
Abstract
Introduction:
A plethora of pathologies can cause medial ankle pain.
Material and methods:
We present a case of 66-year-old male with medial ankle pain.
Result:
Bilateral CTEV (Congenital talipes equino varus) with impingement between the navicular and medial malleolus was present, which was contributing to medial ankle pain.
Conclusion:
One needs to be aware of this rare form of impingement in patients with medial ankle pain.
Keywords
Introduction
A plethora of pathologies can cause medial ankle pain, which commonly arises due to pathologies of the flexor tendons, most notably the tibialis posterior, deltoid ligament, spring ligament or flexor retinaculum. Tarsal tunnel syndrome and tarsal coalitions may also present with a painful medial ankle. We describe a rare cause of medial ankle pain due to impingement between the medial malleolus and navicular.
Case Report
A 66-year-old male presented with a 6-month history of insidious onset of medial ankle pain. There was no history of trauma or any significant systemic illness. He had a history of neglected bilateral CTEV (congenital talipes equino varus).
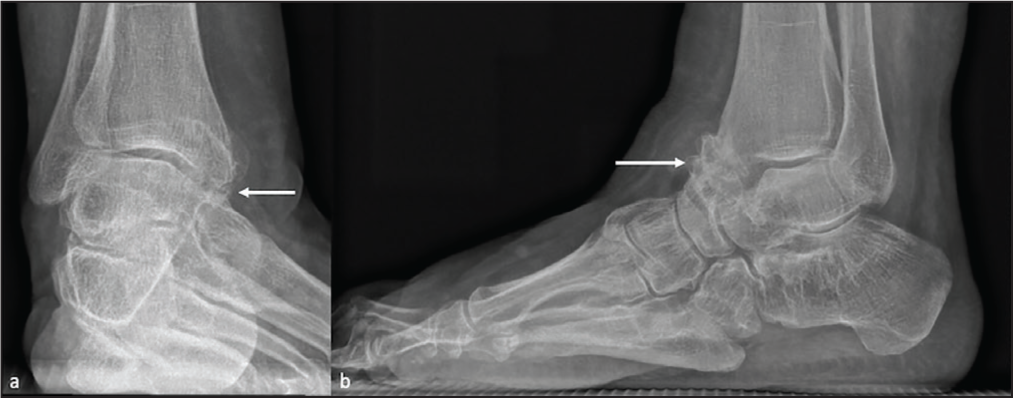
A radiograph of the right ankle showed marked forefoot, midfoot and hindfoot adduction deformity in keeping with sequalae of neglected CTEV (Figure 1). There was pseudo-articulation between the medial part of the navicular and medial malleolus with degenerative changes in the form of marginal osteophytes, subarticular sclerosis, as well as, cystic changes. Weight-bearing CT of both feet confirmed the same deformity bilaterally with impingement of the medial malleolus and navicular as a consequence of neglected CTEV (Figures 2 and 3). The patient was managed symptomatically.
Anteroposterior oblique (a) and lateral (b) radiographs of the right ankle marked deformity of the foot with impingement of the medial malleolus and navicular (arrow)
CT coronal (a) and sagittal (b) images of the right foot showing a marked deformity of the foot with impingement of the medial malleolus and navicular. Degenerative changes at the pseudo-articulation are identified with the presence of osteophytes, subchondral cysts and sclerosis (arrow)

Lateral oblique radiograph (a) and sagittal oblique CT (b) of the left foot showing impingement of the medial malleolus and navicular (arrow)

Discussion
Neglected CTEV is a problem seen predominantly in developing countries due to relatively poor access to medical services and poverty. Delayed CTEV presentation can be neglected CTEV (no treatment) or relapsed CTEV, which could be due to incompletely treated CTEV or due to the physiological growth of a person. The deformity gets progressively worse in neglected CTEV due to contracture of the medial structures while walking resulting in secondary deformation of bones. There is medial angulation of the talar neck and articulation of the talar body with the navicular. There is inversion, adduction and supination of the subtalar joint.[1] In our case due to extreme adduction and inversion of the hindfoot, there was impingement between the navicular and medial malleolus resulting in degeneration at the neo-articulation. This resulted in medial ankle pain which was managed nonoperatively. Conservative treatment includes oral analgesics, physiotherapy along with appropriate tailor-made footwear with the help of a podiatrist. A steroid injection of the neo-articulation may be attempted for pain relief before offering a surgical alternative. In our case, considering the advanced age of the patient, conservative management was preferred.
The various impingements of the ankle and hindfoot include anterior impingement, posterior impingement, anterolateral impingement, anteromedial impingement, posterior impingement, subfibular impingement and impingement at the level of the angle of Gissane.[2]
The various sequela of neglected CTEV include marked deformities, abnormal gait, dorsal bunion, secondary degenerative change, pseudoaneurysm, collapse of talus and pressure sores.[3]
Conclusion
One needs to be aware of navicular-medial malleolus impingement—a rare form of ankle impingement as a cause of medial ankle pain.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
No ethical committee approval was required as its a case report with anonymised images.
Informed consent
Anonymized images used.
Credit author statement
All authors contributed significantly towards the project.
Data availability
Not applicable.
Use of artificial intelligence
No.