
Abstract
Background and Aims:
Lipomas are termed as universal tumours. They can potentially arise from any site having adipose tissue. Presence of lipomas in the intra-peritoneal region is rare, with mesentery being one of the rare locations.
Methods:
We present a rare case of a two-year-old child with a giant mesenteric lipoma. This child presented with malnutrition and was being treated for Koch’s abdomen.
Results:
The child underwent uneventful resection of mass.
Conclusion:
Giant mesenteric lipomas due to their size can present with various unusual symptoms. However, these seldom infiltrate and are easily operable with an uneventful intra-operative course and follow-ups.
Introduction
Lipomas in their ubiquitous notoriety can also be found intraperitoneally.[1] Omentum and bowel mesentery are two intraperitoneal structures harbouring fat and are thus possible sites for a lipoma. The soft yielding consistency of fat allows them to go unnoticed while they slowly grow to a large size.[2] Herewith, we report a rare case of a giant mesenteric lipoma in a malnourished two-year-old boy which was being treated as abdominal tuberculosis (Koch’s abdomen).
Case Report
A two-year-old male child weighing 8 kg presented to us with complaints from six months of protuberant abdomen, intermittent peri-umbilical pain, early satiety and failure to thrive. Clinically, he had a diffusely distended abdomen, which on palpation had a soft doughy consistency. The palpation was non-tender, with no definite localised mass felt. The child was being treated as a case of abdominal tuberculosis by a local practitioner, in view of spurious contact history from his maternal grandmother, who was under treatment for pulmonary tuberculosis. Chronic malnutrition also was attributed to tuberculosis. He had a BCG scar on his left deltoid region and was immunised for age. An abdominal X-ray revealed a ground glass appearance along with normal bowel gas pattern. An ultrasonography showed a large diffuse heterogenous mass involving the entire omentum occupying the entire abdomen. Features were rendered as suggestive of a giant omental lipoma.
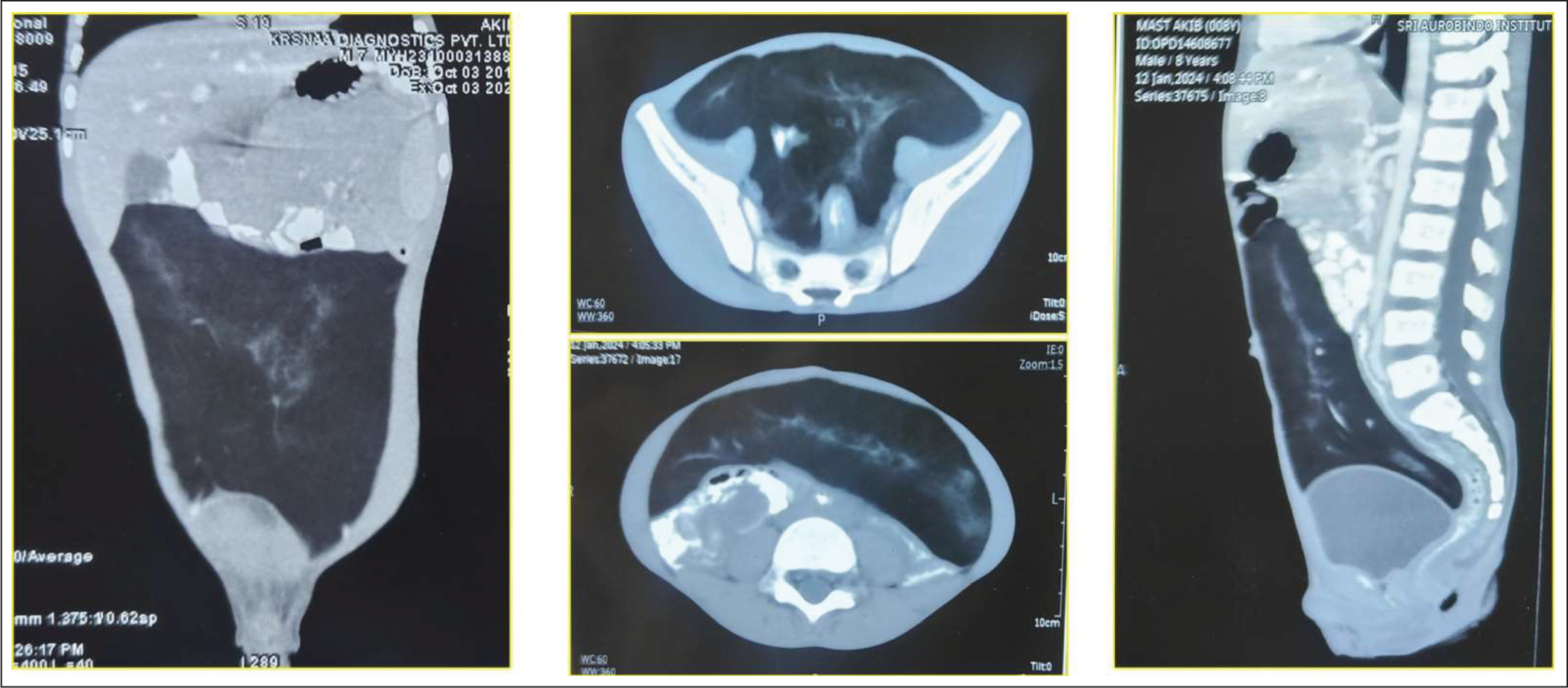
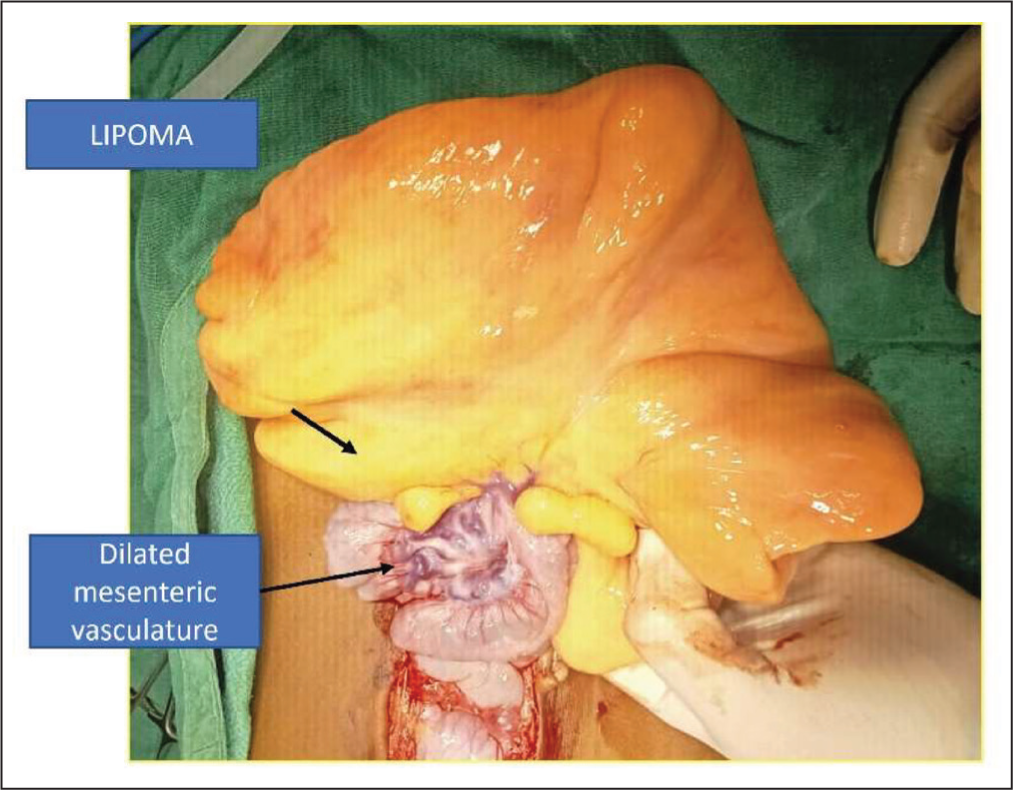
A computed tomography scan showed heterogeneously hypodense fat density (100 HU mean) with a size of 14 cm × 12 cm × 5 cm sized extending from the subhepatic/sub-splenic region to the pelvic cavity, with non-enhancing linear soft tissue and mesenteric vessels within the lesion (Figure 1). These features were suggestive of a giant mesenteric lipoma. Because of suggestion of retroperitoneal extension and large size of the mass, an upper midline incision was planned. Laparotomy revealed a large lipomatous mass with size 15 cm × 6 cm × 10 cm. The mass was in close relation to 5 cm of ileal segment occupying its mesentery, which was divided with the mass. The surrounding mesenteric vessels were dilated and tortuous (Figure 2). An ileo-ileal anastomosis was done. The patient had an uneventful post-operative stay and was discharged after five days. Anti-tubercular medications were stopped, and he was advised a high-protein diet. On two-weeks follow-up, the patient was asymptomatic and playful with improved appetite and improved quality of life. Histopathology revealed it to be a lipomatous mass.
Computerised Tomography Scan Images Showing Giant Lipoma
Intra Operative Figure Showing Giant Lipoma with Mesenteric Vessels and Involved Intestine
Discussion
Mesenteric lipomatous tumours are slow-growing, mobile, soft masses that are not known to infiltrate the surrounding organs.[3] Most symptoms are due to their large size. As a giant lipoma is usually diffuse and soft, many go unnoticed on clinical examination.[4] The lipoma is not felt as a discrete lump. The abdomen in a giant lipoma usually feels distended diffusely and has a doughy feel akin to that described in a tuberculous abdomen. It can impinge on surrounding structures causing obstruction, an ileus-like picture.[4] Large tumours in smaller children can raise suspicion of a rapidly growing cancerous mass. 5 The giant lipoma also can lead to secondary constipation, which is considered as the cause for abdominal distension and early satiety and thus delays the diagnosis.[4]
A common reason for malnutrition in a giant lipoma is pressure symptoms leading to early satiety and constipation.[6] What we observed in our case was the presence of hugely dilated mesenteric vasculature as seen in cases with portal hypertension. Thus, we propose that these huge lipomas would have certain pressure on the mesenteric vasculature and the portal system, and the hypertension thus caused in these vessels can be an added reason for these patients being nutritionally compromised.[7]
The differential diagnoses of a large lipomatous mass include teratoma, lymphangioma, lymphoma, alimentary tract duplications and neuroblastoma.[3] Lipomas are homogeneous, highly echogenic and encapsulated on an ultrasonogram; however, larger masses may look more diffuse. Lipoblastomas, on the other hand, appear as a well-defined hypoechoic myxoid mass embedded within highly echogenic fat.[3] Identification of a lipoma with computerised tomography is done on the basis of a circumscribed low fat density mass ranging from −120 to −65 HU.[1-3]
Despite the conclusive diagnosis of a lipoma by various radiological methods, the large size, presence of fat in various tumours and the multitude of differential diagnosis entertained in a case of a suspected giant lipoma, we recommend a midline incision as an incision of choice in dealing with these giant tumours. Most of the giant lipomas do not infiltrate surrounding structures and can be easily resected. However, many a times they are so closely related to the mesentery that bowel resection becomes imperative, for safe surgery.[1-4] The recurrence rate for any lipoma after local excision is less than 5%. Incomplete excision and lipoblastomas are associated with increased chances of recurrence.[2]
Conclusion
A giant mesenteric lipoma can be consistently diagnosed preoperatively using the conventional radiological methods. However, the surgical approach should be fashioned in a way that other differential diagnoses can be dealt with. These lipomas can reach large sizes in asymptomatic individuals and can be diagnosed erroneously as they present as a diffuse mass with very common symptoms. They seldom infiltrate and are easily operable with an uneventful intra-operative course and follow-ups.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The patient’s informed consent for the publication of the case details and photographs was taken.
CRediT Author Statement
Saurabh Garge: Conceptualisation, title framing, literature search, drafting and critical revision of the article for important intellectual content
Himanshu Kelkar: Literature search, collection, follow-up
Ashutosh Sharma: Final approval of the version to be published
Jayesh Jajodia: Analysis and interpretation of data and manuscript writing
Data Availability
Data Available.
Use of Artificial Intelligence
Not applicable.