
Abstract
Background and Aims:
Adenoid cystic carcinoma is a rare and slowly progressing cancer that frequently starts in minor salivary glands, often causing no symptoms. Therefore, advanced stage at initial presentation is frequently reported.
Case Presentation:
We provide a case study of a 33-year-old young woman with pT1 staging adenoid cystic tumour, emphasising the clinical presentation, treatment plan and patient prognosis. Comprehensive examination and imaging tests showed that the patient had a growing mass at the base of her mobile tongue. The diagnosis was supported by histopathological examination. Based on the tumour’s small size and minimal invasion, pT1 was assigned as its staging. A comprehensive treatment strategy was used, and during surgery, the tumour was removed with precise margins that preserved both function and appearance. One-year follow-up showed no evidence of recurrence or ongoing problems.
Conclusion:
This case report emphasises the significance of early diagnosis, thorough treatment planning and attentive follow-up. It also highlights the infrequent presentation of disease.
Background
Adenoid cystic carcinoma (ACC) is a rare epithelial tumour that accounts for approximately 1% of all malignant tumours in the oral and maxillofacial regions. ACC exhibits moderate growth but is highly invasive, leading to an increased risk of recurrence and distant or local metastasis. Hematogenous spread is more common than lymphatic dissemination to nearby lymph nodes.[1] Histopathologically, ACC almost always exhibits perineural invasion and is classified as having a solid, tubular or cribriform pattern.[1] While ACC can occur in various locations, its occurrence in the mobile tongue is documented in only around 2.9% of cases.[1] ACC located near the base of the tongue is challenging to detect early due to its often asymptomatic or painless submucosal presentation. Due to this reason, Goepfert et al reported that 75% of patients with ACC in the base of the tongue almost always presented with advanced-stage tumours categorised as T3 or T4.[1] The management of ACC in the base of the tongue is particularly difficult due to the high risk of local recurrence and distant metastasis associated with locally advanced tumours. However, long-term survival is still possible.[1] The recurrence of tumours can be significantly decreased with radiotherapy, which is advised in advance T3 or T4 disease, while surgical resection with adequate safe margins is an option in T1 disease presentation.[1] The incidence of ACC is higher in women in their fifth and sixth decades of life; however, in younger adults, ACC is seen frequently in major salivary glands of males.[1] We report a case of T1 ACC at the base of mobile tongue in a young female.
Case Presentation
A 33-year-old female patient, with no known co-morbidities and family history, presented at the Otorhinolaryngology Department of a tertiary care hospital, with a complaint of left-sided mass at the base of tongue, growing progressively for three months. No history of addiction was reported. On intra-oral examination, a reddish, firm to hard exophytic growth, measuring approximately 1 × 2 cm was palpated over the base of tongue, more towards the left side, extending to the tonsillar fossa and displacing the uvula to the other side (Figure 1). No neck nodes were palpable. CT scan of the head and neck showed a heterogeneously enhancing lesion on the posterior part of tongue on the left side, measuring about 2 × 2 × 1.5 cm, indenting the uvula with loss of fat planes, extending up to the lateral wall of the oropharynx with focal thickening of the tonsillar fossa. Few subcentimetre lymph nodes were identified at cervical Level II. On the basis of examination and CT scan findings, incisional biopsy was done, which showed basaloid cell morphology with no convincing stromal component, suggesting it to be either adenoid cystic carcinoma, pleomorphic adenoma, epithelial myoepithelial carcinoma or basaloid squamous cell carcinoma. Subsequently, the patient underwent a left hemiglossectomy with ipsilateral neck dissection (cervical lymph node Levels I, II, and III were removed). Intra-operatively, the lesion was resected with clear margins and the edges were then approximated via Vicryl sutures (Figure 2). The resected specimen was sent for histopathology, which revealed adenoid cystic carcinoma with 60%-5% cribriform component, 35%-40% tubular and no solid component. Anterior, posterior, medial and lateral margins were 0.2, 0.2, 1.1 and 0.7 cm away, respectively. Perineural invasion was positive, and none of the resected lymph nodes showed involvement, therefore it was regarded as a pT1 staged tumor. The patient was kept on follow-up, and after one year, there were no active issues or signs of recurrence.
Pre-operative intra-oral reddish, firm to hard exophytic growth, measuring approximately 1×2 cm over the base of the tongue, more towards the left side, extending to the tonsillar fossa and displacing the uvula to the other side
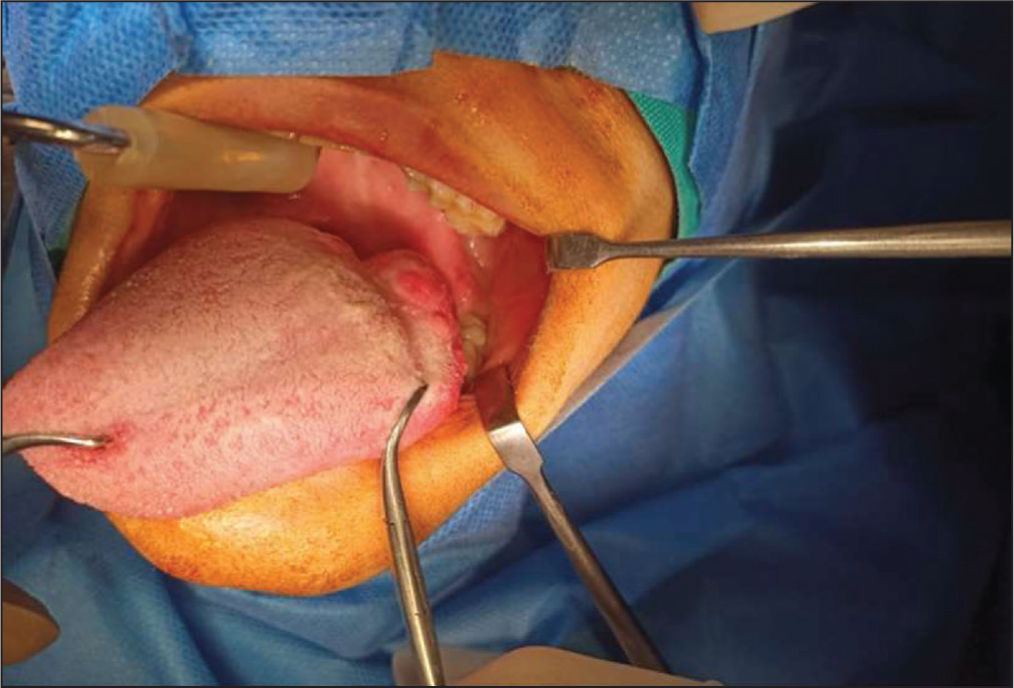
Intra-operative picture after removal of the mass; the lesion was resected with clear margins and the edges were then approximated via Vicryl sutures, with the remaining anterior aspect of the tongue retracted laterally

Discussion
The malignant nature of ACC was explained by Dockerty and Mayo in 1943. Although ACC makes up only around 10% of all salivary neoplasms and less than 1% of all head and neck cancers, it is one of the most prevalent cancers of the submandibular and minor salivary glands. Microscopically, ACC cells are organised in the previously mentioned cribriform, tubular, and solid growth patterns. Generally, cribriform pattern is the most prevalent and comprises basaloid cells of variable size, corresponding to 60% in our case. A well-differentiated tubular pattern is believed to have the best prognosis compared to the moderately differentiated cribriform pattern and worst prognosis in poorly differentiated solid patterns.[1] In terms of gross pathology, ACC has been defined as a firm, un-encapsulated grey-white mass with necrosis and haemorrhage as signs of high-grade transformation.[1] Patients with ACC commonly experience dysphagia as the most initial symptom. Pain has also been observed in 36% of the patients, concluding that it is not so frequent. Other presenting complaints include otalgia and odynophagia. Rarely, a palpable mass is also observed in some cases.[1] This was consistent with our case as dysphagia and palpable mass at the base of the tongue was observed.
The most common occurrence site of ACC is parotid gland, while intra-orally, in 50% cases, the hard palatal region is the most affected. The base of the tongue, as in this case, is a rather unusual site of occurrence with prevalence of less than 2.9%.[1] The incidence of ACC is higher in women in their fifth and sixth decades of life. However, in younger adults, ACC is seen frequently in major salivary glands of males.[1] This was counteracted in our case where ACC was reported in the minor lingual salivary gland of a young female.
Management of ACC depends upon the tumour’s location, stage of diagnosis and biologic behaviour, as seen by histologic grade. When there is an incomplete or near-resection margin, a high-grade or large tumour, signifying advanced T3 and/or T4 stage ACC, adjuvant radiation should be considered.[1] However, according to NCCN guidelines, radical surgical excision with free margins is the ‘gold standard’ treatment for early-stage ACCs.[1] Although being mostly asymptomatic at the base of tongue, T1 ACC rarely presents. Female sex, older age, sino-nasal location, lymph-node invasion, high-grade transformation with perineural invasion, high staging and positive margin status are all poor prognosticators. Primary surgical resection with elective neck dissection in patients of ACC, with or without nodal metastasis, was reported to have more five-year survival rate by Amit et al.[1] Considering the likelihood of recurrence and distant metastases, long-term follow-up is necessary.[1]
Conclusion
ACC is a rare malignant tumour of salivary glands, occurring mostly intra-orally in the hard palate in the fifth or sixth decade of life with female predilection. If presented at a young age, it is prevalent in the major salivary gland of males, almost always at advance stages. This case report presents a case of a young female, who had ACC at the base of her mobile tongue, presented early in the T1 stage, signifying the rare presentation of the disease.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
The study was conducted after receiving institutional ethical committee exemption as a case report as per the Department of Otolaryngology at Dr Ziauddin Hospital, Karachi, Pakistan.
Informed consent
Written consent form was duly signed by the participant of this case report.
Credit author statement
SA: Drafting the article, revising it critically for important intellectual content and reading and approving the final manuscript.
YA: Acquisition of data, drafting the article and reading and approving the final manuscript.
AMK: Acquisition of data, drafting the article, literature search and reading and approving the final manuscript.
WRM: Literature search and reading and approving the final manuscript.
MI: Final approval of the version to be published and reading and approving the final manuscript.
Data availability
The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Use of artificial intelligence
No use of AI.