
Abstract
Background:
Recurrent episodes of upper airway collapse during sleep cause obstructive sleep apnoea (OSA). Patients with OSA, a serious clinical condition, frequently halt or reduce their breathing while they are asleep. This results in non-restful, fragmented sleep, which exacerbates symptoms such as morning headaches and drowsiness during the day.
Aims and objectives:
This review article focuses only on the current medical treatment of OSA. It will also catalyse further study and better awareness of the current medical treatment of OSA.
Materials and methods:
A search was conducted for recent research articles on current medical treatment for OSA. We searched the PubMed, Scopus, Medline and Google Scholar online databases.
Results:
Heart arrhythmias, depression, hypertension and coronary artery disease are among the medical disorders linked to OSA. Clinical symptoms that are predictive include obesity, enlarged neck circumferences, gasping when sleeping and loud snoring. Those who are obese, hypertensive, frequent snorers and hyper-somnolent should be suspected of having OSA. An essential test for accurately diagnosing OSA is overnight polysomnography.
Conclusion:
As OSA is a chronic illness, a long-term, interdisciplinary strategy is required. The first step in managing OSA is patient education. For treatment of OSA, lifestyle changes including losing weight, switching to a different sleeping position, abstaining from alcohol and using certain drugs are crucial. When treating OSA, positive airway pressure is a crucial choice. Since OSA affects both the person and society as a whole, further investigation is needed to find novel treatment approaches for this morbid clinical condition.
Introduction
In society, obstructive sleep apnoea (OSA) is a prevalent condition that is underdiagnosed. Patients often exhibit this sort of sleep-disordered breathing when they have upper airway blockage during sleep.[1] In the case of central sleep apnoea, there is absence of the drive to breathe during sleep, leading to insufficient ventilation and reduced gas exchange in the lungs. On the other hand, individuals with OSA have either whole or partial collapse of the upper airway along with a decrease in oxygen saturation or awakening from slumber.[1] If OSA is not treated, it can result in substantial morbidities affecting several vital organs of the body.[1] OSA also confers a substantial burden on the individual and family due to its morbid clinical manifestations with multiorgan involvement. Currently, surgery of the upper airway, continuous positive airway pressure (CPAP) therapy and specific dental devices made to change the upper airway’s size are the available therapeutic options for OSA.[2] However, all patients with OSA will not tolerate these types of therapy. Other treatments that are commonly used to manage these difficult situations and may even lessen the severity of the diseases include positional therapy, weight loss, oxygen therapy, sleep hygiene, pharmaceutical treatment, pharyngeal muscle stimulation and nasal cavity dilators.[2] This review article addresses the available medical treatments for OSA at present.
Methods of Literature Search
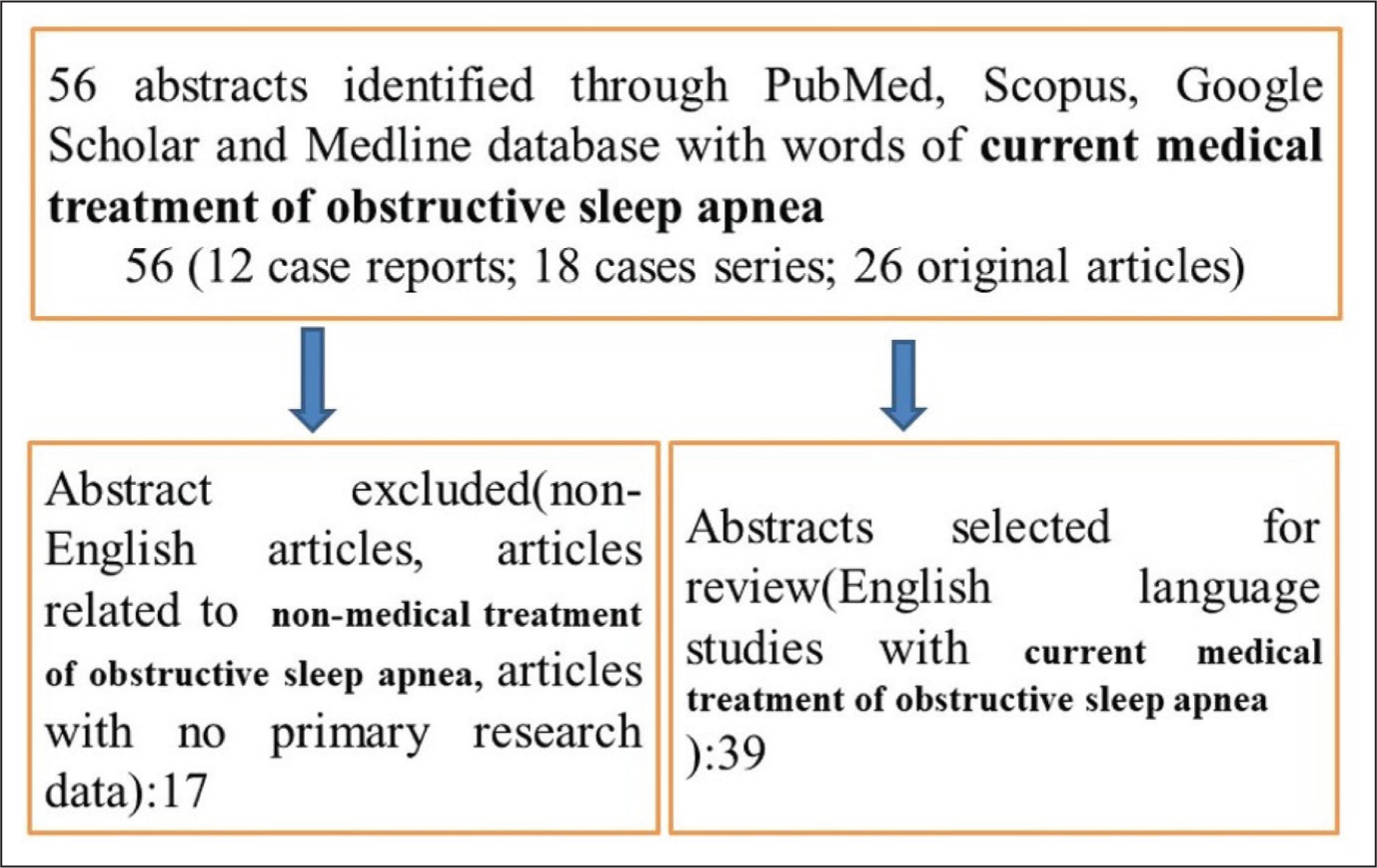
A search was conducted for recent research articles on current medical treatment for OSA. First, we searched the PubMed, Scopus, Medline and Google Scholar online databases. A search strategy was created using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analysis) guidelines. The published works’ abstracts were identified by our search method, although more research publications had to be manually located from the citations. A variety of study designs were looked at, such as case reports, case series, comparative studies, observational studies and randomised controlled trials. There were 12 case reports, 18 case series and 26 unique pieces in all (Figure 1). This review article focuses only on the current medical treatment of OSA. It will also catalyse further study and better awareness of the current medical treatment of OSA.
Methods of Literature Search
Prevalence
The precise prevalence of OSA is uncertain, but it typically varies between 2% and 14% within the community.[3] The prevalence of OSA among persons referred for sleep is 20%–90%.[4] Compared to women, men are three times more likely to develop OSA.[5] It is uncommon in non-obese individuals and premenopausal age. Yet, incidence of OSA in the postmenopausal period in women who are not undergoing hormone therapy is comparable to the rates seen in males of the same age group and with the same body mass index.[6] The occurrence of OSA increases with age, particularly among individuals aged 60 and above. Advancing age and an increasing prevalence of obesity both contribute to a heightened likelihood of OSA.[7]
Clinical Presentations
Snoring and apnoea are common symptoms of OSA during sleep. The clinical manifestations of OSA that are predictive of the condition include loud snoring, enlarged neck circumference (greater than 16 inches/40.6 cm), morning headaches, gasping or choking during sleep and fragmented sleep accompanied by excessive daytime sleepiness.[8] Additionally, the patient may exhibit lethargy, exhaustion or low energy. Cognitive and attention difficulties accompanying the symptoms have an impact on the individual’s quality of life. OSA is more common among males than females, and this clinical condition may be overlooked in females.[9] OSA is a stand-alone risk factor for cardiac rhythm abnormalities, diabetes mellitus, hypertension and stroke. It is typically unappreciated how bed partners affected by clinical signs of OSA experience marital discord, increased risk of work-related injuries and decreased productivity. The impact of OSA on both individuals and society needs a definitive treatment.
Medical Management
In order to reduce the morbidity in the individual and burden on society as a whole, therapeutic treatment options are crucial for people with OSA. Positional therapy, auto-adjusting positive airway pressure (PAP), serotonin, drugs that promote wakefulness, genioglossus stimulation surgery, extra oxygen, nasal dilators, nasal expiratory resistor devices and activities targeting the oropharynx are among the options for treating OSA.[10] CPAP is still the most preferred method of medical management in patients with OSA besides the surgical option. All medical options should be regularly monitored with polysomnography and the sleep score protocols.[10]
Continuous Positive Airway Pressure
CPAP is an important treatment recommended for OSA. It functions by supporting the upper airways with a continuous flow of air, helping to keep them open during sleep. This air pressure can be administered using devices that cover the mouth, nose or both. CPAP is a cost-effective treatment option for patients with OSA along with lifestyle measures. CPAP is the most common type of PAP that is needed for OSA treatment. CPAP assists in keeping the upper airway open by increasing the air pressure, preventing collapse of the airways and maintaining a level above which collapse would occur.[11] Supplemental oxygen via nasal cannula is a temporary measure in OSA patients waiting for surgery. For OSA, nasal CPAP is generally considered the most successful treatment.[12] CPAP not only enhances daytime sleepiness and snoring but also decreases hypertension, car accidents and mortality.[13] CPAP is also an effective treatment option in comparison to other lifestyle management.[14] There are a number of reasons why people do not use CPAP, such as claustrophobia, chronic skin irritation/pain due to mask or simple inconvenience, especially in jobs that require travel to other places and long hours on the road, where carrying a CPAP device is difficult. For many OSA patients, CPAP must be used every day; nonetheless, it is not a cure. Even reports of potential lingering signs of daytime tiredness are present. This could encourage patients and researchers to look for alternative CPAP treatments.
Auto-titrating Continuous Positive Airway Pressure
For individuals at a fixed pressure, conventional CPAP is advised. Age, changes in weight and the use of more recent drugs that relax soft tissues can all cause the pressure to alter over time. Higher CPAP pressure is necessary for patients with primarily rapid eye movement (REM)–related OSA or positional OSA at specific periods of the night, although it may not be necessary for non-rapid eye movement (NREM) or non-supine sleep. The feature of the auto-titrating CPAP device is that it can automatically change the pressure as the patient sleeps from 5 to 20 cm of H2O. So, raising of CPAP pressure is needed when patient goes into supine or REM sleep. This can allow a lower pressure to be maintained during other hours of the night in comparison to traditional fixed-pressure CPAP, potentially increasing compliance and comfort. Using auto-titrating CPAP as part of an empirical treatment plan for suspected high-risk patients for OSA based on Berlin questionnaire is safe and effective.[15] According to a research, CPAP enhanced compliance by 11 minutes and reduced the average Epworth tiredness scale score by 5 points when compared to fixed-pressure CPAP.[16]
Nasal Dilators
Nasal dilators function by widening the passage of the nasal cavity and reducing resistance in the nasal cavity, thereby improving airflow. This mechanism is believed to help prevent collapse of the hypopharynx and reduce both noisy breathing during sleep and OSA. Nasal dilators are of two types: internal nasal dilators, which are inserted into the nostrils and expand the passages due to their elasticity, and external nasal dilators, which are applied outside of the nose and work by gently pulling the nostrils open. There is a scarcity of studies examining the efficacy of nasal dilators specifically for treating OSA. A majority of research indicates that nasal valve dilators are not particularly effective in managing OSA. A prospective study focusing on internal nasal dilators in individuals with moderate to severe OSA found minimal impact on snoring and sleep apnoea episodes.[17] Additionally, feedback from most bed partners indicated only a slight decrease in snoring. Consequently, nasal dilators are generally not advised as a treatment option for OSA.[17]
Sleep Hygiene
Patients with OSA may experience prolonged episodes of apnoea, a decreased hypoxic and hypercapnic respiratory drive, and an increased threshold for arousal as a result of sleep loss. Thus, sleep deprivation may make OSA symptoms worse.[18] Adjusting one’s lifestyle can help cure OSA by enhancing sleep hygiene. A regular sleep and wake-up time as well as abstaining from stimulants like caffeine are among the lifestyle adjustments. Reducing physical activity before bed and mentally slowing down are also helpful for good sleep.[18] Avoiding sedatives and alcohol, which decrease the pharyngeal muscle tone and enhance sleep fragmentation, is also recommended.
Weight Reduction
Cervical obesity, a build-up of fat around the neck airway that is associated with obesity in people, encourages the collapse of the upper airway.[19] The upper airway collapses frequently in patients with OSA. It appears that reducing weight exacerbates this collapsibility by raising the crucial closing pressure of the pharynx.[20] Losing weight can help the upper airway expand and become more open, especially if symptoms start to appear after a large increase in weight. There exists a non-linear relationship between the apnoea-hypopnea index (AHI) and body weight, meaning a substantial decrease in weight is necessary before a notable decrease in AHI can be observed.[21] The extent to which weight loss can ameliorate sleep apnoea varies among individuals. Research has indicated that an approximately 3% decrease in AHI is observed with every 1% decrease in body weight.[22] Substantial weight loss can be attained through very low-calorie diets or surgical interventions, both of which have been shown to improve OSA and even lead to the resolution of apnoea in certain patients. Encouraging weight loss is crucial for obese individuals with OSA, and lifestyle changes and dietary adjustments play vital roles in their management. For severely obese patients, surgical treatment like gastric stapling bypass can be beneficial. In cases where modest weight loss occurs, it may reduce the need for long-term CPAP therapy.
Oral Appliance Treatment
If an individual finds it challenging to use CPAP, oral appliances present a viable alternative. Oral appliance therapies come in two prominent varieties: mandibular advancement devices (MADs), which move the patient’s jaw forward to maintain an open airway, and tongue-retaining devices, which hold the tongue in place to maintain an unobstructed airway.[23] MADs are favoured over tongue-retaining devices due to the scarcity of evidence supporting the latter’s effectiveness. Furthermore, emerging alternatives like oral pressure therapy utilise a mouthpiece and vacuum pump that work together to stabilise the tissue in the upper airways.[24] In patients with moderate to severe OSA, in particular, CPAP is thought to be more beneficial than oral appliances in reducing AHIs, arousal indices and oxygen desaturation. However, the indices of quality of life is believed to be comparable between CPAP and oral appliances.[25] Comparable rates of blood pressure reduction were found in a meta-analysis between MADs and CPAP therapy.[26]
Electric Stimulation of Upper Airway
Occlusion of the upper airway is seen in OSA due to the reduced tone of the neuromuscular pharyngeal wall. The genioglossus muscle, innervated by the hypoglossal nerve, plays a critical role as a pharyngeal dilator. Stimulation of the hypoglossal nerve has been identified as a valuable therapy for OSA. A study investigated the effects of hypoglossal nerve stimulation using an implantable device, specifically the InspireTM I system, over a six-month period. During the study, patients demonstrated a notable decrease in AHI, from an initial range of 48–52 to 17–23 after one month of hypoglossal nerve stimulation during sleep.[27] Stimulating the posterior section of the genioglossus muscle tends to provide greater stabilisation of the pharynx compared to stimulating the anterior section. Optimal results are typically observed in patients with large tongues and a narrow pharynx.[28] Further research is needed to fully understand the extended effects of hypoglossal nerve stimulation in the management of OSA. The patient selection criteria and optimisation of implantable stimulating devices for hypoglossal nerve stimulation are needed.[28]
Nasal Expiratory Resistor Devices
This one-way valve creates a strong expiratory resistance during expiration, acting as a splint to maintain the patient’s upper airways. When EPAP was applied via a valve, individuals with OSA experienced fewer and shorter apnoea. The mechanisms behind this action are lung hyperinflation from elevated end-expiratory pressure increasing the tracheal traction, a decrease in upper airway collapsibility and a mild increase in CO2 from hypoventilation, leading to increased respiratory drive. Upper airway dilatation is caused by pressure generated during expiration. When compared to a sham therapy, the nasal EPAP device dramatically lowers the average heart rate and enhances the subjective measure of daytime drowsiness in patients with mild to severe OSA who have exceptional adherence during a three-month time. Individuals with mild to severe OSA intolerance to CPAP have an alternate therapeutic option in the form of the nasal expiratory resistor device.
Lifestyle Changes
Obesity causes fat accumulation around the neck, which manifests the collapse of the pharyngeal wall. Although it has been shown that reducing weight lowers the airway’s essential closing pressure, there have been conflicting results about the connection between weight loss and better breathing and sleeping patterns.[29] For patients with OSA, sleeping in the supine position instead of the lateral position may result in an increase in AHI by up to two times. Tennis balls can be put in a pocket or sock and fastened to the back of shirts, vests with rear bumpers can be worn and positional alarms can be used to deter supine sleeping. However, positional treatment is not widely used because of low long-term compliance. Good sleep hygiene includes a set bedtime and wake-up time as well as avoiding certain stimulants like caffeine. Sound sleep is also aided by reducing physical activity before bed and mentally unwinding. It is crucial to avoid alcohol and sedatives that weaken the muscles in the airway and cause sleep fragmentation in order to practice proper sleep hygiene.
Pharmacotherapy
Patients of OSA should steer clear of few medications known to either exacerbate or improve obstructive events. Specifically, benzodiazepines, narcotic agents and muscle relaxants should be avoided by individuals with OSA as these might reduce the upper airway activity and cause breathing difficulty. Certain pharmacotherapies have been tried for the treatment of OSA.
Protriptyline
Protriptyline is classified as a tricyclic antidepressant with the ability to bolster upper airway tone through its impact on central norepinephrine transmission. It has been used in smaller trials as well as for the treatment of OSA.[30]
Baclofen
Baclofen, functioning as a gamma-aminobutyric acid (GABA) agonist and muscle relaxant, can influence mean overnight oxygen saturation if administered prior to sleep.[31]
Benzodiazepines
Various benzodiazepines, such as nitrazepam, flurazepam, temazepam and triazolam, have been examined in individuals with OSA. A study observed that oral flurazepam at a dose of 30 mg was linked to an increase in the frequency and duration of apnoea episodes, as well as a worsening of oxygen desaturation levels.[32] Another study showed a significant increase in the number of non-REM apnoea after taking a single dose of flurazepam (45 mg).[33] Taking triazolam at a dose of 0.25 mg one hour before bedtime raises the threshold for arousal from airway occlusion during sleep. This can result in a slight prolongation of apnoea duration and increased oxygen desaturation.[34]
Morphine
Morphine, an opioid analgesic, has the potential to suppress the ventilatory drive, leading to respiratory depression. The only opioid with a regular dosage that does not appreciably worsen sleep-disordered breathing in a healthy, normal person who does not appear to have OSA symptoms is oral hydromorphine.[35]
Intranasal Steroids
Certain individuals suffering with rhinitis and OSA may find relief from intranasal steroids, such as fluticasone. A six-week course of intranasal budesonide treatment was shown in research to decrease the degree of underlying adenoid hypertrophy and the severity of moderate OSA.[36] Topical steroids are a good starting point for treatment for mild OSA in otherwise healthy children.
Acetazolamide
Acetazolamide is an inhibitor of carbonic anhydrase that raises salt and bicarbonate excretion through the urine, which causes metabolic acidosis and increases respiratory drive. By enhancing the central ventilatory drive and stabilising the ventilatory control, it is helpful in moderate instances of OSA.[37] In one study, acetazolamide medication significantly improved sleep structure and clinical symptoms while reducing the frequency of apnoea, apnoea index and the percentage of apnoea duration in male patients with OSA.[38]
Almitrine
Almitrine is a respiratory system stimulant that acts by making the carotid body’s peripheral chemoreceptors more sensitive. This method increases hypoxic pulmonary vasoconstriction, which improves gas exchange. In a particular research, it was found to elevate the average oxygen saturation levels during sleep while reducing the frequency of desaturation events.[39]
Armodafinil
The Federal Drug Administration has approved armodafinil as a longer-acting R-enantiomer of modafinil for the treatment of OSA in those who comply with CPAP therapy but still have excessive daytime drowsiness.[40] Although the precise mode of action is unknown, it is believed to be connected to the neurotransmitter system that promotes orexin wakefulness. It improves episodic memory and lengthens the sleep latency. A few adverse effects include rash, headache, nausea, hypertension and mental symptoms such as mania, anxiety, sadness and psychosis.
Thyroid Hormone
Higher OSA prevalence is linked to hypothyroidism. When hypothyroidism is present in people with OSA, thyroid hormone replacement therapy is thought to be a therapeutic option for those with sleep disorders. Although hypothyroidism is associated with nocturnal apnoea, there is no correlation between the incidence of nocturnal apnoea and thyroid hormone levels.[41] Following standard thyroid hormone treatment, there is a substantial correlation between the blood level of thyroid hormone and the values of maximum and mean apnoea as well as the greatest oxygen saturation in individuals with OSA and primary hypothyroidism.[42]
Conclusion
OSA is a common clinical entity and its prevalence is increasing in modern days. Early treatment of OSA helps reduce morbidity such as cardiovascular and cerebrovascular events. While CPAP, oral devices and surgery are recognised treatments for OSA, numerous novel and unconventional therapies are also available. The first treatment of OSA includes weight reduction and behavioural therapy like changing position while sleeping. Drinking alcohol or taking medications that worsen apnoea should be avoided. CPAP therapy stands out as the primary and most crucial treatment for OSA.
Footnotes
Acknowledgements
The author is thankful to Ishan Satvik for language corrections of the manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
Not applicable.
CRediT Author Statement
SKS: Conception, design, data analysis, data interpretation, drafting and final approval of the manuscript.
Data Availability
Data openly available in a public repository that issues datasets with DOIs.
Use of Artificial Intelligence
Not used.