
Abstract
Introduction:
Xanthogranulomatous oophoritis is a rare ovarian inflammatory disorder characterised by the extensive infiltration of foamy macrophages and chronic inflammation in the ovarian stroma.
Background:
We report two cases of xanthogranulomatous oophoritis, both of 34 years of age with complaints of chronic pelvic pain with infertility and with abnormal uterine bleeding.
Aim:
This case study aims to explore the clinical and pathological features of this rare condition while highlighting the challenges in diagnosis and management.
Introduction
Xanthogranulomatous oophoritis is a rare pathological entity, with only a limited number of cases reported in the literature.[1] This inflammatory disorder is characterised by a histological pattern resembling other xanthogranulomatous inflammation, consisting of lipid-laden foamy macrophages, lymphocytes and plasma cells within the ovarian tissue. The aetiology and pathogenesis of this condition remain unclear, and the diagnosis is often challenging due to its rarity and similarity to other ovarian disorders.[2]
We report two cases of similar age who presented at our outpatient Department of Gynaecology, both of whom were diagnosed with this uncommon condition.
Case Report
Case 1: A 34-year-old female presented to the gynaecology clinic with a 2-month history of chronic pelvic pain and failure to conceive. Pelvic ultrasound showed a bulky uterus with subserosal fibroids along with a large right ovarian cyst with uterine and lateral pelvic wall adhesions.
Subsequently, the patient underwent diagnostic laparoscopy. Intraoperative findings revealed a right enlarged ovary adherent to the uterus medially and with a right lateral pelvic wall.
Laparoscopic right cystectomy and adhesiolysis were performed, and the specimen was sent to the Pathology Department for further evaluation.
Gross examination showed a right ovarian cyst measuring 7.0×6.0×0.4 cm. Outer surface was smooth grey-white, on cut a unilocular cyst was noted, with focal grey-brown areas. Wall thickness was 0.2 cm.
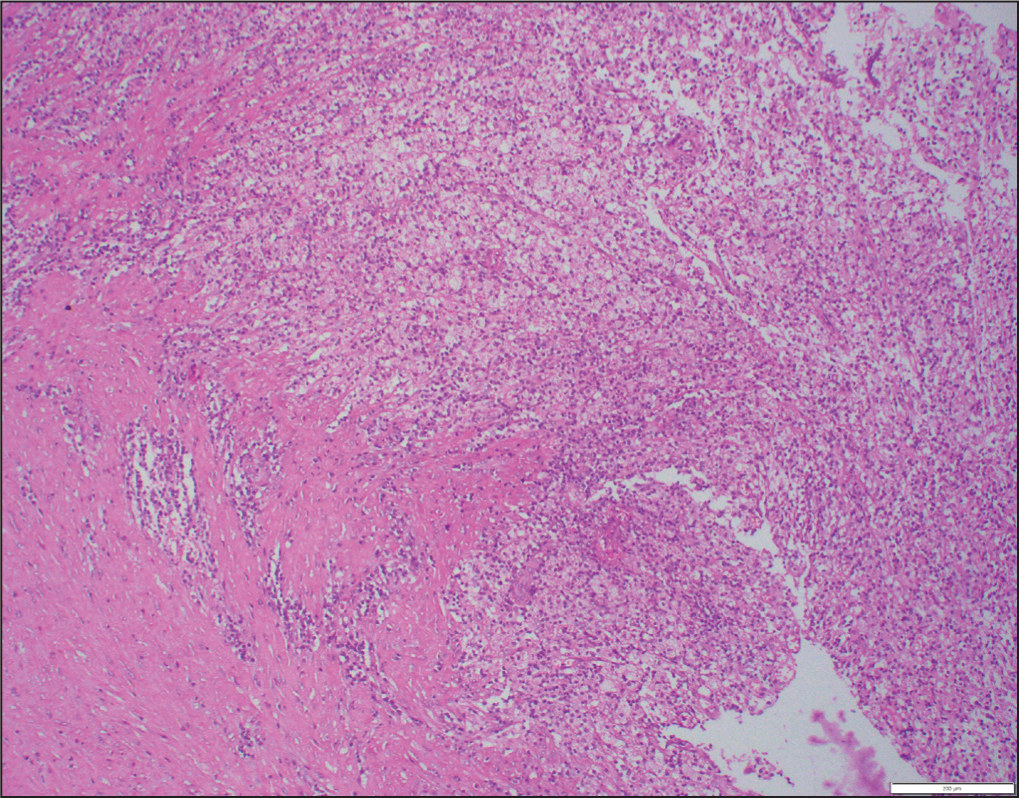
Microscopic examination of Haematoxylin and Eosin (H&E) stained sections revealed extensive infiltration of the ovarian stroma by sheets of foamy macrophages, chronic inflammatory cells and multinucleated giant cells. Surrounding areas showed fibrosis and focal areas of haemorrhage [Figure 1].
H and E: 200x: Case 1, sheets of foamy histiocytes with lymphomononuclear infiltrate
Case 2: Another 34-year-old woman, with completed family, presented to the gynaecology, outpatient department with complaint of abnormal uterine bleeding and chronic pelvic pain.
This patient underwent a hysterectomy with bilateral salpingectomy along with a cystectomy of the left ovarian cyst.
Gross: Uterus and cervix measured 10×7.5×5.5 cm. Cut section of the uterus showed thickened endometrium. Fallopian tubes were grossly, unremarkable and each measured 5 cm in length. A Fragmented cyst was received, separately, all together measuring 6×4.8×1.1 cm, wall thickness of the ovarian cyst ranged from 0.4 cm to 0.8 cm. Representative sections were taken. Multiple sections from the ovarian cyst wall were taken.
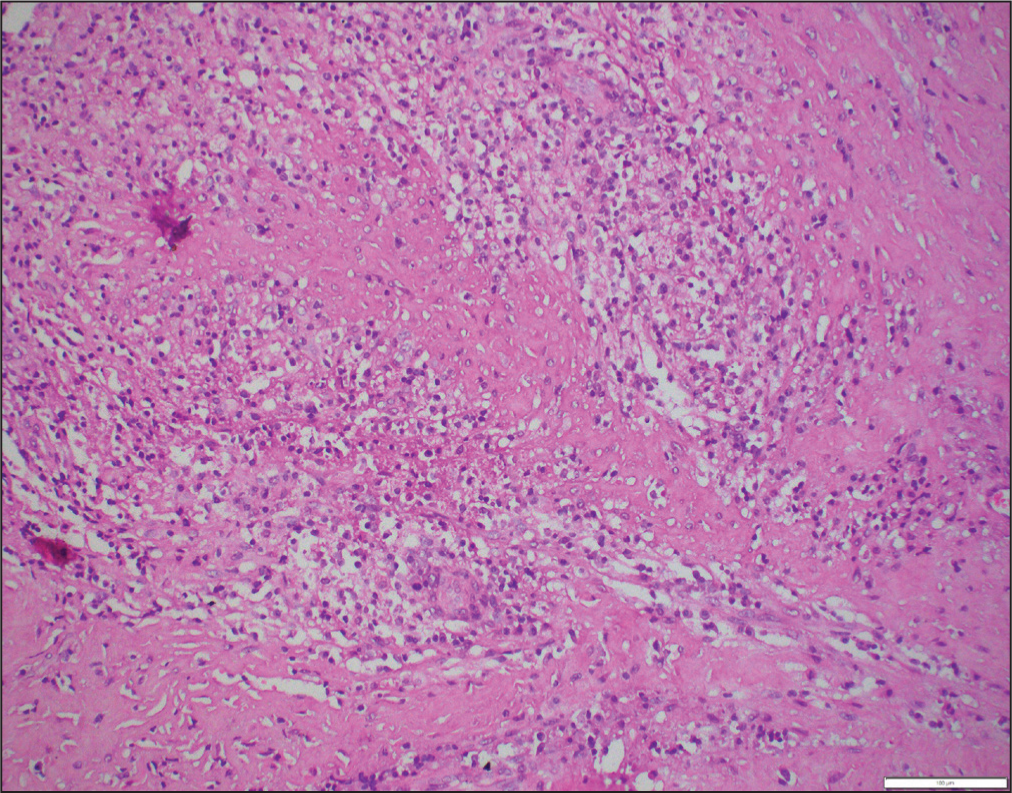
Microscopic examination of H&E sections from uterus showed endometrial hyperplasia with adenomyosis. Multiple sections from the ovarian cyst wall showed infiltration with foamy histiocytes along with mixed inflammatory infiltrate and fibrosis. However, no endometrial glands and stroma were seen. Bilateral fallopian tubes were unremarkable [Figure 2].
H and E: 200x: Case 2, sheets of foamy histiocytes with fair number of plasma cells and multinucleate giant cell
Ziehl Neelsen stained sections of ovarian cysts from both the above cases, were negative for acid fast bacilli.
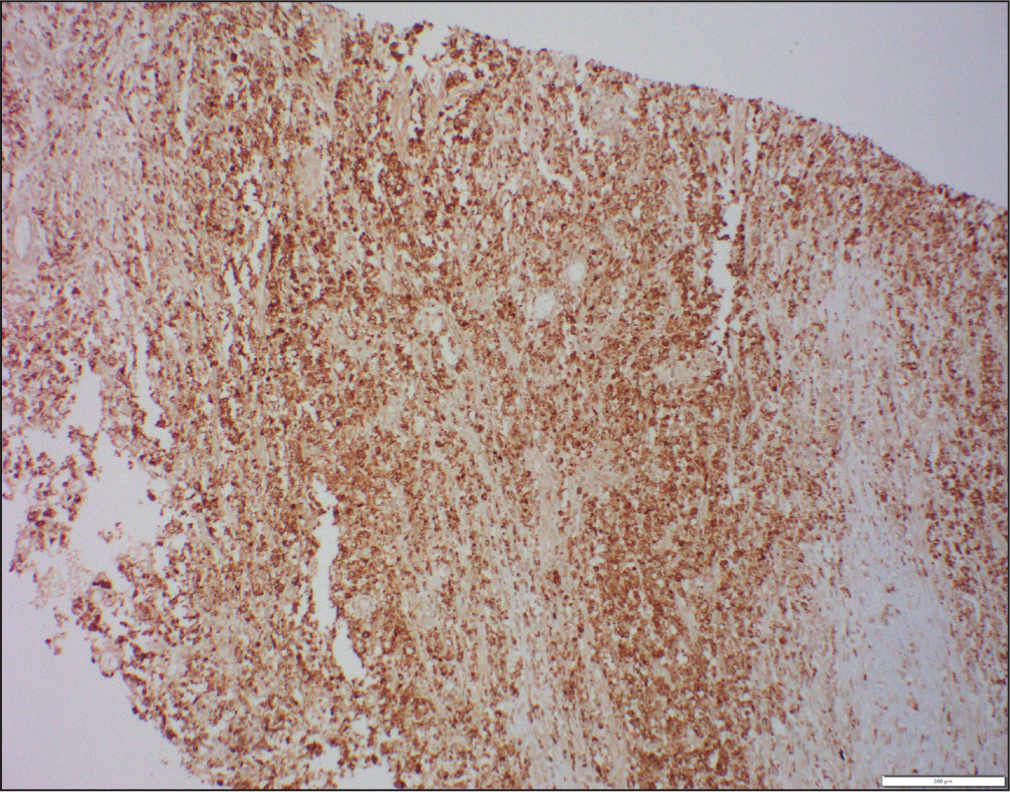
Immunohistochemical staining was performed, which demonstrated the presence of sheets of CD68-positive macrophages [Figure 3].
Immunohistochemistry CD68: 200x: cytoplasmic positivity in sheets of histiocytes
Surrounding areas showed an admixture of CD3 and CD20-positive small lymphocytes. Based on these findings, a diagnosis of xanthogranulomatous oophoritis was made.
Discussion
Xanthogranulomatous oophoritis is a rare form of chronic oophoritis often masquerading as other ovarian disorders. Only 100 cases have been reported in the literature, of which the first case of xanthogranulomatous oophoritis was reported in 1968 by Roth.[3]
It affects fallopian tubes or ovaries focally or entirely, which clinically forms mass-like lesion in the pelvic cavity and invades the surrounding tissues.[4,5]
Most commonly, females of reproductive age group are affected, however, it can occur at any age, ranging from 23 to 72 years.[6]
A long-standing history of pelvic inflammatory disease and symptoms such as anorexia, fever, suprapubic pain, menorrhagia, vaginal bleeding and infertility are the usual chief complaints.
In the female genital tract, the endometrium is most commonly affected by xanthogranulomatous inflammation, followed by, vagina, cervix, fallopian tubes and ovary.
The aetiology and pathogenesis of this condition have been the subject of numerous hypotheses, some of which include endometriosis, infections, intrauterine devices, inborn abnormalities of lipid metabolism in macrophages, antibiotics, as well as potential combinations of these factors. These conditions lead to degeneration of ovarian tissue or tissue necrosis resulting in the ongoing release of lipids and cholesterol from the dead cells. The xanthomatous process begins as a result of macrophages phagocytosing these biochemical components, as a subsequent inflammatory response.[7,8]
Gynaecologists need to be aware of this entity and be able to differentiate it from other ovarian disorders. Increased awareness and familiarity with the histopathological characteristics of xanthogranulomatous oophoritis are crucial in ensuring accurate diagnosis and appropriate patient management. A delayed diagnosis may lead to unnecessary surgical interventions and infertility-related distress.[9]
Conclusion
These cases highlight a rare presentation of xanthogranulomatous oophoritis in young female patients, emphasising the difficulties in diagnosis and potential implications for fertility. Clinicians and pathologists need to consider this uncommon entity when evaluating patients with chronic pelvic pain and ovarian masses. Raising awareness and reporting such cases will contribute to a better understanding of the pathogenesis, appropriate diagnosis, and optimal management of xanthogranulomatous oophoritis.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Ethical approval from relevant committee or Institutional Review Boards (IRBs) was obtained: Approval Number R/22/2023.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Credit author statement
Dr Kavita Somani: Case diagnosis and written by.
Dr Pretty Singh: Drafting and critical appraisal.
Data Availibility
Not applicable.
Use of Artificial Intelligence
No.