
Abstract
Introduction:
The term ‘hepatitis’ describes an inflammation of the liver. A viral infection commonly causes it, but there are other possible causes of hepatitis. These include hepatitis caused by drugs, alcohol, toxins and other pharmaceuticals, as well as hepatitis caused by autoimmune conditions. The World Health Organisation suggested that by the close of the 20th century, all nations should include the Hepatitis B vaccine (HBV) in their regular infant and childhood immunisation regimens.
Objective:
To evaluate the knowledge, attitude and practice of Hepatitis B vaccination among students attending medical, dental, nursing and physiotherapy courses.
Materials and Methods:
Students studying medicine, dentistry, nursing and physiotherapy at a tertiary health care facility in Kerala’s Kozhikode district are participating in this cross-sectional survey. A structured, open-ended questionnaire that the self-administered knowledge, attitude and practice (KAP) used to gather information regarding HBV infection and vaccination was employed to assess the KAP. For the assessment of knowledge, attitude and practice, appropriate scoring was carried out. Utilising SPSS Software version 20.0, the data was analysed.
Results:
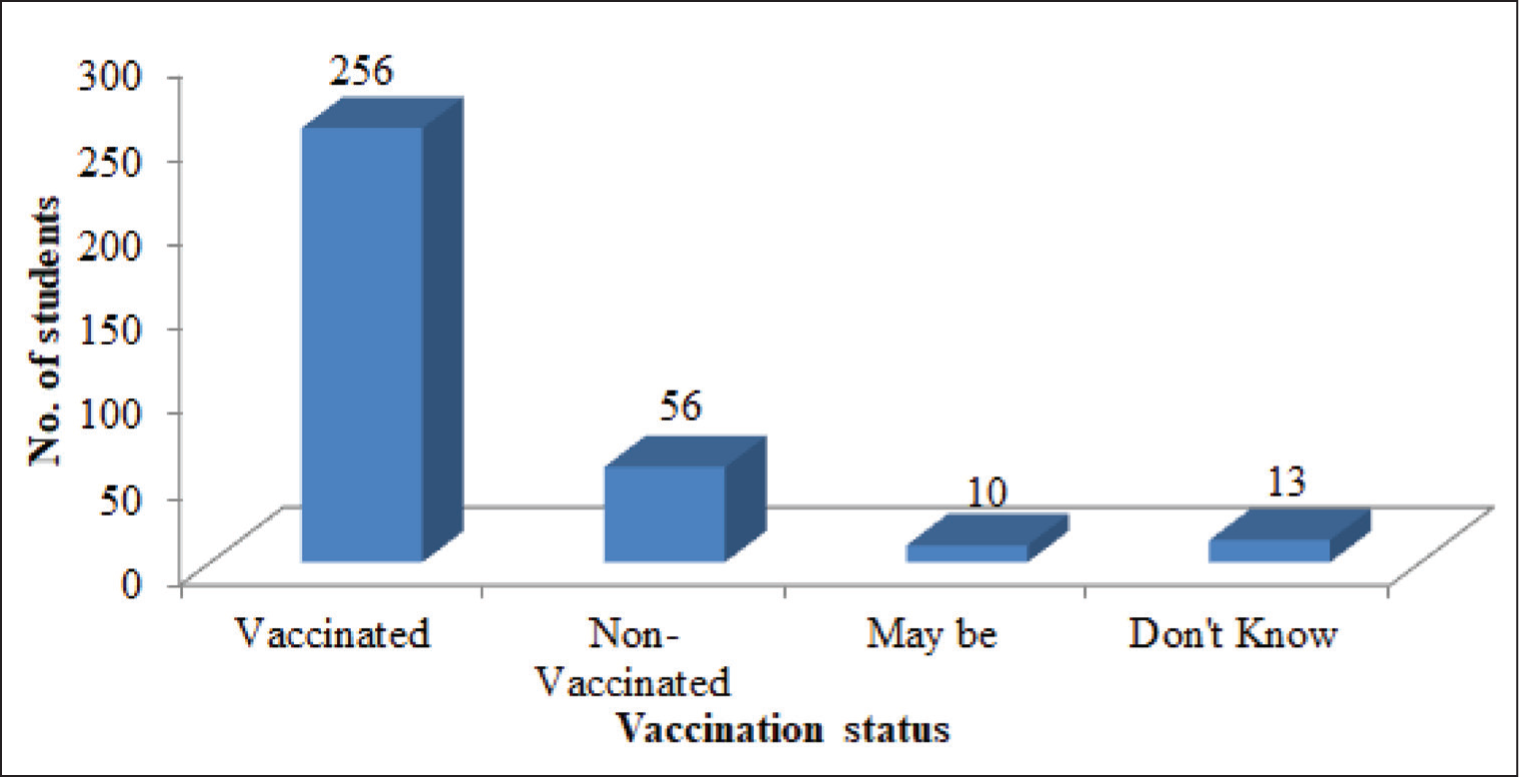
Out of the total 335 students who responded, 256 (76.4%) students were vaccinated, 232 (69.3%) showed poor knowledge towards Hepatitis B vaccination, 6 (16.7%) were not vaccinated and the remaining 23 (6.9%) are not sure about vaccination status. About 38.8% of students have good practice and show a significant association between knowledge, attitude and practice of Hepatitis B vaccination among students.
Conclusion:
This study shows an association between knowledge, attitude and practice of Hepatitis B vaccination among students, implying that a better understanding of the disease has a positive effect on the practices exercised by an individual.
Keywords
Introduction
Hepatitis refers to an inflammatory condition of the liver. A viral infection commonly causes it, but there are other possible causes of hepatitis.[1] These include hepatitis caused by drugs, alcohol, toxins and other pharmaceuticals, as well as hepatitis caused by autoimmune conditions. Numerous viruses can cause viral hepatitis. The hepatitis types A, B, C, D and E are the five types. While hepatitis A and E viruses are mainly found on faeces, hepatitis B, C and D viruses are mainly found in blood or bodily fluids made from blood.[2]
The hepatitis B virus (HBV) is the cause of hepatitis B, a liver infection that can be prevented by vaccination. Hepatitis B can spread to non-infected individuals by contact with contaminated blood, semen or other body fluids. This can happen during intercourse, when sharing syringes, needles, or other injectable supplies, or when a mother transmits it to her infant child. While signs of a new HBV infection are not always evident, those that do may include jaundice, exhaustion, nausea, decreased appetite and stomach discomfort. For many people, hepatitis B is often a temporary illness. Others can get a persistent, chronic infection that can lead to life-threatening conditions including liver cancer or cirrhosis. Age at diagnosis is associated with an increased risk of chronic illness––approximately 90% of newborns with hepatitis B go on to acquire chronic infection, compared to 2%–6% of adults who contract the virus as adults. To prevent hepatitis B, vaccination is the recommended course of action.[3] Knowledge is the ability to gather, organise and apply information; attitude is the propensity to respond in a certain manner to particular circumstances; and practice is the use of guidelines and knowledge to take appropriate action. Good practice is an art form that is ethically performed and connected to the advancement of knowledge and technology.[4] To control the disease, it is crucial to evaluate their knowledge, attitude and practice as well as their status as vaccinated. This study aimed to evaluate the knowledge, attitude and practice of Hepatitis B vaccination among medical, dental, nursing and physiotherapy students in a tertiary health care centre.
Methodology
Students studying medicine, dentistry, nursing and physical therapy who agreed to take part in the survey and provide their knowledge, attitude and practice (KAP) on the hepatitis B vaccination were the subjects of this cross-sectional study. The KAP assessments were scored appropriately. Information regarding HBV infection and vaccination was gathered for the evaluation of the KAP using a standardised, open-ended questionnaire that was self-administered. Thirty-six students participated in a pilot study after the questionnaire’s validity was established. It posed queries regarding knowledge of hepatitis vaccination, diagnosis and transmission. A scoring system was used to establish if the participants’ knowledge was good, average or bad. With the use of relevant questions and a valid scoring system, the attitudes of the participants were assessed. Information regarding practices related to exposure to and/or protection against the HBV was obtained through appropriate queries. Thirty-six students participated in a pilot study after the questionnaire’s validity was established. The SPSS software version 20.0 was used to examine the data once it was extracted into Microsoft Excel.
Results
Out of the 335 students who responded, 68% accounted for females and 32% for males [Figure 1]. A total of 46.6% of the students belong to medical, 38.2% dental, 26.78% nursing and 7.5% physiotherapy students [Figure 2]. A total of 58.8% of the students belonged to rural areas, and 41.2% belonged to urban areas. Results showed that out of the respondents, 76.4% of students were vaccinated. The remaining 23.6% of the students were unsure about their vaccination status [Figure 3]. A total of 40.29% were aware of Hepatitis B vaccination through awareness programs, 41.9% through lectures, 8.95% through social media and the remaining were from another source.
Distribution of study participants according to their gender
Distribution of study participants according to their course
Distribution of study participants according to their vaccination status
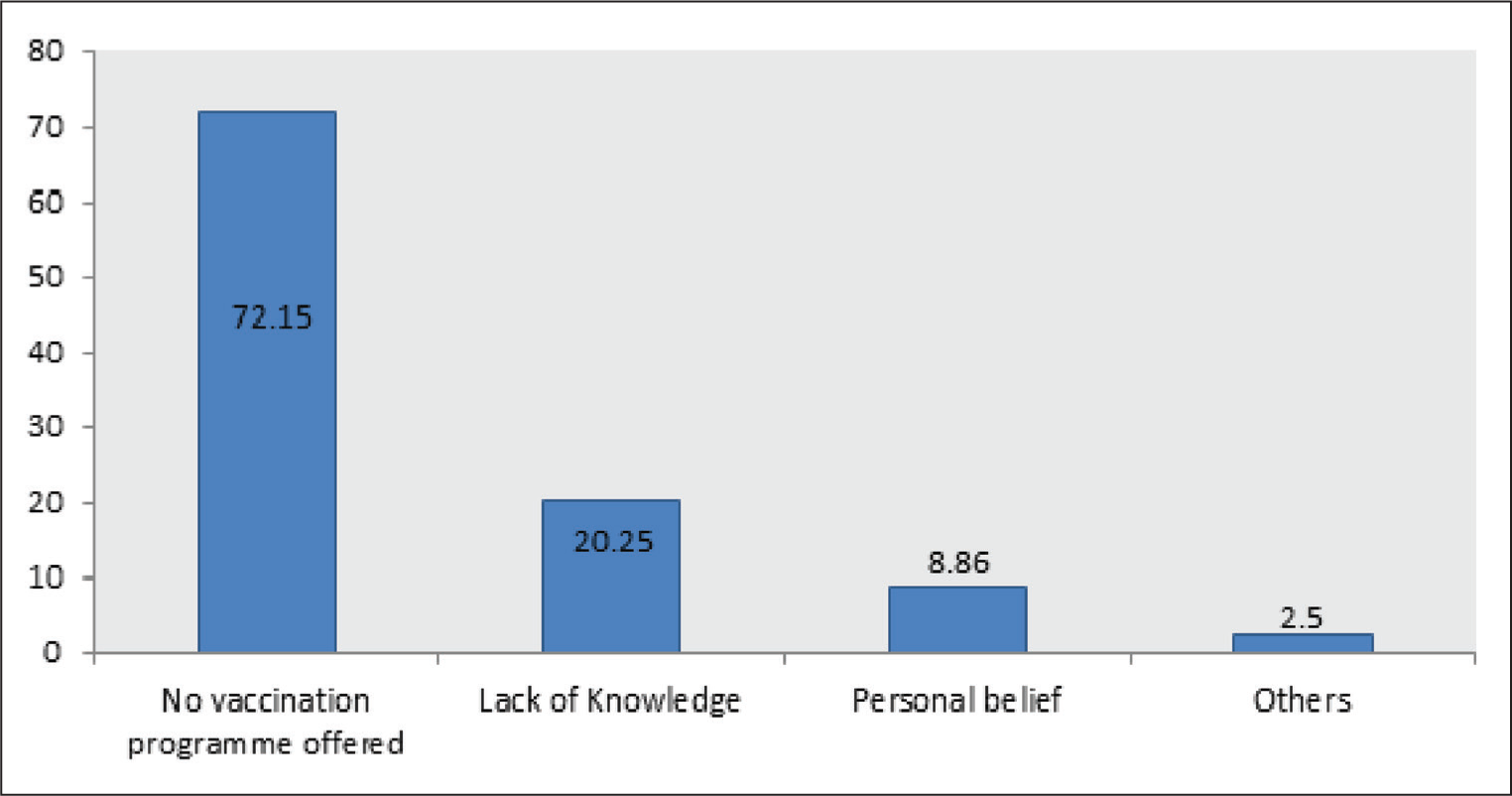
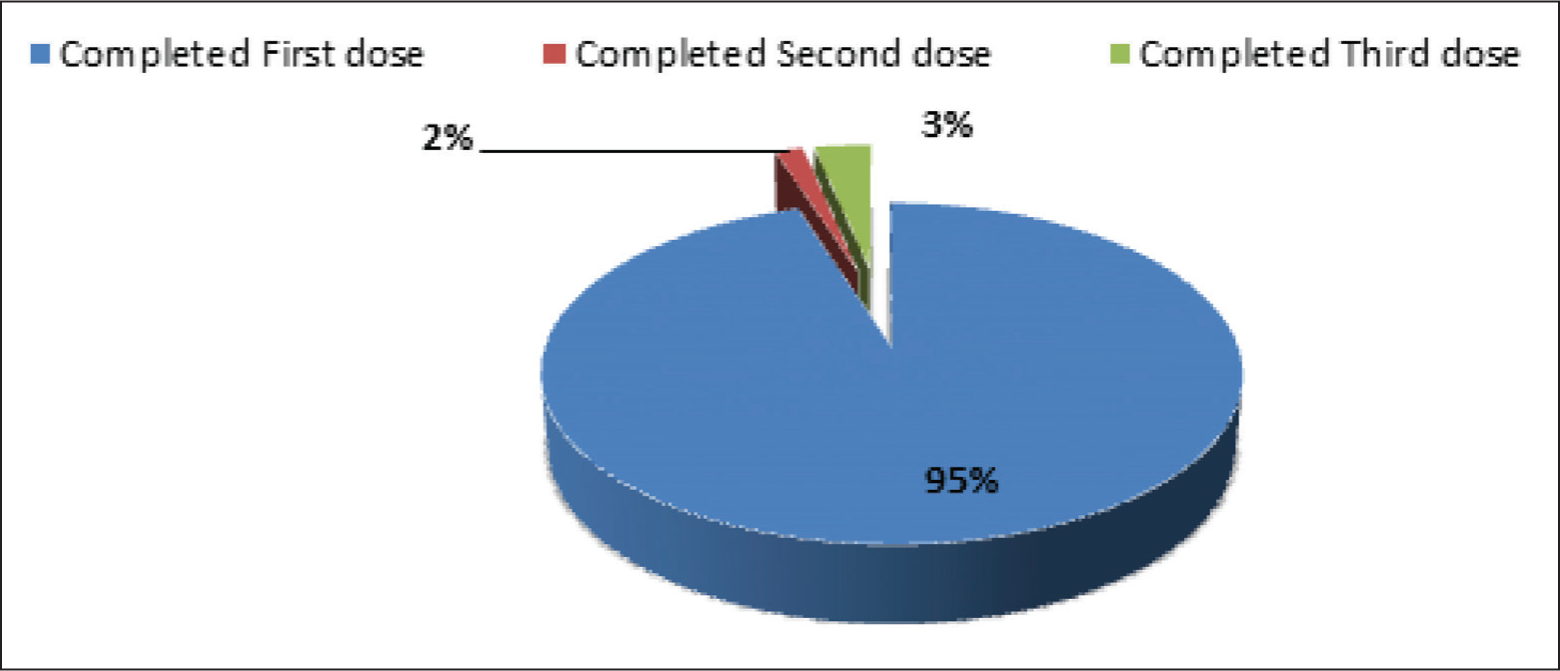
Out of the 79 students who have not taken the Hepatitis B vaccination, 72.15% did not take it because of the lack of vaccination programs offered, 20.25% did not take it because of their lack of knowledge, 8.86% did not take it because of their personal belief and the remaining 2.5% did not take vaccination because of other reasons [Figure 4]. Out of the total 256 students who were vaccinated, 56.25% have taken the complete dose of Hepatitis B vaccination, 28.4% have taken two doses of Hepatitis B vaccination, and 16.42% have taken the first dose of vaccine [Figure 5].
Distribution of study participants according to their reason for not taking vaccination
Distribution of study participants according to the doses of Hepatitis B vaccination taken by them
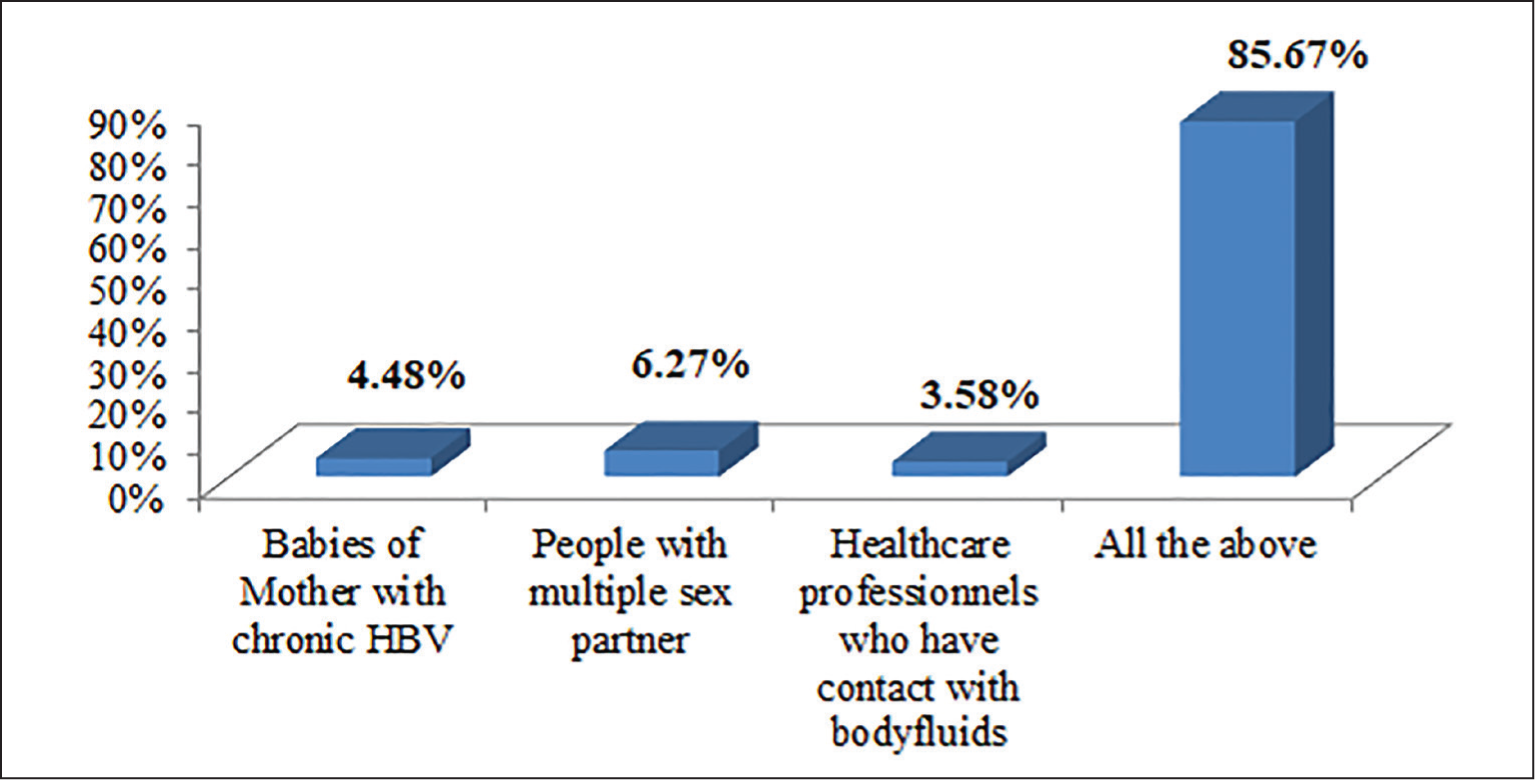
Out of the study participants, 85.67% know the high-risk group for HBV infection [Figure 6]. Among them 45.07% know the recommendation of booster dose for Hepatitis B vaccination, 20.30% know doses of Hepatitis B vaccine protect from any other Hepatitis infection, 27.76% know the best time to take the first dose of Hepatitis B vaccine and 59.8% strongly agree that they need more information about hepatitis B vaccination.
Distribution of study participants according to their knowledge on high risk group for HBV infection

The majority (97.31%) believe hepatitis B vaccination is safe, effective, and ready to take vaccination and recommend it to others. 31.58% of students took the complete course of hepatitis B vaccination and attended hepatitis B vaccination-related awareness programs.
Out of the total students who responded, 30.7% showed good knowledge, 34.4% had a good attitude, 38.8% students had good a practice, and there exists a significant association between knowledge, attitude and practice of Hepatitis B vaccination among these students [Table 1, 2].
Association between knowledge and attitude

Association between attitude and practice

Discussion
Everyone agrees that having access to health services and information is essential as a fundamental human right. All people must have access to high-quality services for their health as well as the health of their families and communities for health for all to become a reality. Achieving universal health coverage (UHC) and choosing what to cover depends on the requirements of the populace and available resources in each nation [5]. The World Health Organisation (WHO) predicts that there will be 1.5 million new cases of chronic hepatitis B each year and 296 million infections globally in 2019. Hepatitis B caused an estimated 820,000 deaths in 2019, with cirrhosis and hepatocellular carcinoma (HCC, primary liver cancer) accounting for the majority of these deaths. A total of 30.4 million people, or 10.5% of those expected to have hepatitis B, were aware they had the illness as of 2019, and 6.6 million people, or 22% of those who had been diagnosed, were undergoing treatment. The percentage of children under five who had chronic HBV infection fell to less than 1% in 2019, according to the most recent WHO estimates [2]. This is compared to over 5% in the pre-vaccine era from the 1980s to the early 2000s. Our study concentrated on practice, attitude and knowledge.
Of the students 335 responded, 68% accounted for females and 32% for males. Among them 46.6% were medical, 38.2% were dental, 26.78% were nursing and 7.5% were physiotherapy students. Also, 58.8% belong to the rural area, and 41.2% belong to urban areas. Results showed that out of the respondents, 76.4% of students were vaccinated, and the remaining 23.6% were unsure about their vaccination status. Out of the total immunised students, 34.03% have taken the complete dose of Hepatitis B vaccination. According to a study by Khan N et al.,[6] the positive attitude towards vaccination among medical staff is more than that of paramedical staff. Twenty-seven medical staff and 13 paramedics had a complete vaccination; the others either did not receive the vaccine or had an incomplete schedule. In this study, 40.29% were aware of Hepatitis B vaccination through awareness programs, 41.9% through lectures, 8.95% through social media, and the remaining were from other sources. Based on the findings of our study, most of the students (41.7%) got information from lectures, which is higher than the studies shown in hospitals in Gujarat. Abdela et al.[7] found that the paramedical worker was the respondent’s primary information source.
Out of the study participants, 85.67% know the high-risk group for HBV infection. Among them, 45.07% see the recommendation of booster dose for Hepatitis B vaccination, 20.30% know doses of Hepatitis B vaccine protect from any other Hepatitis infection, 27.76% know the best time to take the first dose of Hepatitis B vaccine, and 59.8% strongly agree that they need more information about hepatitis B vaccination. The study participants belong to the top most literate state in the country, but the students did not have any clue about their vaccination status even though the universal immunisation program in India started way back in 1985. The students of the present study belong to the category of people who were born after 2000 AD. That means most of them belong to the second generation of the population who had undergone vaccination in India after the implementation of the universal immunisation program. Since Kerala is a 100% literate state, most of the parents of the students were graduates and above which in terms has resulted in good primary care practices in the country. The success of the vaccination programs in the country was evaluated according to the vaccination coverage. The coverage in terms belongs to the decision of the parents who had been informed regarding the uses and also the adverse events following immunisation. In a study by Al-Thaqafy et al.,[8] 92% of participants said they knew something about HBV, and 59.8% said the virus was the cause of HBV. Individuals who reported they were not at risk of contracting HBV were those whose mean score was less than 2.2174. The majority of individuals responded that the HBV vaccine aids against contracting HBV above the mean score (mean > 3.65). Nonetheless, the overwhelming majority of participants—55.4% reported that they had never gotten the HBV vaccine, and 51.1% said they had never attended an informational session on HBV to learn more about hepatitis. These results are consistent with those of a study done by Nagpal et al.[9]
Yasobant et al.[10] reported that 44.5% had good knowledge of hepatitis B vaccine. According to a study conducted by Atlam et al.,[11] among Tanta University medical students in 2016, the study included 185 students; more than half (57.85%) of the participants have sufficient knowledge about Hepatitis B vaccination. In this study, out of the total students who responded, only 30.7% showed good knowledge, 34.4% had a good attitude, 38.8% had good a practice and there exists a significant association between knowledge, attitude and practice of Hepatitis B vaccination among these students. There is a need to increase awareness about the importance of vaccination against HBV at the beginning of the course. Implementing strategies for prevention, promoting the practice of simple hygienic measures, preclinical vaccine checking and provision of HBV vaccine to non-vaccinated students are required. The students in our study were also asked to check their vaccination history with their parents. They were also asked to check their vaccination history with the vaccination cards at their home. The vaccination status of Hepatitis B can be known from the vaccination card. Few of the students had gained knowledge regarding the universal immunisation program when they cross-checked with the vaccination card. While assessing the knowledge on hepatitis coverage, most of the (80%) students opined that hepatitis B vaccination will cover all hepatitis. The knowledge regarding primary prevention of a vaccine-preventable disease is not in an acceptable range. This shows that there is a need for aggressive social marketing regarding vaccinations. Although the Government of India provides most of the childhood vaccinations free of cost. There are challenges and vaccine hesitance among various categories of people. There is a role for religion in vaccine hesitance and the decision whether to get vaccinated or not. This can be overcome by proper health education. The role of education among the parents has helped in making them understand the uses of vaccines.[12] Thus, when there is an increased literacy rate, it also reflects in the rate of vaccine coverage, but there is a religious role. About 60% of the students agreed that they need more information regarding hepatitis B vaccination. This is in terms of a reflection that there is an unmet need for UHC to be successful at a global level.
Conclusion
Approximately 350 million individuals worldwide are chronic HBV carriers. Acute and chronic illnesses including cirrhosis and HCC can be brought on by the infection. The WHO advised that all nations should include the HBV in their regular baby and childhood immunisation regimens by the end of the 20th century.[12] According to our research, there is a need to raise awareness at the start of the course about the significance of receiving an HBV vaccination. To increase the understanding, attitude and practice surrounding the Hepatitis B vaccination, preventive strategies, simple sanitary measures, preclinical vaccine checking, and giving the HBV to students who have not had it yet are all necessary. Kerala state may have the highest educational attainment in the nation, but not in terms of health literacy.
Footnotes
Acknowledgements
The authors thank all the participants who consented to the data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
MMCH&RC/IEC/2021.
CRediT Author Statement
The study conception, design, data collection, analysis and interpretation of results and draft manuscript preparation were done by all the authors and they reviewed the results and approved the final version of the manuscript.
Data Availability
All data analyzed during this study are included in this article.
Use of Artificial Intelligence
No.