The frequency and percentage of each categorical variable were used to represent them. Fisher’s exact test or the Chi-square test was used to compare categorical variables. Between FNAC and HPE, sensitivity and specificity were computed. Data was entered using a Microsoft Excel spreadsheet. The software used for data analysis was SPSS version 28.0. All P values < .05 were considered statistically significant.
Ethical approval was obtained from the Institution Review Board.
Results
In our study, the gender-wise distribution of the 80 patients included was observed, of which 39(49%) were males and 41 (51%) were females [Figure 1].
Sex distribution
In our study, 30 patients (37%) were between 18 and 35 years of age, 44 patients (55%) were between 36 and 60 years, and it was the most common age group, and only six patients (8%) were above 60 years of age. Among the patients between 18 and 35 years of age, tuberculosis (37%) was the most common cause of cervical lymphadenopathy, followed by reactive lymphadenopathy (30%) and Hodgkin’s Lymphoma (13%). Metastatic secondaries and other granulomatous conditions were 10% each. Tuberculosis (32%) and reactive lymphadenitis (32%) were both common among the patients between 36 and 60 years, followed by Hodgkin’s Lymphoma (16%) and metastatic secondaries (16%), followed by non-Hodgkins lymphoma (2%) and other granulomatous conditions (2%). Among patients over 60 years of age, it was observed in our study that Hodgkin’s Lymphoma (32%) and metastatic secondaries (32%) were more common, followed by reactive lymphadenitis (20%) and non-Hodgkin’s Lymphoma (16%) [Table 1].
The age-wise distribution of different aetiologies

Hence, our study observed that tuberculosis was more prevalent among the economically active age group, and lymphomas and metastatic secondaries were more common in older age groups [Table 1]. However, there was no association between age and disease statistically (P value .189)
Our study also observed that 81% of patients presented with unilateral cervical lymphadenopathy, and 19% presented with bilateral cervical lymphadenopathy. The right side of the neck was involved in 47% of patients, followed by 38% on the left side; bilateral involvement was seen in 9%, and the least involved was the central group, accounting for 6%.
Our study observed that 95% of cervical lymphadenopathy was mobile, and only 5% had restricted mobility.
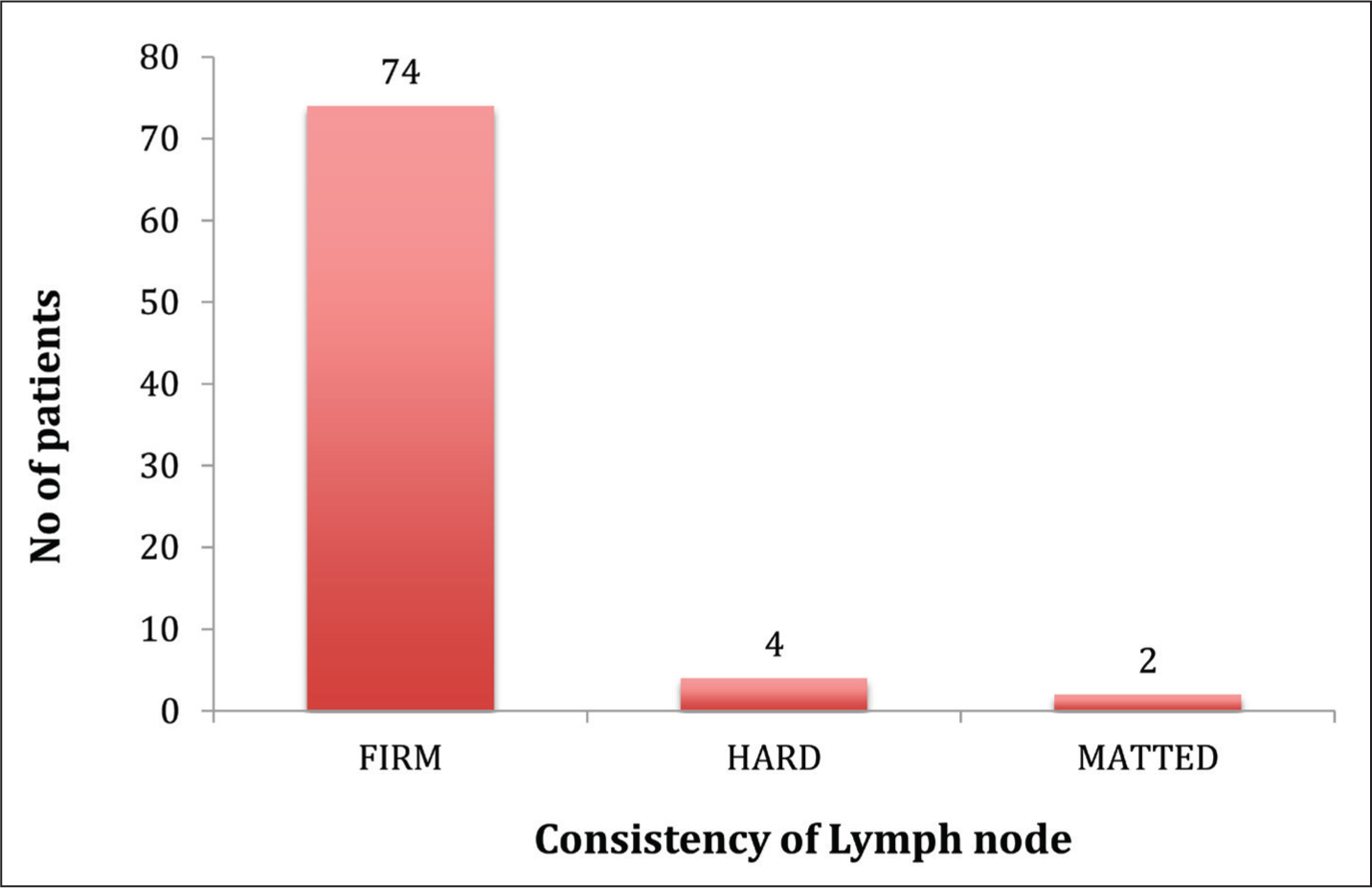
Among the 80 patients clinically examined in our study, 74 patients (92%) had firm consistency, four patients (5%) had hard consistency, and two patients (3%) had matted consistency [Figure 2].
Consistency of lymph nodes in cervical lymphadenopathy
In our study, 26 (33%) had swelling as their only symptom, 21 (26%) had swelling with fever, 20 (22%) had swelling with fever and pain, 13 (16%) had swelling with pain, and only 2 (3%) had swelling with voice change.
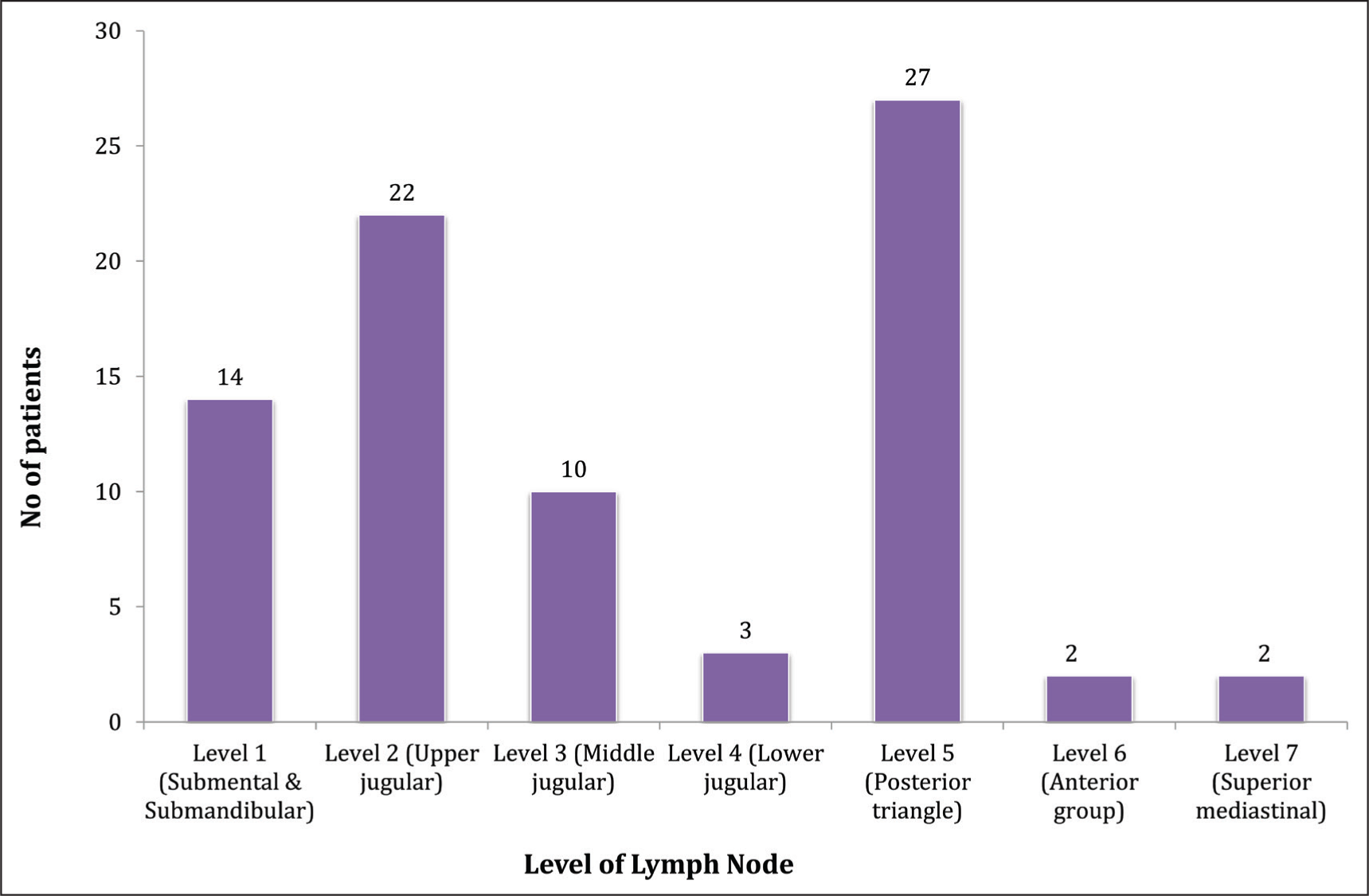
Our study observed that more cases involved level 5 (35%) and level 2 (28%) lymph nodes, followed by involvement of level 1 (18%) and level 3 (13%) [Figure 3].
Level of lymph nodes involved in patients
In this study, 33% of the cases were malignant and 67% were benign [Figure 4]. 16% of the malignant lesions were Hodgkin’s Lymphoma, 3% were non-Hodgkin’s Lymphoma, and 15% were metastatic secondaries.
Benign and malignant lesions in cervical lymphadenopathy
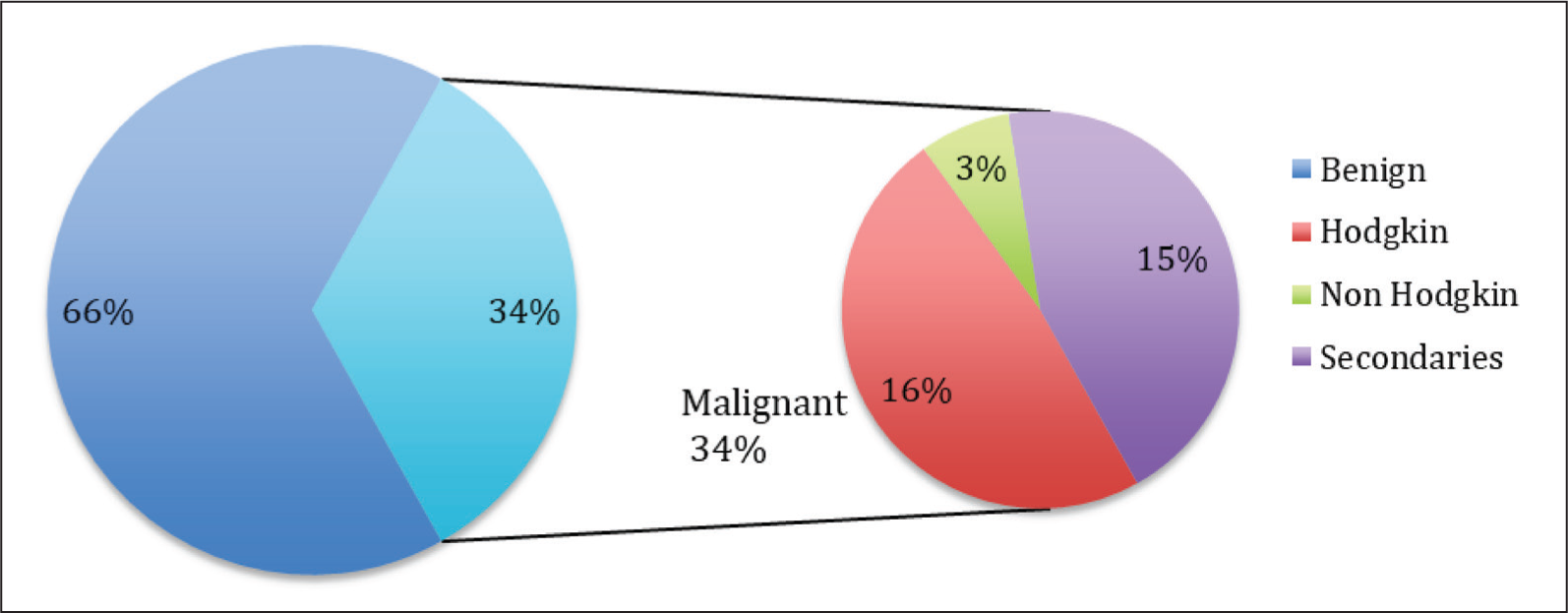
Reactive lymphadenitis (30%) was the second most common aetiology, after tuberculosis (31%). Among lymphomas (19%)- Hodgkins Lymphoma was more common than non-Hodgkins, metastatic secondaries (15%) and Other granulomatous conditions (5%) [Figure 4].
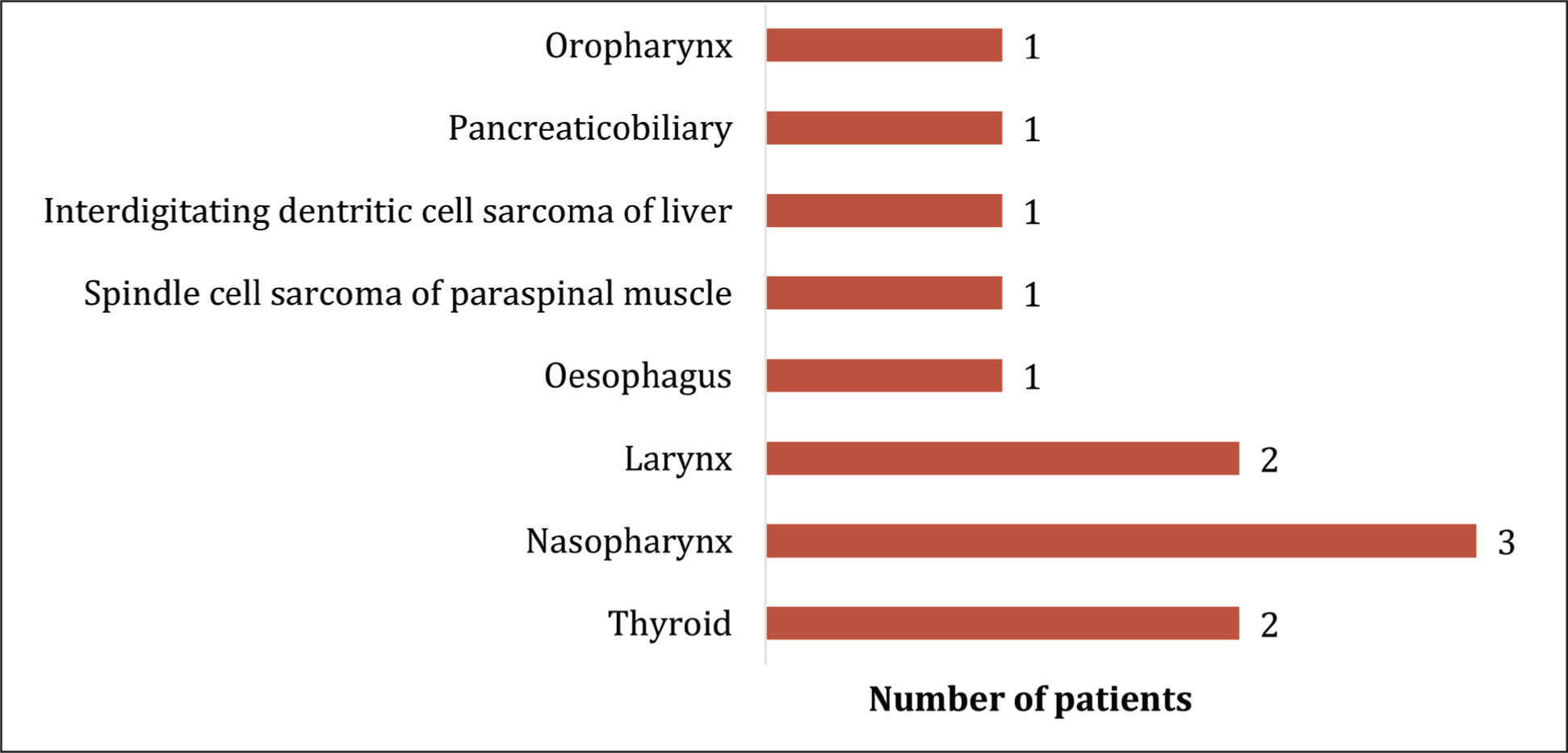
In our study, a total of 12 patients were confirmed to have metastatic secondary lymph node involvement based on histopathological assessment. Despite thorough clinical evaluations and comprehensive pan-endoscopic examinations, no primary tumour could be identified in these patients. Hence, these 12 patients were classified as occult primary with metastatic secondary nodes in our study. Following their biopsy, patients were referred to an oncologist, who further evaluated them with PET CT scans, which revealed increased FDG uptake with the probable primary sites of origin as detailed below, of which the most common site was in the nasopharynx (30%), followed by the larynx (20%) and Thyroid (20%). Other sites included the Oesophagus, Spindle cell sarcoma of paraspinal muscle, and Interdigitating dendritic cell sarcoma of the liver, Oropharynx and Pancreas, accounting for 10% each [Figure 5].
Primary site distribution in metastatic nodes (Based on PET CT Scan)
Among the metastatic nodes, level 2 was more commonly involved, as observed in our study.
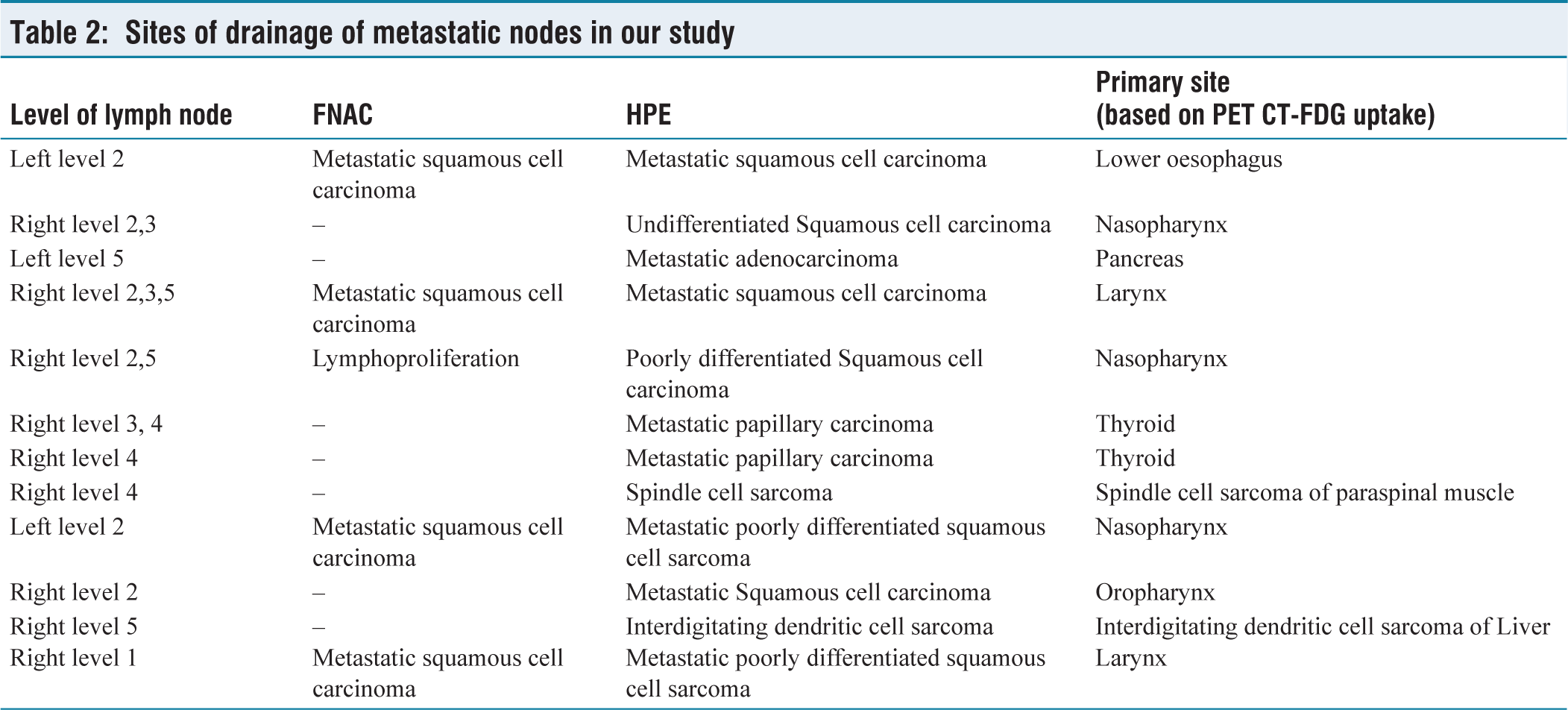
Out of the 12 patients with metastatic nodes, seven were histopathologically diagnosed with metastatic squamous cell carcinoma. The most common primary site was in the nasopharynx, followed by the larynx. Two patients had metastatic papillary carcinoma, and both had previously undergone total thyroidectomy several years ago, unrelated to malignancy. One patient had metastatic adenocarcinoma with the primary site in the pancreas. The other two patients were diagnosed with metastatic sarcoma with a possible primary site located in the paraspinal muscle and liver [Table 2].
Sites of drainage of metastatic nodes in our study
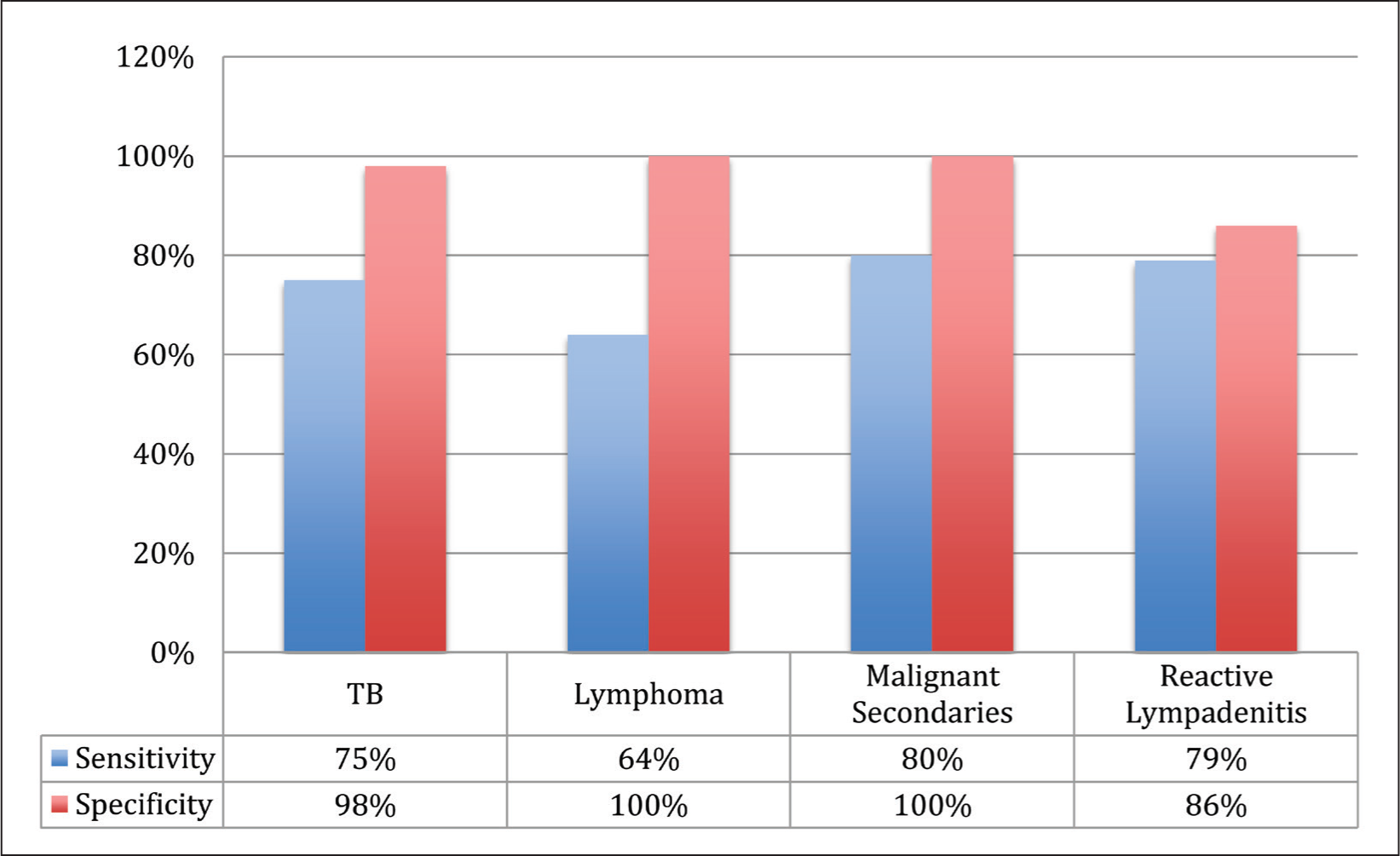
According to our research, FNAC exhibited 75% sensitivity and 98% specificity for TB detection, 64% and 100% sensitivity and specificity for lymphomas, 80% and 100% sensitivity and specificity for metastatic secondaries, and 79% and 86% sensitivity and specificity for reactive lymphadenitis. In our study, the overall FNAC sensitivity is 70.6% (68.5–72.7) with a 95% confidence interval [Figure 6].
Sensitivity and specificity of FNAC
Discussion
The evaluation of cervical lymphadenopathy is of significant importance in determining the accurate diagnosis and suitable treatment approaches, given the wide array of potential causes associated with this clinical condition. Males and females in our study were equally impacted, with a 1:1 M: F ratio. However, in most studies, there was a slight male preponderance. In a study conducted by Alam J et al.,[4] males were affected more, with M: F ratio being 1.9:1. In our study, the most predominant age group with cervical lymphadenopathy was 36–60 years, concordant with Maheshwari A et al.[5] Two studies were done by Alam J et al.[4] and Saurabh G et al.[6] had predominantly patients in 11–20 age group. On comparing the results of our study with the study conducted by Alam J et al.,[4] it was observed that TB was more common in 36–60 years of age in our study as compared to 18–35 years, as noted by Alam J et al. Lymphomas and metastatic secondaries were more common in 36–60 years of age in both studies, and both studies found that people between the ages of 18 and 35 had a higher incidence of reactive lymphadenitis. In our study, the right side of the neck was involved in 47% of patients, followed by 38% on the left, bilateral involvement was seen in 9% of patients, and the central group accounted for 6% of those that were least involved, which was consistent with the findings noted by Alam J et al.[4] This contrasts with the Bhavani et al. study.[7] which shows left-side involvement to be more common (50%). According to our study, 92% of cervical nodes were mobile, and only 5% presented with fixity. Alam J et al.[4] reported matting at 22.3%, fixity at 12.16%, and mobility at 65.54%. In our study, among the 80 patients clinically examined, 74 patients (92%) had firm consistency, four patients (5%) had hard consistency, and two patients (3%) had matted lymph nodes. However, among the 148 cervical lymphadenopathy patients clinically examined by Alam J et al.,[4] 111 patients (75%) had firm consistency, 25 patients (17%) had hard consistency, and 12 patients (8%) had rubbery consistency, In the Bhavani et al.[7] study, firm made up 70% and hard 28%. Firm nodes comprised 65.5%, hard nodes 29.1%, cystic nodes 3.6%, and soft nodes 1.8% in Chamyal et al.’s[8] study.
In our study, it has been seen that more cases have involved level 5 (35%) and level 2 (28%) lymph nodes, followed by involvement of level 1 (18%) and level 3 (13%). However, Alam J et al.[4] reported that more cases had involved level 2 (21%) and level 3 (20%) lymph nodes, followed by involvement of level 4 (17%). In a study by Maheshwari A et al.,[5] 25 patients (50%) presented with involvement of the level 2 lymph nodes, whereas 16 patients (32%) presented with involvement of multiple groups of lymph nodes. Further findings from our study revealed that lymph nodes in the level 2 and level 5 groups were frequently associated with lymphomas and tuberculosis.
In our study, of the 80 patients with cervical lymphadenopathy, 67% were benign, and 33% were malignant. Among the malignant lesions, 16% were Hodgkins Lymphoma, 3% were non-Hodgkins Lymphoma, and 15% were metastatic secondaries. In the study by Alam J et al.,[4] of 148 patients with cervical lymphadenopathy, 89% were benign, and 11% were malignant. A study by Haque et al.[9] showed that 25.3% were malignant, and the remaining were benign. Among the Benign lesions, tuberculosis was the most common aetiology concordant with studies by Alam et al.,[4] Maheshwari et al.,[5] Kulal et al.,[10] and Shrivastava et al.[11] Our study revealed a higher prevalence of tuberculosis among individuals from lower socio-economic backgrounds from the North East Belt. Additionally, among the 25 patients diagnosed with tuberculosis, only three had a prior history of the disease: one patient had a history of bone tuberculosis, and two patients had a history of pulmonary tuberculosis. The remaining patients had no previous exposure or the disease.
Our study also revealed a higher incidence of lymphomas (19%) among the patient population than in other studies. Additionally, it was noted that lymphomas frequently affected several nodes on the same side. This paradigm shift in the increase in lymphoma cases could be because our hospital is a specialised centre that receives referrals for complex cases. In our study, among the 12 patients with metastatic nodes, the most common primary site was noted to be the nasopharynx (30%), followed by larynx (20%) and thyroid (20%). Other sites included the Oesophagus, Spindle cell sarcoma of paraspinal muscle, Interdigitating dendritic cell sarcoma of the liver, Oropharynx and Pancreas, accounting for 10% each. Therefore, our study highlights the importance of not limiting the search for primary sites to the head and neck region alone when dealing with metastatic cervical nodes. In a study by Gorle VK et al.[12] among malignant secondaries, the primary was detected in the larynx (2), thyroid (2), and parotid (1). In another study by Gakhar S et al.,[6] it was observed that the most common site for the primary was Oropharynx (53%), followed by larynx (17%) followed by Hypopharynx (14%) and nasopharynx (7%). Further, in our study, it was observed that level 2 nodes were more commonly involved in metastatic nodes, concordant with the study by Zhou et al.[13] However, in a study by Guruswamy et al.,[14] level 5 nodes were more commonly involved. Our study’s FNAC sensitivity for tuberculosis is 75.5%, which is in line with that of Kulal P et al.,[10] and our study’s FNAC specificity for metastatic secondaries and lymphomas is 100%, which is in line with that of Alam J et al.,[4] Maheshwari A et al.[5] and Kulal P et al.[10]
Some of our study’s limitations include the need for a larger sample size for more reliable results. There is also the potential for observer variation, as FNAC procedures were not limited to our institution alone. As ours is a referral centre, it is plausible that this factor has contributed to the higher prevalence of lymphoma cases observed in our study.
After diligent analysis of our results, we observed a higher incidence of tuberculosis and lymphomas in the economically active population; hence, proceeding with an incisional biopsy is recommended if FNAC results are inconclusive. In situations where a diagnosis of reactive lymphadenitis is made through FNAC, it is advisable to proceed with an incision biopsy in persistent cases as it could potentially be identified as a granulomatous condition, lymphoma, or malignancy upon histopathological examination. As the overall sensitivity for FNAC is only 70.6%, it is advisable to go ahead with incisional biopsy when FNAC is inconclusive or not typically correlating with the clinical picture. This precautionary measure helps prevent unnecessary antibiotic usage and antibiotic resistance and ensures a precise diagnosis through histopathological examination.
Conclusion
Cervical lymphadenopathy is a common clinical problem that needs to be carefully assessed, analysed, and treated by medical specialists. Our study found that tuberculosis is the most common cause of cervical lymphadenopathy, which is consistent with the endemic nature of the disease in our country. Early and accurate diagnosis, as well as prompt management, are crucial in reducing the overall prevalence of the disease. Tuberculosis can be effectively treated with appropriate anti-tubercular drugs following accepted regimens. PET scans prove invaluable in detecting occult primary cancers. FNAC stands out as an initial, cost-effective diagnostic tool, particularly for the timely detection of malignancies. In order to improve patient outcomes by preventing delays in diagnosis and treatment, it is imperative to use strong clinical judgement while handling patients with cervical lymphadenopathy.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethics committee approval number
AMH-DNB-050/08-22.
Informed consent
Informed has been obtained from all the patients who met the eligible criteria.
Credit author statement
Dr. Preethi S collected data, acquired data computing, interpreted data, analysed data, drafted the article, and was accountable for all the aspects of the study.
Dr. Nithyana Narayanan: Conception of the idea, interpretation of data, analysis of the data, correction of the chart, and accountability for all the aspects of the study.
Dr. Venkatakarthikeyan C: Conception of the idea, interpretation of data, Review of the draft, final approval for the manuscript to be published, and accountability for all the aspects of the study.
Data availability statement
Data supporting the findings of this study are available from the corresponding author upon request.
Use of artificial intelligence
There was no use of Artifical Intelligence.