
Abstract
Introduction:
Haemoperitoneum due to spontaneous splenic rupture is a rare condition.
Methods:
We present a case of AL-type amyloidosis and chronic kidney disease (CKD) who is presented with diffuse abdominal pain. A contrast-enhanced CT scan of the abdomen revealed moderate to large amounts of free fluid in the peritoneum, indicating splenic rupture causing haemoperitoneum.
Result:
The patient underwent emergency exploratory laparotomy and splenectomy. After the operation, the patient was closely monitored in the ICU and was transferred to the ward on postoperative day 3. He was discharged home on day 6.
Conclusion:
This case report highlights a rare occurrence of haemoperitoneum secondary to spontaneous splenic rupture in a patient with AL amyloidosis.
Introduction
Splenic rupture is frequently observed in patients with blunt abdominal trauma, but spontaneous splenic rupture (SSR) is a rare occurrence. The hypovolemic shock associated with SSR contributes to a 10% mortality rate.[1] Amyloidosis is characterised by accumulating low molecular weight, highly organised fibrils outside cells. These fibrils are derived from proteins that are typically found in the bloodstream. When these fibrils are stained with Congo red and viewed under polarised light microscopy, they exhibit apple-green birefringence.[2,3]
Case Report
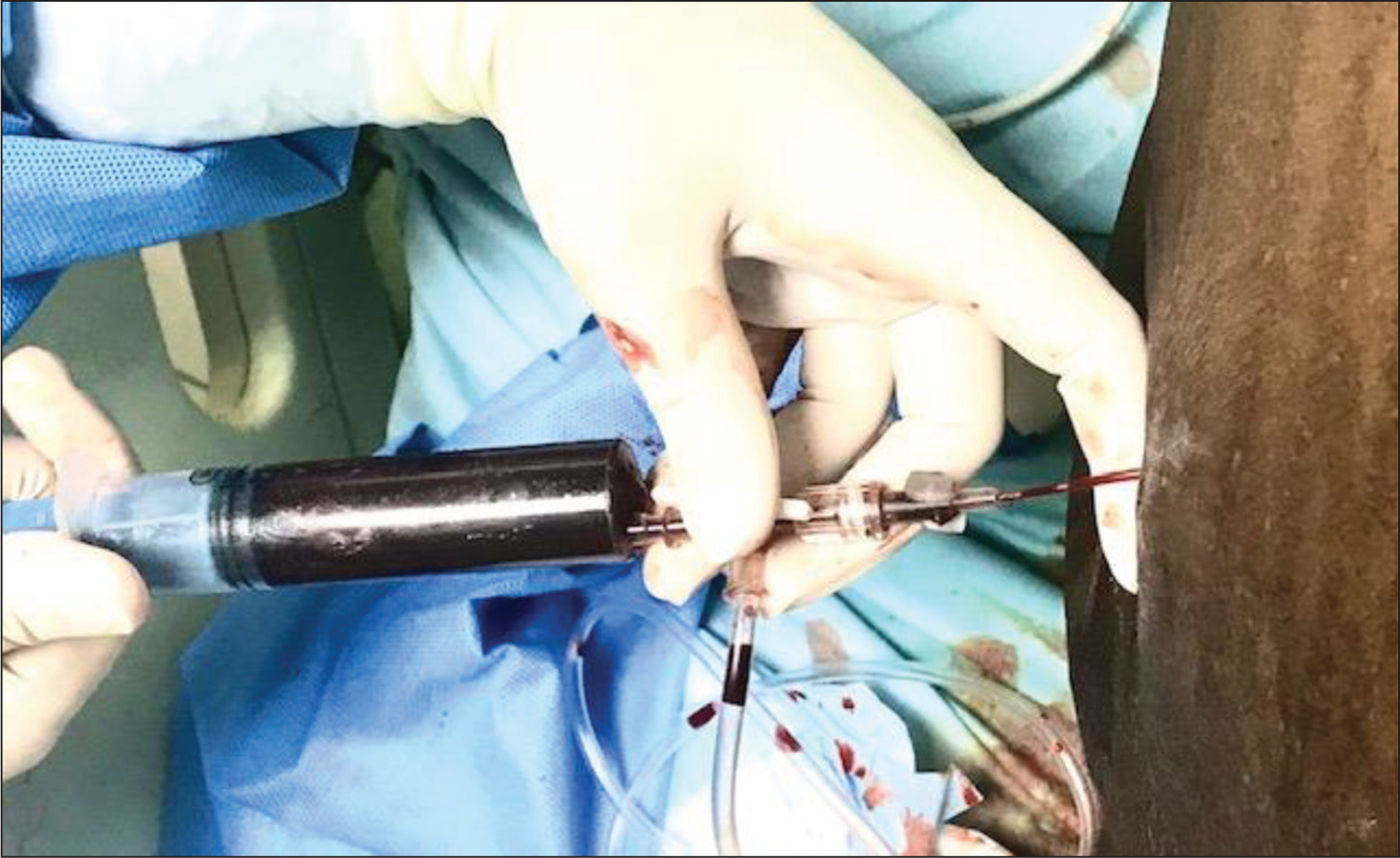
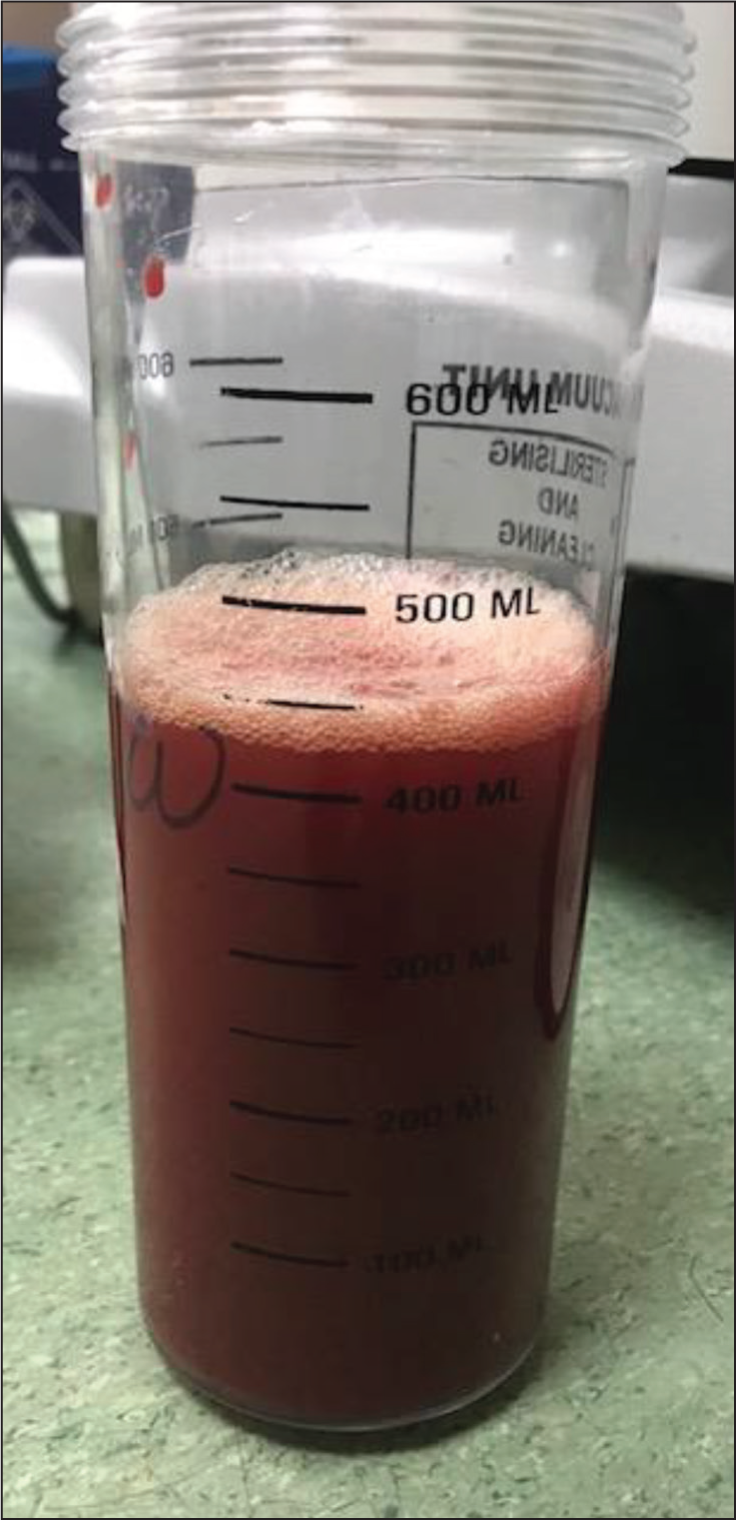
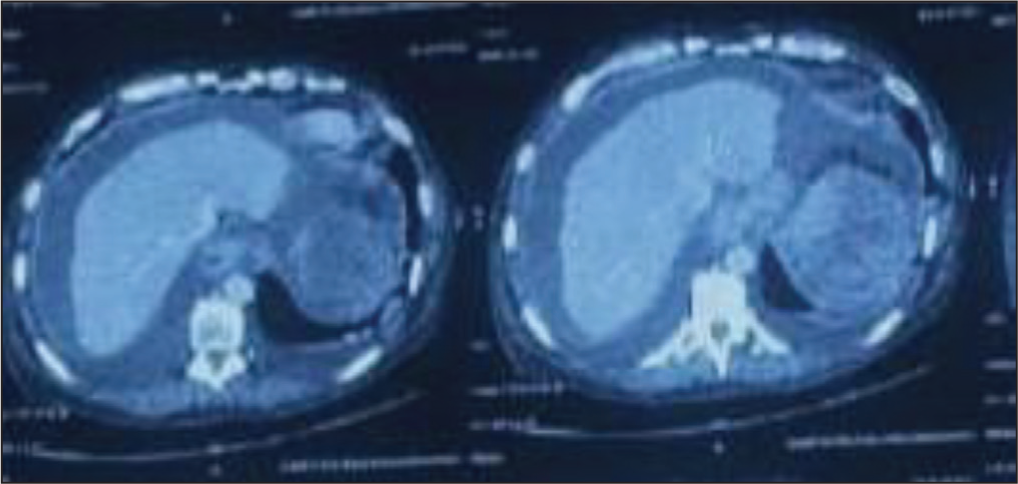
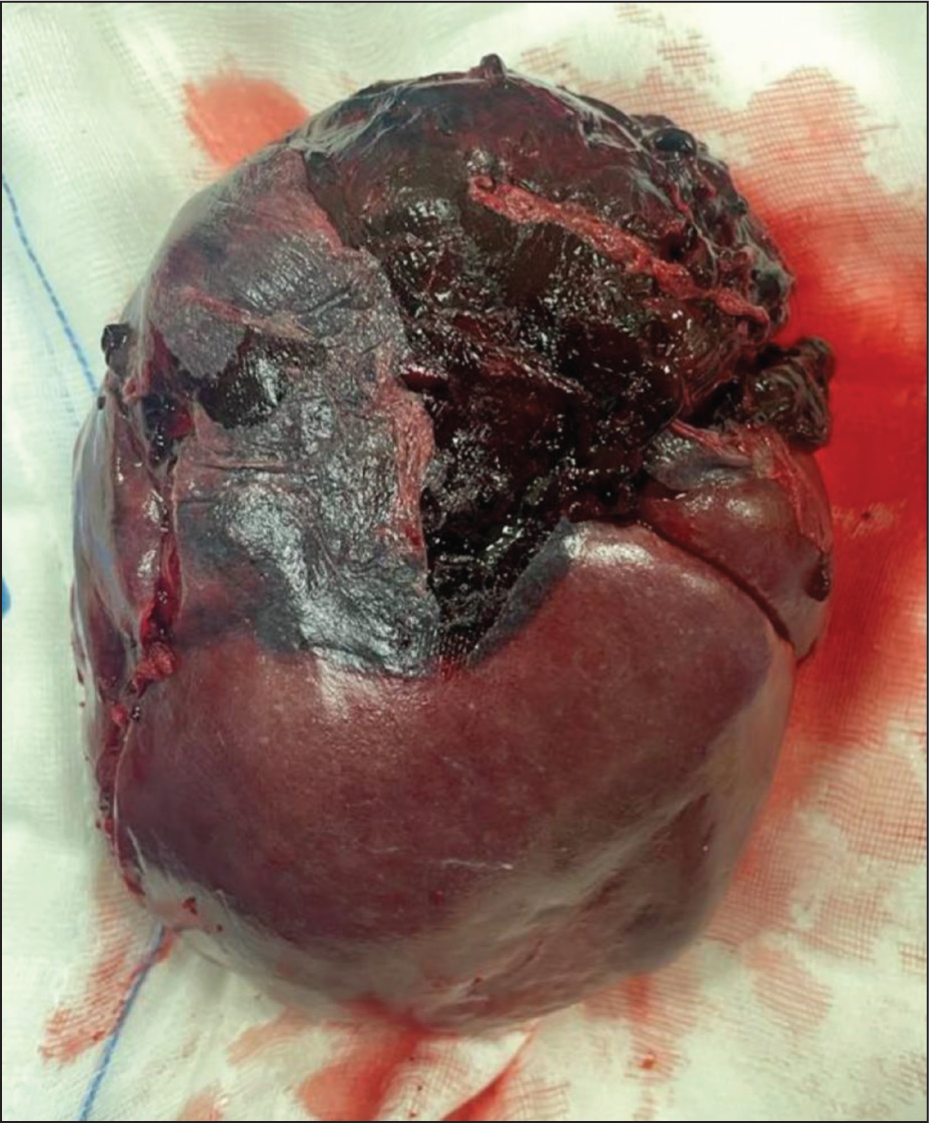
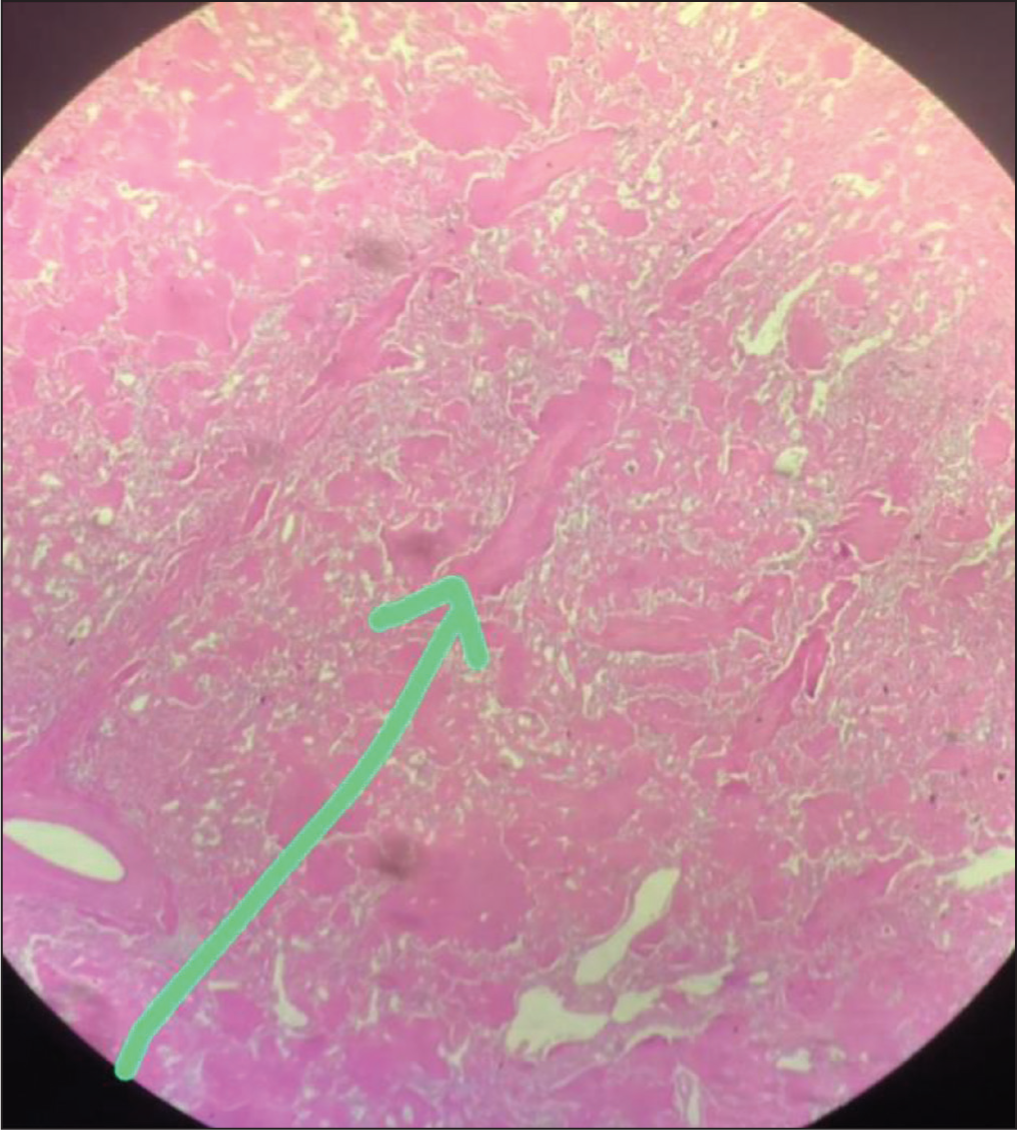
This is a case of a 56-year-old male with AL-type amyloidosis and chronic kidney disease (CKD) undergoing regular haemodialysis. He arrived at our hospital’s Emergency Department (ED) complaining of diffuse abdominal pain, abdominal distension and respiratory distress for two days. The patient provided informed consent. In the ED, he was conscious, with a heart rate of 90 bpm, blood pressure of 82/48 mmHg and Spo2 of 78% on room air. There was no history of blunt trauma to the abdomen or use of antiplatelet or anticoagulant medications. He received oxygen therapy via a face mask, a 500 ml intravenous fluid bolus and a low-dose noradrenaline infusion. After stabilising, he was moved to the intensive care unit (ICU) for further treatment. The routine blood test showed a haemoglobin level of 5 gm/dl, S. creatinine at 5.5 mg/dl and platelets at 1,24,000 cells/mm, with normal liver function. Blood and sputum cultures came back negative. 2D-transthoracic echocardiography revealed mild left ventricular (LV) hypertrophy with normal LV function. Initially, upper gastrointestinal bleeding was suspected, so a stool test for occult blood was conducted, which turned out negative. In the ICU, he started haemodialysis and received two units of PRBC transfusion. An ultrasound of the abdomen showed moderate ascites with internal echoes, splenomegaly, bilateral moderate pleural effusion and anterior abdominal wall oedema. A diagnostic ascitic tap revealed bloody fluid (Figure 1), and about 430 ml of blood was aspirated (Figure 2). Immediately after, a contrast-enhanced CT (CECT) of the abdomen was performed, revealing moderate to gross free fluid in the peritoneum and pelvis, suggesting haemoperitoneum, with a heterogeneous appearance at the splenic upper pole indicative of splenic rupture (Figure 3). The patient was diagnosed with amyloidosis, which raised the possibility of a spontaneous spleen rupture leading to haemoperitoneum. Upon consulting a general surgeon, the patient underwent emergency exploratory laparotomy and splenectomy. The spleen was found to be enlarged with a rupture at the upper pole (see Figure 4). During the procedure, the patient received two units of PRBC and four units of FFP transfusion. The histopathological examination of the spleen tissue using H&E stain revealed extracellular deposition of amyloid proteins (see Figure 5). Additionally, the Congo red stain of the specimen tested positive for amyloid under polarising microscopy. Post surgery, the patient was closely monitored in the ICU, extubated and transferred to the ward on the third day. The patient was discharged on the sixth day with instructions to receive the post-splenectomy vaccine.
Bloody Tap Following Abdominal Fluid Aspiration
The Blood That Was Aspirated (Around 430 ml) Following Abdominal Fluid Aspiration
CECT Abdomen Showing Moderate to Gross Haemoperitoneum with a Heterogeneous Appearance at the Splenic Upper Pole Suggestive of Splenic Rupture
The Spleen (Post-splenectomy) Which Is Enlarged and Ruptured at the Upper Pole
The H&E Staining of Splenectomy Specimen Showing Extracellular Deposition of Amyloid Proteins
Discussion
The spleen typically weighs around 250 g and can measure up to 13 cm long.[4] It is a highly vascularised organ. Around 50%–70% of splenic rupture cases are due to traumatic injury. Other causes of splenic rupture include immunological or haematological issues, such as malignancy. Renzulli et al conducted a systematic literature review to investigate the causes and treatment options for patients with splenic rupture.[5] In this review, 30.3% of patients had neoplasm, 27.3% had infections, 20.0% had inflammatory diseases, 9.2% had drugs/treatment-related SSR, 6.8% had mechanical factors and the remaining 6.4% had no identifiable diseases.
In 1838, a German botanist Matthias Schleiden coined the term ‘Amyloid’ while describing plant starch.[6] Very few case reports were published about amyloidosis-related SSR between the age group of 43 and 87 years.[7] The spontaneous splenic rupture in amyloidosis is due to splenomegaly (accumulation of amyloid fibrils). This makes the spleen fragile and less elastic, increases vascular fragility, and results in the formation of nodules/masses within the spleen, which makes the spleen more prone to rupture. Our patient is also a known case of AL amyloidosis not on treatment.
Ravichandran et al reviewed 11,000 amyloidosis cases and found that 56% of patients had systemic AL amyloidosis. Our patient also had AL-type amyloidosis: 21% had ATTR and 8% had AA amyloidosis.[8] These patients present with signs and symptoms of renal involvement, hepato-splenomegaly, heart failure and carpal tunnel syndrome. Our patient had renal involvement (on maintenance haemodialysis) and splenomegaly due to amyloid deposits. Ultrasound is the initial investigation of choice in suspected cases of splenic injury. It can detect as low as 100 ml free fluid in the abdomen with a sensitivity of 90%.[9] CECT scan of the abdomen is the main diagnostic modality.[10]
Treatment depends mainly on the disease’s severity and the patient’s haemodynamic stability. Angiographic embolisation was found to be effective in 95% of the patients. Surgical treatment is indicated for patients with haemodynamic instability or those requiring more than four units of blood within 48 hours. Our patient underwent surgical treatment due to haemodynamic instability and the need for a blood transfusion.
Conclusion
This case report highlights a rare case of spontaneous splenic rupture secondary to AL Amyloidosis. Having a high degree of suspicion in patients who come to the hospital with pain abdomen and hypovolemic shock (without a history of abdominal trauma or infection) with early diagnosis and treatment can reduce morbidity and mortality.
Footnotes
Acknowledgements
We acknowledge general surgeons Dr Bhaskar Pai, Dr Prasad and Dr Amol), the emergency team (Dr Sharavanan), the pathologist (Dr Deepa), nurses (Aruna, Shruthi and team), respiratory therapists (Inshad and Parvin), physiotherapists (Javed), blood bank manager (Jagadish) and management of the hospital for their valuable support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval
We did not get the Institutional Ethical Committee approval since it was not an observational or interventional study. This is a routine case which every surgeon does in their routine practice.
Informed Consent
Informed consent was taken from the patient.
Credit author statement
All authors equally contributed in completing this case report (the literature search, data acquisition, data analysis, manuscript preparation, manuscript editing and manuscript review).
Data Availability
Available freely on the internet; this is a very rare presentation which we encounter in our clinical practice.
Use of artificial intelligence
Not used.