
Abstract
Background and Aims:
Vaughan–Jackson syndrome, a complication of rheumatoid arthritis, presents with extensor tendon rupture, dorsal tenosynovitis, distal radioulnar synovitis, dorsal subluxation of the distal ulna, and wrist arthritis. This article aimed to present a surgical approach for Vaughan–Jackson syndrome, focusing on dorsal tenosynovectomy, distal ulnar resection and extensor tendon reconstruction.
Case Description:
A detailed case study is presented, highlighting the surgical technique employed for managing Vaughan–Jackson syndrome. Technical nuances and considerations are discussed.
Results:
The surgical technique described resulted in successful management of the patient’s Vaughan–Jackson syndrome, with restoration of hand and wrist function.
Conclusion:
Surgical intervention involving dorsal tenosynovectomy, distal ulnar resection, and extensor tendon reconstruction is a viable option for managing Vaughan–Jackson syndrome. This article provides insights into the surgical management of this complex condition, offering guidance for clinicians encountering similar cases.
Introduction
Rheumatoid arthritis affecting the wrist and hand manifests in various ways depending on the disease stage and progression. In the early stages, patients may present with tenosynovitis accompanied by wrist swelling. As the disease progresses, synovial invasion leads to rapid articular, bony, and ligamentous disruption, causing distortion of the normal wrist anatomy. Clinical symptoms include pain, instability, sudden weakness, or loss of flexion/extension of the fingers, along with restricted range of motion.[1,1] Vaughan–Jackson[1] first described a condition in 1948 wherein the extensor tendon of the ulnar digits progressively ruptures towards the ulnar side due to attrition, compounded by synovitis in the distal radioulnar joint (DRUJ) and radiocarpal region. This results in dorsal subluxation of the distal ulna, accompanied by dorsal bone spicules and roughening.[1-1]
The need to discuss surgical techniques for Vaughan–Jackson syndrome arises from its rarity and poorly understood nature.[1-1] This syndrome, characterised by extensor tendon rupture due to DRUJ attrition, severely impacts functionality, particularly in the dominant hand. Timely diagnosis is crucial to prevent further tendon damage and decay, highlighting the importance of understanding and recognising this condition. Surgical intervention is the definitive treatment for Vaughan–Jackson syndrome, involving tendon reconstruction, protection, and stabilisation, alongside ulnar head resection and osteophyte removal. These procedures aim to halt disease progression and restore function, emphasising the necessity of exploring effective surgical techniques.
Given the limited literature on Vaughan–Jackson syndrome, primarily confined to case reports and series, there is a clear need to provide comprehensive insights into surgical approaches and outcomes. By presenting a surgical technique for this syndrome involving the DRUJ, distal ulna, carpal bones and extensor tendons, we can contribute to advancing understanding and optimising treatment strategies for this challenging condition.
This article outlines a surgical technique involving dorsal tenosynovectomy, distal ulna resection, and reconstruction of extensor tendon rupture in patients diagnosed with Vaughan–Jackson syndrome.
Presentations
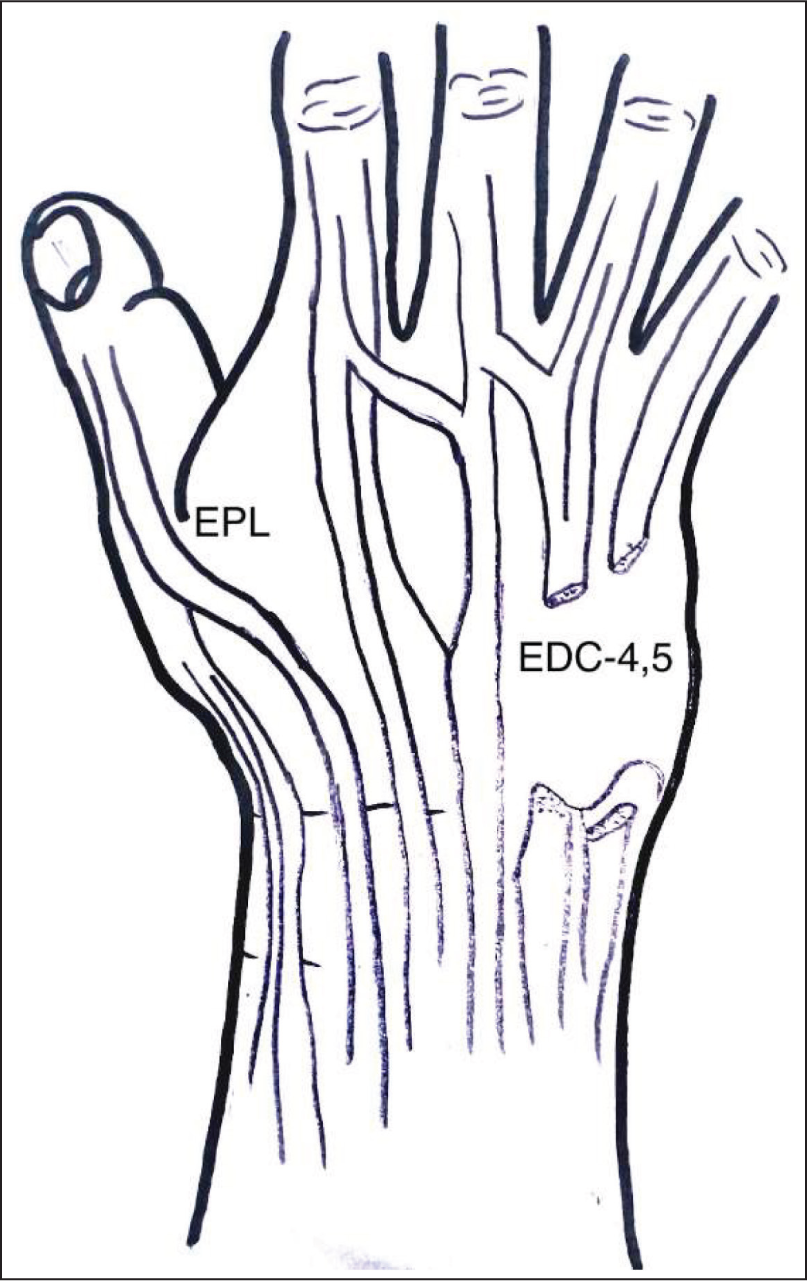
The typical presentation at the emergency room or hand clinic involves a sudden, painless loss of extension in the ulnar fingers (Figure 1). The most commonly ruptured tendons in descending order are the extensor digiti minimi, extensor digitorum communis (EDC) of the little and ring fingers, extensor pollicis longus, and EDC of the middle finger (Figure 2). Radiographs reveal the hallmark ‘scalloping sign’, characterised by erosion of the sigmoid notch with the formation of a sclerotic border.[1,1,1,1] This sign is ominous, indicating rupture or impending ruptures. Additional findings may include dorsal subluxation of the ulnar head, radiocarpal or pancarpal arthritis, carpal fusion, and volar dislocation of the carpus.
Illustration depicting the deformity observed in a patient with Vaughan–Jackson syndrome, showcasing the loss of extension in the ring and little fingers
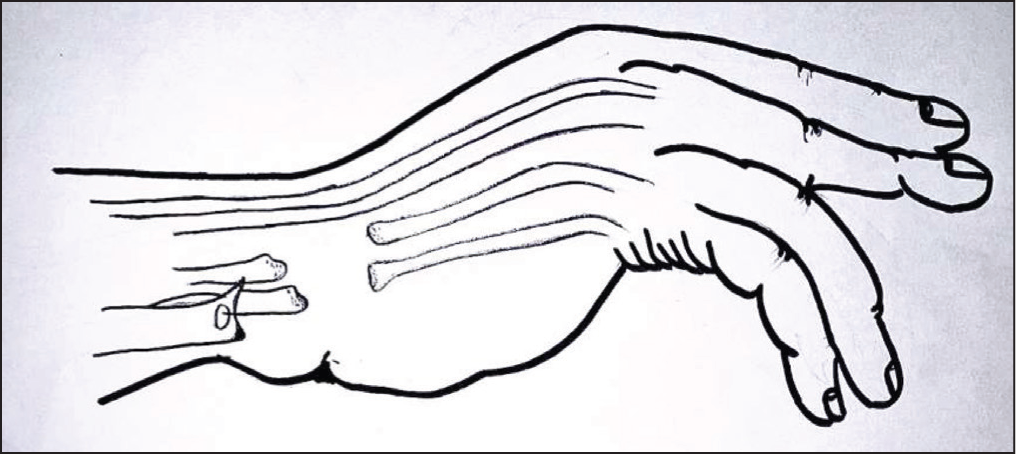
Illustration highlighting the extensor tendon rupture in the ring and little fingers following dorsal prominence of the distal ulna, a rare sequela of rheumatoid disease progression in the wrist
The presence of the Vaughn-Jackson lesion is suggested by radiological scalloping sign and surgical findings such as tenosynovitis of the extensor tendons, tendon attenuation, synovitis of the DRUJ, and ruptures of the ulnar extensor tendons.[1,1]
Indication and Contraindications
Extensor tendon ruptures, coupled with tenosynovitis of the tendons and involvement of the DRUJ, along with radiological evidence indicative of the Vaughn-Jackson lesion, serve as key indicators for extensor tendon reconstruction, involving either transfer or tendon grafting, alongside distal ulnar resection.[1,1,1,1] For patients presenting with multiple risk factors, including clinical and radiological signs, prophylactic tenosynovectomy is recommended. Advanced DRUJ arthritis and radiocarpal dislocation may necessitate Darrach procedures or Sauve–Kapandji procedures with extensor carpi ulnaris (ECU) stabilisation or other tenodesis techniques. In cases where total DRUJ arthroplasty is indicated, restoration of function and attainment of a good range of motion, along with effective pain relief and grip strength, can be achieved.
Relative contraindications to tendon transfer in the hand include perivascular inflammation, boggy synovium, and intrinsic muscle contractures. Additionally, conditions such as skin ulceration or thinning due to vasculitis or prolonged glucocorticoid and immunosuppressive therapy should be carefully considered.[1]
Surgical Anatomy and Pathoanatomy
The dorsum of the distal radius comprises six compartments through which extensor tendons to the wrist and hand traverse, each enveloped by synovium. In rheumatoid arthritis, tenosynovitis ensues, leading to erosions of bone, ligament attenuation between the carpus and DRUJ, and tendon weakening. Consequently, weakened tendons are susceptible to rupture due to friction, resulting in joint instability.[1,1]
Tenosynovitis and hypertrophied synovium can restrict finger mobility due to chronic invasion or bulkiness. Additionally, tendon nodules may impede differential gliding movements. As rheumatoid disease progresses, inflamed synovium infiltrates and erodes the distal ulna and sigmoid region of the radius, leading to extensor tendon rupture.[1,1,1,1]
The DRUJ is particularly vulnerable, frequently manifesting instability in the distal ulna, erosion of the distal ulna, and rupture of ulnar extensor tendons (e.g. EDC of ring and little fingers, extensor digiti minimi, and ECU).[1-1] Subsequently, the damaged triangular fibrocartilage complex (TFCC) destabilises the DRUJ causing dorsal displacement of ulna and volar subluxation of the ECU tendon along with the adjoining carpus bones, a spectrum termed as caput ulnae syndrome.[1,1] This painful deformed DRUJ severely restricts the wrist function and stability. Rupture of the extensor pollicis longus tendon may also occur due to tendon abrasions and avascularity.
Anaesthesia and Patient Positioning
The patient is positioned supine and undergoes surgery under supraclavicular brachial block anaesthesia, with an upper arm tourniquet applied.
Surgical Technique
Informed consent is diligently acquired from all patients, with active involvement of their relatives in the decision-making process.
The surgical technique begins with a curvilinear incision along the dorsal skin, starting over the third metacarpal, gently curving ulnarly over the DRUJ, and extending proximally to the radius.[1] Careful elevation of the skin flaps is followed by dissection up to the extensor retinaculum, with meticulous attention paid to preserving the sensory branches of the radial and ulnar nerves. The extensor retinaculum is fashioned into two ulnar-based flaps, one proximal and one distal. The proximal flap accommodates the site of distal ulna resection, while the distal flap protects the new tendon reconstruction, preventing bowstringing. Longitudinal division of the retinaculum on the radial side of the sixth compartment allows for ulnar reflection.
Surgical exploration reveals a markedly distorted distal ulna protruding through a significant disruption in the ulnar capsule, with intact and ruptured extensor tendons (ring and little fingers) enveloped by hypertrophied pathological proliferative synovium. Thorough tenosynovectomy and excision of diseased tissue are performed using rongeurs or sharp dissection. Evaluation of the ruptured tendon ends reveals attenuation, fraying, infiltration with diseased tissue, and rupture, particularly in the distal ulnar region. Proximal ruptured tendon ends, often retracted into the proximal forearm, are also frayed and thinned out, posing challenges for primary repair with the distal ends.
Rheumatoid synovial tissue invasion may form pea-sized or larger nodules within the tendons, which are excised and repaired with non-absorbable sutures. Tendon transfers or overlay tendon grafts may be necessary when both nodules and tendon rupture ends are significantly attenuated with a large gap. Occasionally, pseudotendon – a thin strand of opaque fibrous tissue – may appear in rheumatoid patients involving the extensor or flexor tendons, requiring excision and treatment as tendon rupture.
Distal Ulna Resection
A substantial functional improvement is obtained by distal ulna resection in Vaughan–Jackson syndrome with painful and deranged DRUJ with extensor tendon ruptures. The ulna head is resected to a level just proximal to the rim of the sigmoid notch of the radius, which is usually <2 cm. Excising too much of the shaft must be avoided because of the risk of causing later instability or worsening instability that may already exist. Therefore, an optimal distal ulna resection eliminates the ulna impingement on the radius and the ulnar carpus. The interosseous membrane and the adjacent tissue may render a maximum stability to the remaining ulna. The cut edge of the ulna is rounded with either a rasp or rongeur to avoid any sharp bone edge beneath the skin or impingement against the adjacent radius. The sigmoid region of the radius is cleared of synovial adhesions and granulations tissues.
The Darrach procedure is recommended for cases involving the resection of the distal ulna in rheumatoid wrists where there is ulnar impingement on the overlying tendons. Additionally, it proves beneficial in addressing intractable pain associated with rheumatoid DRUJ involvement or deformities resulting from subluxation of the DRUJ, with or without extensor tendon ruptures. Furthermore, Darrach procedures are effective in managing pain, instability, and DRUJ post-traumatic arthritis.
ECU Tenodesis
In cases of dorsal subluxation of the distal ulna associated with disruption of the DRUJ, the ECU tendon often subluxates volarly due to fibrous sheath attenuation and stretch. This leads to DRUJ instability and radial deviation of the wrist. To address this, synovectomy of the ECU tendon is performed, and the tendon is relocated dorsally. Although the distal ulna typically remains aligned with the carpus, there is invariably dorsal displacement of the resected distal ulna.
A longitudinal split is made in the ECU tendon, and approximately half of the tendon is divided 6 to 8 cm proximal to its insertion (Figures 3–6). An osseous canal is then created in a dorsal to volar direction through the distal ulna, approximately 1 to 2 cm proximal to the level of resection. The tendon slip is passed into the medullary cavity of the ulna, emerging through a hole in its dorsal cortex. The end of the tendon is then pulled and sutured to the intact distal half of the tendon under maximum traction, with the forearm in pronation and the ulnar hand elevated. This configuration forms a sling, depressing the resected distal ulna and stabilising it.
Illustration demonstrating the technique of half ECU tenodesis to the distal ulna stump, aimed at providing stability and preventing further displacement of the ulna
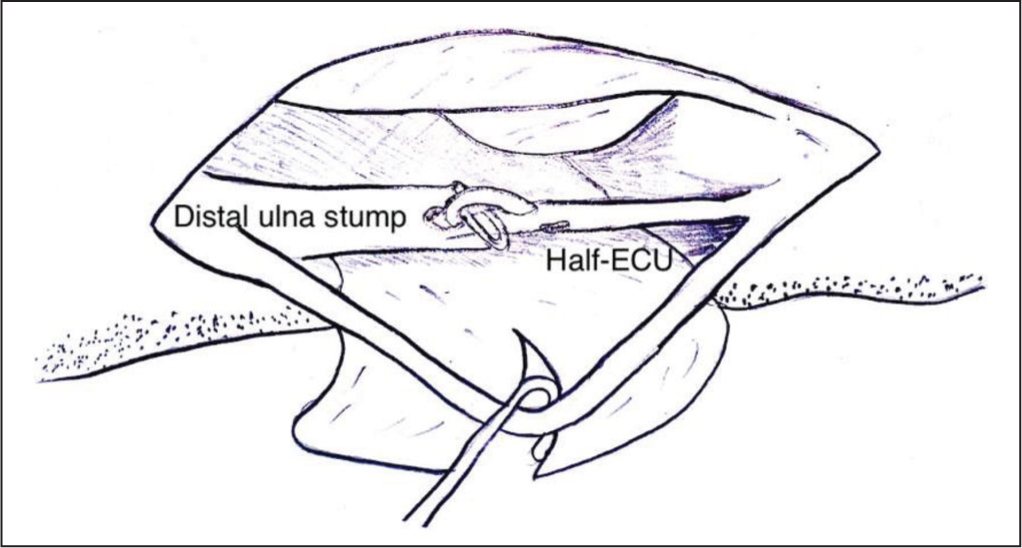
Illustration depicting the reconstruction of the extensor tendon in the ring finger through an end-to-side transfer to the extensor digitorum communis (EDC) of the middle finger, and in the little finger through an extensor indicis proprius (EIP) transfer
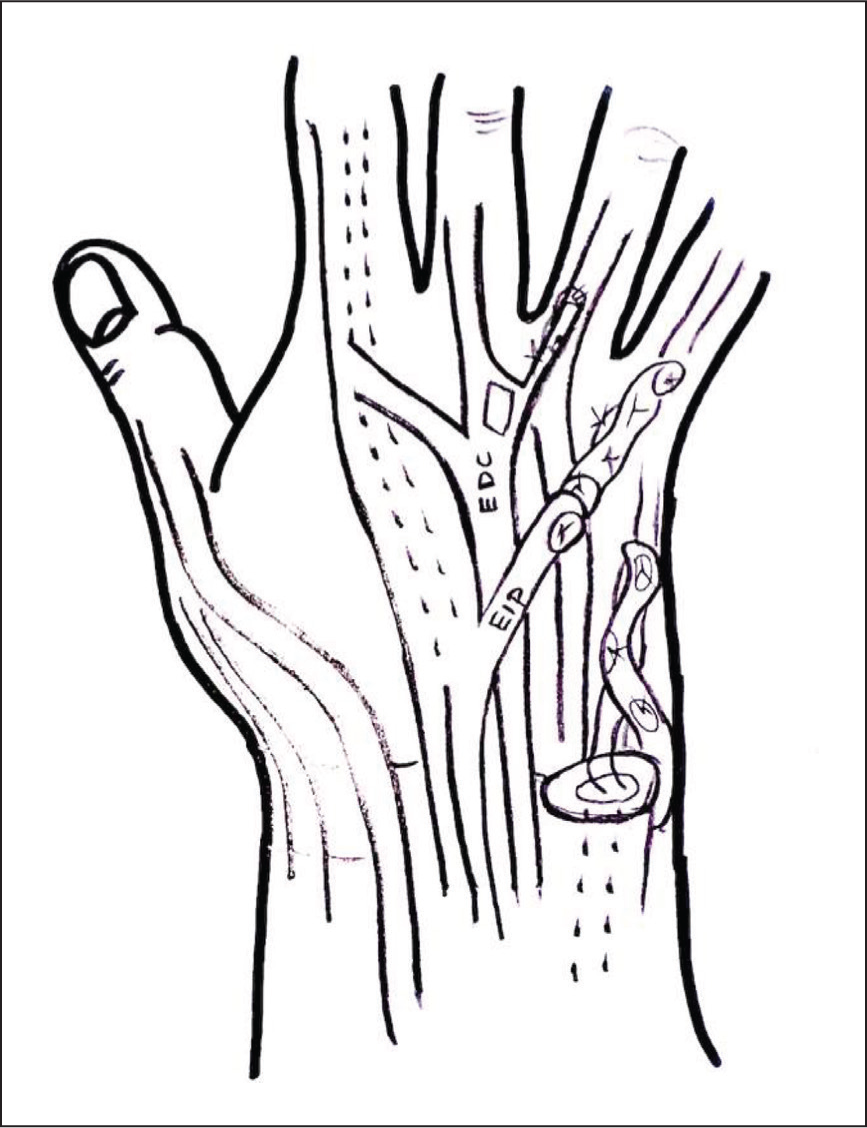
Illustration showing the creation of retinacular flaps and their role in the reconstruction procedure
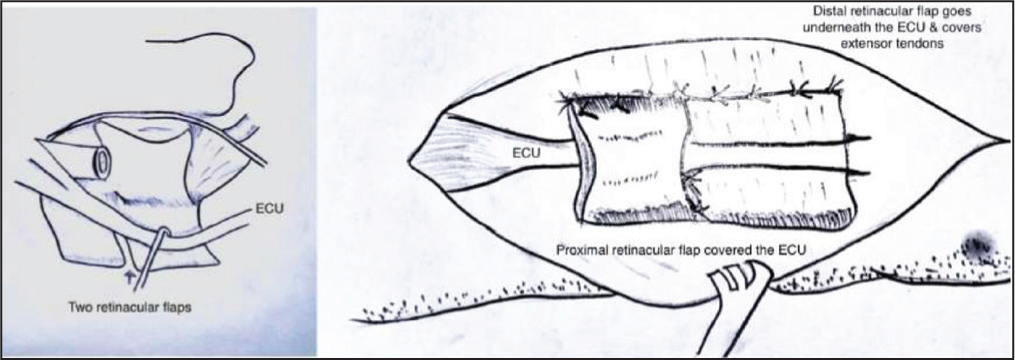
Illustration demonstrating the retinacular flaps covering the extensor carpi ulnaris (ECU) tendon and the extensor tendon reconstruction, preventing dorsal displacement and bowstringing, respectively
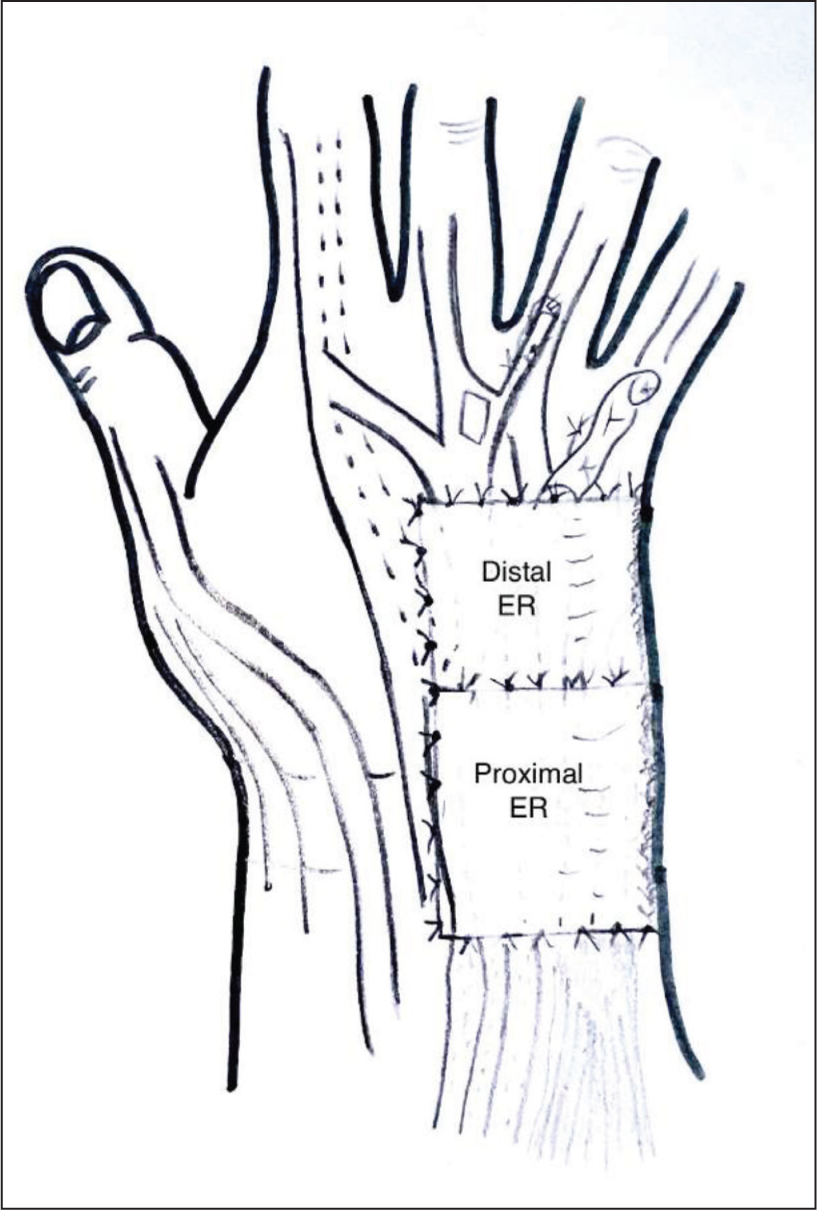
Additionally, the proximal retinaculum flap encircles both the normal and the ECU-tenodesed resected distal ulna, providing further stability. The ECU is restored to its normal position by the downward pressure exerted by the retinaculum flap. Moreover, the retinacular flap serves as a protective membrane between the tendon and the bone, reducing bone rubbing and further stabilising the distal ulna.
The choice between a proximal or distal-based slip of the ECU tendon for tenodesis is determined by intraoperative findings, specifically the degree of tendon attenuation caused by synovial invasion and destruction. Biomechanically, the ECU is the preferred tendon for tenodesis due to its line of pull being closer to the axis of rotation of the ulna. However, in cases where the ECU is severely compromised by disease progression and chronic tenosynovitis, the flexor carpi ulnaris (FCU) may serve as an alternative option for stabilising the distal ulna.
Extensor Tendon Transfer
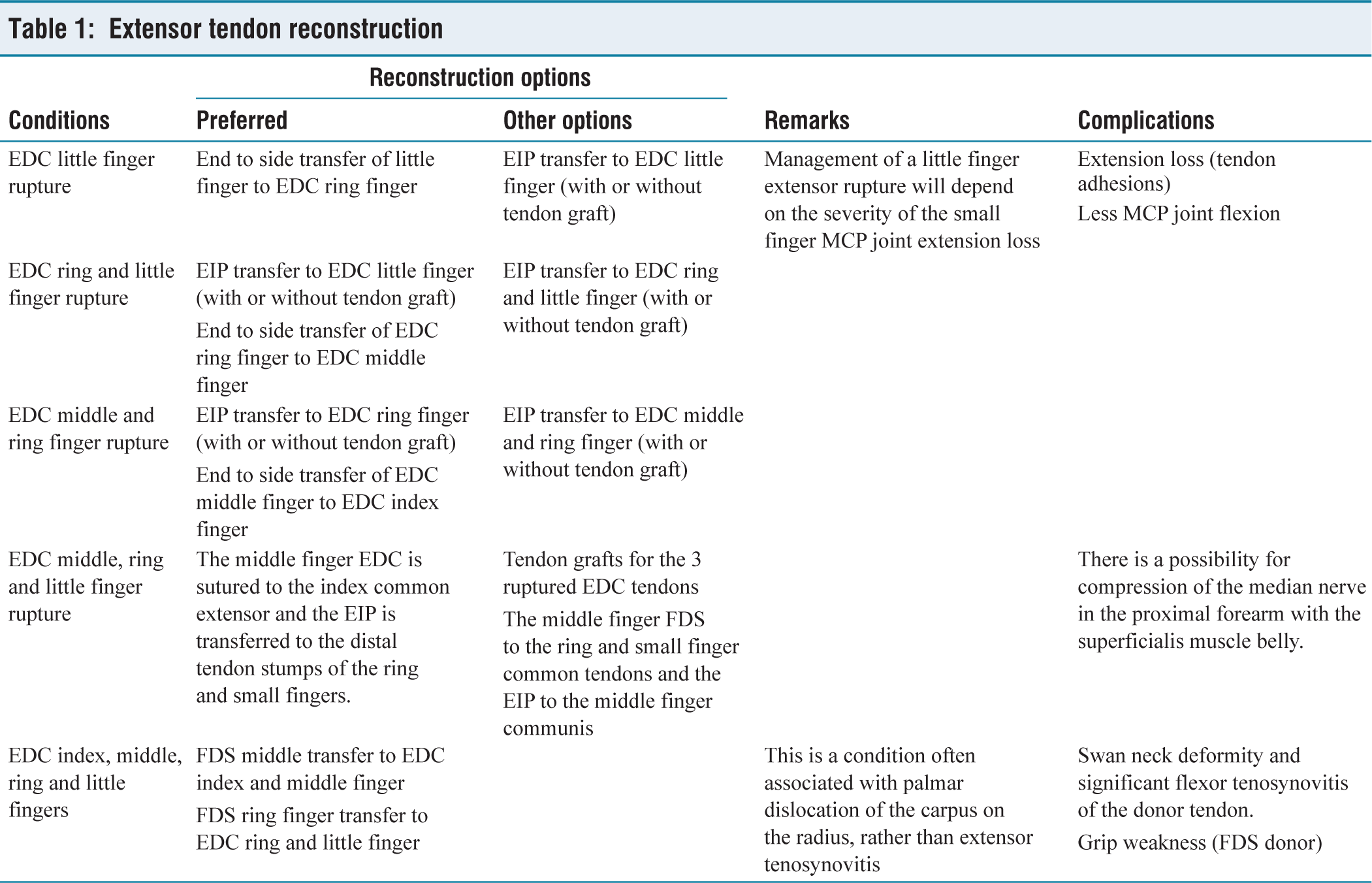
Direct repair of the extensor tendon is seldom feasible due to extensive tendon damage and a significant gap between the resected tendon ends and healthy tissue. Consequently, surgeons typically opt for tendon transfers, which can involve either end-to-end or end-to-side techniques. Potential donor tendons for transfers to the EDC rupture ends include the extensor indicis proprius tendon and the flexor digitorum superficialis (FDS) of the ring finger (see Table 1). Some surgeons may also employ intercalary tendon grafting using the palmaris longus. Tension adjustment is critical during tendon transfer to ensure optimal functionality. For instance, with the wrist in 40° of extension, the metacarpophalangeal (MCP) joints should be capable of 15° flexion, whereas with the wrist in full extension, complete MCP flexion should be achievable.
Extensor tendon reconstruction
Additionally, among other tendon ruptures, the extensor digiti minimi is commonly affected, with frayed, thinned, and retracted ends that may not be amenable to repair.
Postoperative Care
The patient undergoes immobilisation with a wrist splint for a period of 4 weeks post-surgery. Following splint removal, a regimen of passive and active assisted therapy targeting the fingers and wrist extensors is initiated. Night splints are prescribed for an additional 2 weeks. By the sixth week post-surgery, patients are granted full movement freedom and no longer require splinting. Assessment of outcomes utilises a straightforward scoring system modified and adapted from the authors’ Radial Nerve Palsy Tendon Transfer Outcome Score[1] (see Table 2). Additionally, DASH score is also used to assess the overall functional outcome.
Outcome score
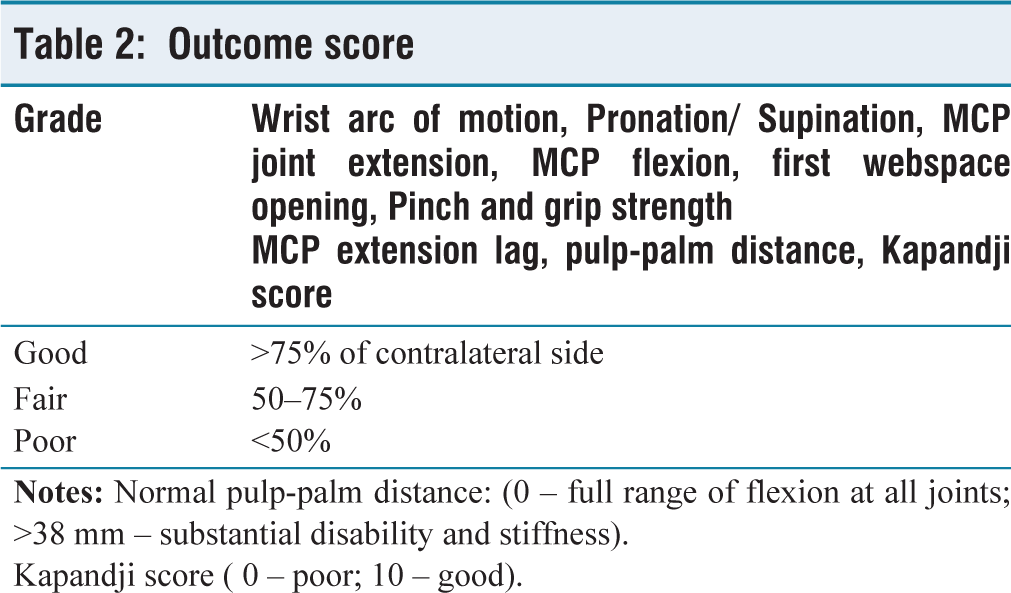
Kapandji score ( 0 – poor; 10 – good).
Illustrative Case
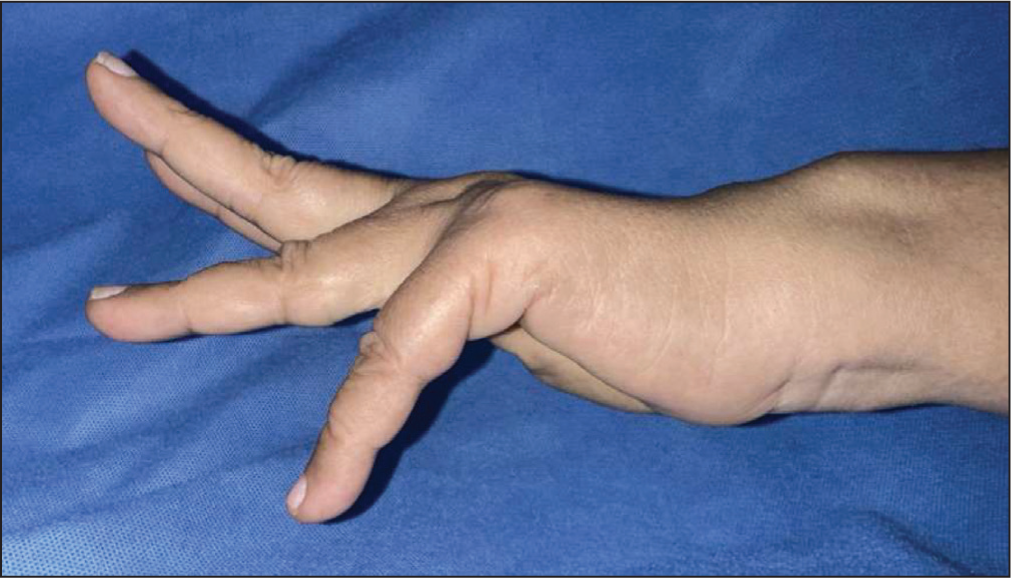
A 62-year-old woman presented to the hand clinic with long-standing pain in her right wrist and a 6-week history of weakness and deformity in her right ring and little fingers. She recalled hearing a popping sound 6 weeks prior, followed by a sudden loss of finger extension in the affected digits. Previously, she had been on disease-modifying drugs for rheumatoid arthritis for 15 years but had recently discontinued them. Upon physical examination, there was no active extension of the ring and little fingers at the MCP joint (Figure 7). However, passive extension was intact. The presence of dorsal prominence of the distal ulna and tenderness over it was noted. Radiographs (Figure 8) revealed distal radioulnar erosion (scalloping sign), a sharp ulnar head, DRUJ arthritis, and partial carpal fusion. A diagnosis of Vaughan–Jackson syndrome was established. Blood parameters were within normal limits. Considering the clinical and radiological findings indicative of tendon rupture, DRUJ arthritis, dorsal prominence of the ulna, and pancarpal arthritis, surgical intervention necessitated exploration of the dorsum of the wrist. This involved identifying the retracted and irreparable tendons beyond primary repair. Subsequently, the distal ulna was resected and stabilised using the ECU tendon. Furthermore, the extensor indicis proprius (EIP) was transferred to the EDC of the little finger, and end-side suturing of the ring finger EDC was performed using the EDC of the middle finger as reinforcement.
Clinical image displaying the loss of extension in the left ring and little fingers in a patient with Vaughan–Jackson syndrome
Radiographs revealing distal radioulnar erosion (scalloping sign), a sharp ulnar head, distal radioulnar joint (DRUJ) arthritis, and partial carpal fusion

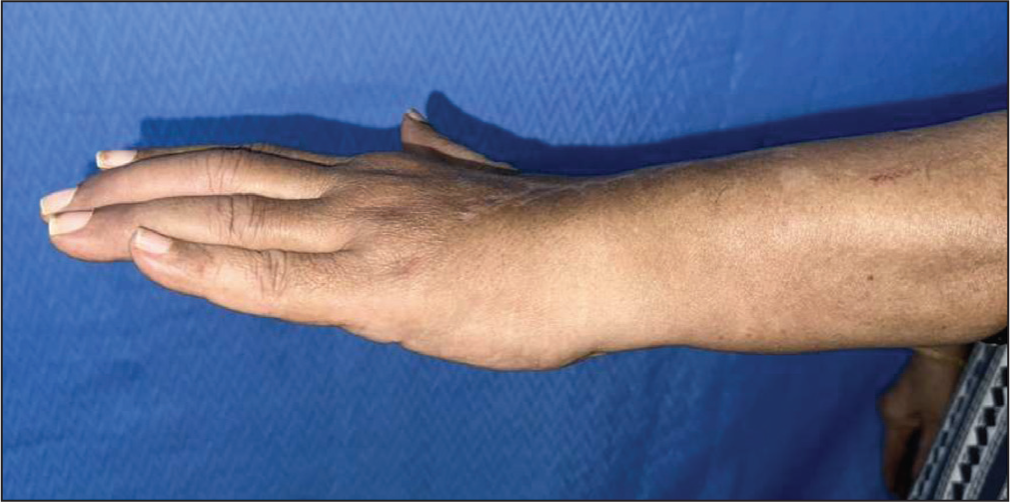
Post-surgery, the patient attained a GOOD grade based on the modified Jerome’s outcome score for extensor tendon transfers/repair (Table 2) in both the wrist and fingers. Additionally, at the 12-month follow-up, the patient reported a DASH score of 4.5 (Figure 9). Regaining full range of motion at the wrist and MCP joints allowed the patient to comfortably resume her daily activities.
Follow-up images of the same patient exhibiting good extension of the fingers
Pearls and Pitfalls
Precise identification and suturing of healthy tendons, along with proficient tendon transfer using the Pulvertaft technique, are crucial for facilitating early postoperative motion. Following reconstruction, it is essential to passively mobilise the finger joints to assess tension across the sutures and transfers. It is imperative to maintain synergy between the wrist and fingers, ensuring that the fingers extend during wrist flexion and adequately flex during wrist extension. Excessive tension may lead to postoperative stiffness and loss of flexion.
Complications
While the author has not encountered complications with this technique, it is essential to acknowledge the potential risks. Reported complications include tendon ruptures, tendon adhesions, insufficient distal ulna resection, failure to stabilise the distal ulnar stump, recurrent tenosynovitis, stiffness, and the development of complex regional pain syndrome (CRPS).
Discussion
Vaughan–Jackson syndrome manifests as a rare combination of symptoms, characterised by dorsal tenosynovitis, distal radioulnar arthritis, erosions, and dorsal prominence of the ulnar head. This condition often culminates in atraumatic, painless rupture of the extensor tendons to the ring and little fingers. Initial tendon rupture typically affects the extensor digiti minimi (EDM), which may go unnoticed due to minimal functional impairment. However, subsequent multiple tendon ruptures result in significant functional loss.
Differential diagnosis includes MCP joint dislocation, extensor tendon subluxation at the metacarpal head level, and paralysis of the extensor muscles due to posterior interosseous nerve compression at the elbow, caused by elbow synovitis. A thorough physical examination is crucial for excluding these conditions prior to surgery.
The selection of the optimal procedure for reconstructing extensor tendon rupture is contingent upon several factors, including the specific digit(s) affected and the number of tendons involved. Options typically include end-to-end repair, tendon grafting, adjacent tendon suturing, or tendon transfer.[1-1] While end-to-end repair is seldom feasible, an intercalated tendon graft may be considered in rare cases where there is a suitable bed (which is uncommon in rheumatoid arthritis) and a proximal motor with adequate excursion (typically observed in recent ruptures). However, in most scenarios, adjacent tendon suturing and/or tendon transfer techniques are preferred (Table 1). The extensor retinaculum flap provides a smooth gliding surface and protects from bone attrition and bowstringing.
The Darrach procedure, involving distal ulna resection, typically achieves favourable outcomes in terms of pain relief, range of motion, and grip strength. However, post-procedural radio-ulnar impingement is a recognised complication. To address this impingement, various stabilisation techniques are employed, such as ECU or FCU tenodesis or pronator quadratus tenodesis. Alternative methods involve utilising retinacular flaps or palmar capsular flaps to prevent dorsal displacement of the ulna.
In our author’s modifications, additional measures are taken, including radial half of the proximal ECU tenodesis, distal extensor retinaculum flap to protect against bowstringing, and proximal extensor retinaculum flap to prevent dorsal displacement of the ulna, along with ECU tenodesis to mitigate distal end ulna impingement. ECU tenodesis reinforces stability to the distal ulna, radiocarpal joint, and acts as a buttress and checkrein for disease progress around the DRUJ.
While the Sauve-Kapandji (SK) procedure is typically indicated for painful and unstable DRUJ with sufficient bone stock in the ulna head for arthrodesis with the radius, it may not be suitable for cases of Vaughan–Jackson syndrome due to distal ulna erosion, DRUJ subluxation with arthritis, and extensor tendon ruptures resulting from ulnar impingement.
Overall, the Darrach procedure is often favoured in elderly and low-demand patients, where tendon reconstruction, coupled with ECU tenodesis, serves to prevent further impingement and dorsal displacement, as seen in our case series.
The study’s focus on Vaughan–Jackson syndrome, a rare condition, limits the applicability of its findings to broader populations or different types of extensor tendon injuries. Its potentially small sample sie, due to the syndrome’s rarity, could impact the reliability of conclusions. Being conducted at a single centre may limit diversity in patient demographics and treatment approaches, affecting external validity. As a retrospective study, bias in patient selection and outcome assessment could influence results without proper randomisation or blinding. Long-term follow-up data on post-surgery outcomes may be lacking, essential for evaluating intervention efficacy. While describing surgical technique modifications, the study may lack direct comparisons with alternative treatments, hindering assessment of superiority. Surgical outcomes may vary based on surgeon experience, potentially leading to inconsistency, especially if multiple surgeons are involved. Despite mentioning procedure complications, the article may lack thorough discussion on frequency, severity, and management, critical for clinical decision-making.
Despite these limitations, the author documents that surgical techniques effectively manage Vaughan–Jackson syndrome, resulting in significant clinical improvement and restoration of daily activities. Surgical intervention is crucial for addressing tendon rupture, DRUJ arthritis, and ulnar prominence. Techniques such as distal ulna resection, stabilisation using the ECU tendon, tendon transfers, and end-side tendon suturing contribute to finger extension restoration. Further studies and long-term follow-up are necessary to validate these findings and refine treatment strategies for this complex condition.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval from the Ethical Committed Board of OHRC. No 08/2024
Informed consent
The patients and/or their families were informed that data from the research would be submitted for publication, and they consented.
Credit author statement
J TJJ: Roles/writing – original draft, data curation, and conceptualisation. CM: Writing – drawing, review & editing.
Data availability
The data are available with the due consent of the patients.
Use of artificial intelligence
Nil.