
Abstract
Background and Aims:
Single-sided deafness (SSD) is a severe type of hearing loss affecting one ear, and it frequently presents social difficulties for those affected. Head shadow effect and sound localisation play an important role in speech perception.
Methods:
Research articles on SSD were identified through an online search of PubMed, Scopus, Medline, and Google Scholar databases.
Results:
SSD affects daily activities and emotional or social well-being. It is necessary to get the early identification of the aetiology of SSD for prompt intervention. The aetiology of SSD can be determined with the use of investigations such as as genetic testing, serological testing, computed tomography (CT) scan, magnetic resonance imaging, and DNA testing for viral infections. Rehabilitation options for patients with SSD include cochlear implants, bone-anchored hearing aids, and contralateral routing of sound. Individuals with SSD cochlear implants have strong auditory perception. The objective of this review article is to provide aetiology, clinical presentations, diagnosis and current treatment of SSD.
Conclusion:
Individuals with SSD commonly experience communication issues that have a substantial negative effect on their quality of life. Word discrimination is hampered by SSD, and this impairment varies depending on the affected ear’s residual hearing. Speech comprehension is frequently difficult for patients with severe SSD, especially in noisy environments.
Introduction
Single-sided deafness (SSD) is a serious clinical entity that impairs a person’s ability to communicate.[1] SSD is defined as a clinical entity where a person has severe to profound hearing loss (≥70 dB HL) on the one side and nearly normal hearing on the opposite side (–10 to 15 dB HL).[2] In the adult age group, the most common aetiology for acquired SSD is idiopathic, with other potential aetiologies being cholesteatoma and infections, neoplasms at cerebellopontine angle, and rarely injury to head, autoimmune disorders, and Meniere’s disease.[3] Patients with SSD often face difficulties in the localisation of sound, and speech discrimination in noise is usually worsened by unilateral tinnitus.[1] The head shadow effect leads to a noticeable difficulty in hearing sounds on the affected side. SSD often causes social difficulties and is documented to hamper normal activities in school among children and emotional well-being of adult patients.[4] SSD severely hampers sound localisation and affects speech discrimination when the talker is standing on deaf side.[5] Patients with SSD are now included in the clinical indications for cochlear implants and bone conduction devices.[1] While bone conduction devices cannot fully restore binaural hearing, they can diminish the head shadow effect, enhance speech perception in noisy settings and improve sound localisation, thereby positively impacting quality of life. On the other hand, cochlear implants not only restore binaural hearing but also enhance quality of life, reduce tinnitus and improve both speech perception in noisy environments and sound localisation.[6] This review article aims to outline the aetiology, clinical presentations, diagnosis and current treatments for SSD.
Methods of Literature Search
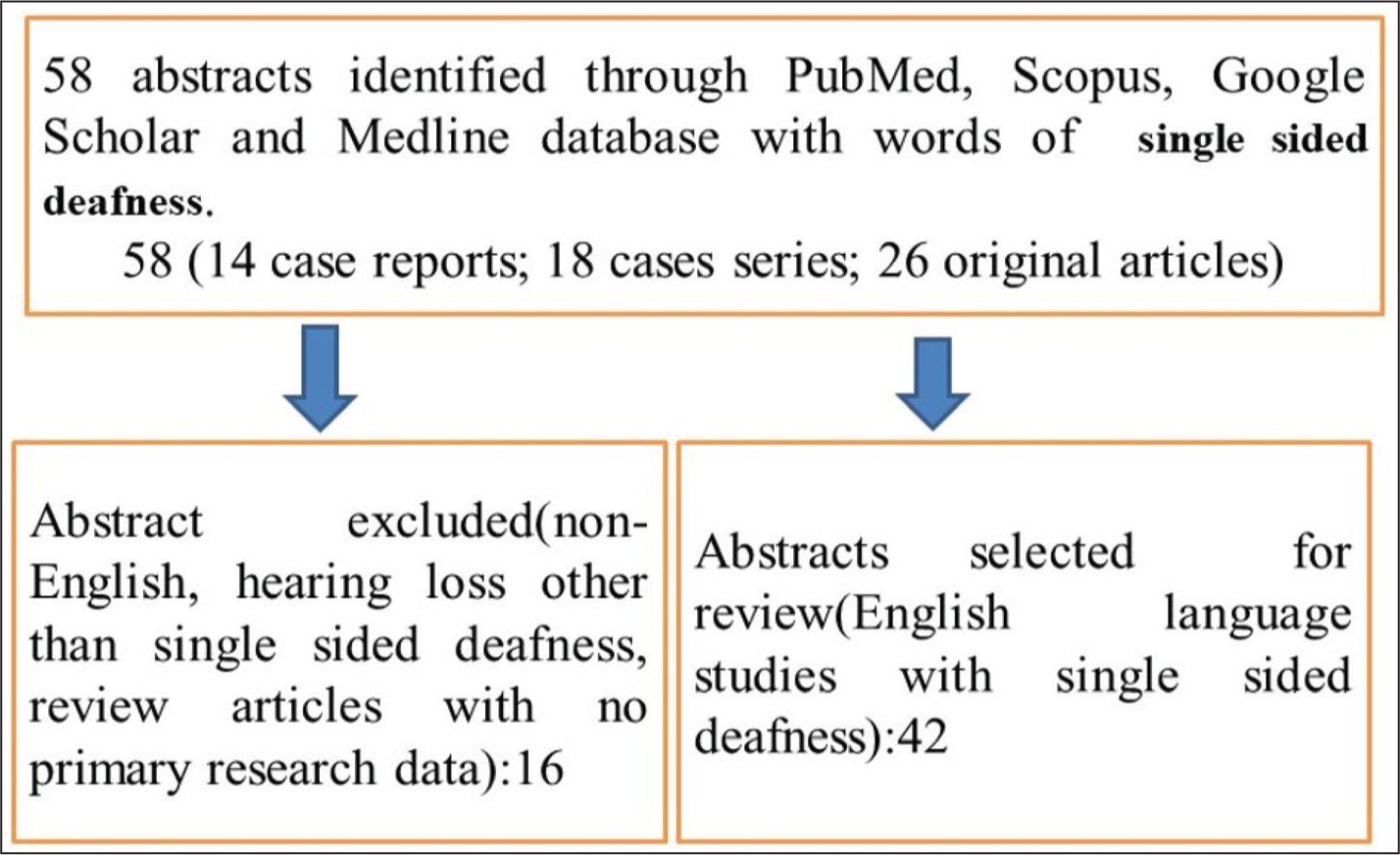
The search for recent research articles on SSD used several methodologies. We started by conducting an online search through the PubMed, Scopus, Medline and Google Scholar databases. We developed our search strategy on the basis of Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Although we also manually identified additional research articles from citations, our search approach focused on reviewing the abstracts of existing publications. We analysed various types of studies, including observational studies, comparative studies, randomised controlled trials, case series and case reports. In total, we reviewed 58 articles, comprising 14 case reports, 18 case series and 26 original articles [Figure 1]. This review article specifically concentrates on SSD. A better knowledge of SSD is provided by this review analysis. It will also catalyse further study and better awareness about SSD.
Methods of literature search
Epidemiology
Understanding the incidence and prevalence of SSD is crucial for directing clinical assessment, patient counselling, management and research endeavour. The exact global incidence of SSD is not known.[7] SSD has been found to affect 7.9% to 13.3% of general public.[8] According to a UK study, the annual incidence of adults diagnosed with SSD is estimated to be between 12 and 27 per 100,000.[9] However, another study estimated that the prevalence of SSD among adult civilians in the United States is 0.14%.[10] SSD is relatively common in newborns, occurring in 0.5 per 1,000 births.[11] The prevalence of SSD also rises with age.[12] According to reports, children with SSD of sensorineural hearing loss have a frequency of cytomegalovirus (CMV) infection ranging from 9.1% to 25%.[13] Each year, over 9,000 new cases of SSD are reported in the United Kingdom, whereas approximately 60,000 people with SSD are diagnosed in the United States.[14,15]
Etiology
Important causes of SSD include mumps, congenital CMV infection, meningitis, acoustic neuromas, inner ear malformations, cochlear nerve defects and auditory neuropathy spectrum disease.[16] A small percentage of SSD patients with certain aetiologies have progressing conditions.[17] Although cochlear nerve deficiency/hypoplasia was once thought to be an underdiagnosed condition, high-resolution magnetic resonance imaging (MRI) is now being used to identify it more frequently.[1] Children who are diagnosed with severe or profound hearing loss are substantially more likely to have auditory nerve deficits.[18] SSD is an extreme form of asymmetric hearing impairment. The central auditory system in SSD may be able to recognise itself because of the severely unbalanced input it gets from two ears.[19]
Clinical Presentations
Hearing Impairment in SSD
In SSD, there is a unilateral hearing loss; one can hear normally through the other ear. SSD significantly hampers word discrimination, which ranges from the function of residual hearing retained on the affected side.[20] When a patient has severe SSD, it might be difficult for them to understand speech, especially in a noisy surrounding, even when their hearing is normal on the normal side.[21] Patients with SSD encounter various challenges in daily life, particularly in noisy environments. These difficulties include locating sound sources, positioning themselves to enhance hearing and dealing with physical issues such as tinnitus and vertigo.[22] SSD can occur at any age group; most cases of SSD are of a sudden onset, affecting both the nerves and the inner ear, and usually irreversible.[1] The patient frequently loses sound localisation in SSD. Sound localisation necessitates binaural hearing. Speech processing also depends on binaural hearing.[23] Individuals diagnosed with SSD have notable impairments in spatial hearing. People with SSD experience reduced sound awareness, trouble understanding speech in loud situations, difficulties in localising auditory events and increased listening effort as compared to normal hearers.[24] Similar to sound localisation, the head shadow effect plays an important role in speech perception.[25] One significant association of hearing loss is tinnitus. To understand how tinnitus affects someone’s day-to-day activities, the condition can range in intensity from moderate to severe. Tinnitus affects most SSD sufferers to some extent. The benefits of summation effects (redundancy of auditory input), head shadow effect and binaural squelch (the brain’s capacity to distinguish sound and noise signals from spatially distinct sources) are not available to SSD sufferers. The combined effects of these disabilities have a significant influence on day-to-day functioning, particularly in social interaction and communication.[26] The impact of SSD can extend to all family members as patients often become more reliant on them. Additionally, patients may face difficulties adjusting to changes in communication quality after diagnosis, which can alter the family dynamics. This effect on family members owing to a newly diagnosed condition is known as third-party disability.[27] Individuals with SSD may experience a range of negative emotions, including denial, anger, isolation, depression and resentment. They may also feel jealous of their normally hearing partners, who may have more favourable interactions with other hearing family members.[28] Children with SSD suffer from difficulty in the intelligibility of speaking, determining the side of sound coming from and auditory perception, particularly in crowded and multi-sound sources environments.[29]
SSD and Speech Perception
Bilateral hearing is required for speech perception.[30] The redundant data from two separate acoustic sensors are acquired, enabling suppression and summation. When both ears receive identical auditory stimuli, binaural summation occurs. A 2- to 6-dB signal threshold is produced by the increased auditory processing of redundant information, which is especially helpful in a loud environment.[30] A type of higher order auditory processing known as the ‘squelch effect’ occurs when noise from one ear that perceives a lower signal-to-noise ratio is coupled with noise from another ear that perceives a higher signal-to-noise ratio.[31] This helps to distinguish speech from noise and is crucial for separating meaningful sound from background noise. The head shadow effect can be just as crucial for speech perception as it is for sound localisation.[32] Contralateral routing of sound (CROS), CI devices and bone-anchored hearing aids (BAHAs) are among the SSD rehabilitation methods that are available; these help to compensate for head and shadow effect deficiencies. On the afflicted side of deafness, each of these devices has an auditory sensor.
Psychological Impact of SSD
The diagnosis of SSD is a transformative event for both patients and their families. SSD diagnosis often leads to certain negative outcomes in a patient’s life. In SSD, patients often suffer from the disruption of spatial aspects of hearing, which disturbs the ability to understand speech in the background sound. The functional results in SSD are associated with different ranges of psychological and social manifestations. There are psychological and social implications of SSD caused by the handicap of hearing loss. Patients with SSD are prone to higher stress levels in social settings with an increased chance of social isolation.[33] There may be a myriad of negative experiences and emotional problems such as anger, denial, isolation and impatience. After a diagnosis of SSD, couples may experience marital turbulence because of heightened emotional and relational issues, which can lead some to consider separation or divorce. Persons with SSD have reduced confidence, hearing fatigue, decreased self-esteem and poor quality of life.[34] Patients have experience with different psychosocial consequences. Those with SSD frequently report heightened anxiety about losing hearing in their other ear, embarrassment because of the social stigma associated with hearing impairment and reduced social interaction.[35] Patients with SSD may encounter difficulties with their children after diagnosis. Children often experience frustration and annoyance because they feel that they are not being heard properly or must repeat themselves frequently.
Diagnosis
Early diagnosis of SSD is helpful for aetiology-specific rehabilitation and improved outcomes. In children, behavioural audiometry test assesses the sound localisation ability. Radiological investigations for SSD may be useful, specifically in the cases of anatomical abnormalities of the inner ear and auditory nerve. A CT scan is useful for identifying abnormalities in the middle and inner ear, whereas an MRI is crucial for diagnosing issues with the cochlear nerve. Auditory nerve deficiency is associated with a narrow bony auditory nerve canal and is usually found anatomical abnormality accounting for causation of SSD.[36] The incidence of anatomical anomalies of the inner ear and middle ear thought to be dependent on the severity of hearing impairment.[37] Preoperative work-up for SSD involves radiological imaging to find out the aetiology of hearing loss. One study showed that imaging of SSD in children revealed 28.9% abnormal anatomy of temporal bone in CT scans.[38] Serological testing and DNA testing are done for viral infection and genetic testing.
Imaging and Brain Plasticity in SSD
The importance of radiological investigations in SSD is quite limited. Both in non-auditory linked parts and auditory-related areas, there is growing evidence for brain plasticity. Using an auditory memory test, a magnetoencephalographic imaging investigation revealed reduced gamma band oscillations in the occipital lobe but enhanced theta band oscillations across the left superior temporal cortex.[39] In the cases of adult-onset SSD, functional and entropy connectivity changes are noted in the primary auditory cortex and other areas, such as the occipital lobes, during resting state functional MRI (fMRI).[34]
Treatment
Appropriate intervention is needed as per the aetiology of the SSD. The first step in offering the right treatment for SSD is aetiology clarification. Patients of SSD require expertise from several areas such as an audiologist, ENT, speech therapist and psychologist. Cochlear implants, BAHA and CROS are among the SSD therapeutic options.[40] The head shadow effect and the non-hearing side’s perception of sound are two of the SSD deficiencies that are mitigated by these three modalities. Additionally, they enhance hearing in loud environments. A traditional hearing aid is not an option for treating the SSD. Traditional hearing aid amplifies the sound, where the amplified sound is heard as distortion. BAHA is a surgically implanted device that uses direct conduction to transmit sound from the affected ear to the normal side. In comparison to CROS and BAHA, only cochlear implants offer the potential to restore binaural hearing and helpful sound localisation.[41] Most patients with SSD present with some degree of tinnitus. If the cause of the hearing loss is confined to the inner ear, a cochlear implant is likely to result in a positive hearing outcome. A microphone and transmitter-equipped hearing aid called a CROS is worn on the afflicted ear as a nonsurgical therapy option. The acoustic signal from this hearing aid is sent to a receiver inside a hearing aid worn in the better hearing ear. In addition to the CROS input, the better-hearing ear’s hearing aid can provide amplification if contralateral hearing loss is present. When a person has mild-to-moderate aid-able hearing loss on their contralateral (better hearing) side, they may employ a set-up known as BiCros. Despite this benefit, the acceptance and adoption rates of CROS hearing aids are less in the SSD population. Many of the early acoustic restrictions connected with CROS and BiCros hearing aids have been addressed by the substantial advancement of CROS hearing devices. Seamless between-ear signal transmissions have been made possible by advancements in hearing aid technology and design. The hearing outcome is less likely to better when the cause is located in the central auditory system or auditory nerve. After cochlear implantation, tinnitus becomes less severe.[42] Individuals with a cochlear implant in one ear and normal hearing in the other provide a unique opportunity to study sound encoding and adaptation with a cochlear implant. Although CI is a promising treatment for SSD, it cannot be used in all cases of SSD. A functioning cochlear nerve must be intact for a CI to restore the hearing.[43] In many cases of surgical treatment of vestibular schwannoma, the cochlear nerve is removed to ensure the complete excision of the tumour. If the auditory nerve is preserved, CI may be an option for SSD after the surgical removal of vestibular schwannoma. The cochlear nerve is usually preserved anatomically in the cases of radiosurgery for vestibular schwannoma. SSD patients with certain aetiologies have progressing conditions that can be managed by CI where long term results reveal that CIs provide a durable relief of hearing loss and tinnitus.[44]
Conclusion
Patients diagnosed with SSD face difficulties in communication and social challenges. Patients with SSD have trouble communicating because they have trouble localising sounds and understanding speech when there is background noise. It can lead to a range of emotional and negative experiences, including denial, anger and impatience. So, many patients require rehabilitation options. Currently, CROS, BAHA and CI are the most frequently used options for SSD. Through their ability to eliminate the head shadow effect, these treatment methods provide a substantial advantage. Additionally, voice perception in quiet and noisy environments has improved because of sound localisation.
Footnotes
Acknowledgements
Author is thankful to all of his postgraduate students for their encouragement to write this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Institutional ethical committee
Not applicable.
Credit author statement
Dr Santosh Kumar Swain: Concept, literature search, data acquisition, manuscript preparation, manuscript editing, and approval of the version to be published.
Data Availibility
Not applicable.
Use of artificial intelligence
Not applicable