
Abstract
Background:
Maternal height has been for long a contributory anthropometric factor that can determine the obstetric outcome. There is always a need of a consistent, reliable, and simple risk indicator which is easy to use for preventing unnecessary complications in a country like India where often antenatal care is provided by dais in rural areas. The background of this research aims to ascertain the relationship between maternal height and mode of delivery based on other intrapartum factors which influence labor and consequent maternal and neonatal outcome.
Materials and Methods:
All primigravidae at term gestation (>37 weeks) with cephalic presentation on admission to labor suite with no other comorbidities were recruited in the study. Their mode of delivery, maternal outcome, along with neonatal outcome was documented.
Results:
Out of the 680 patients, 104 patients are considered for the short-stature group (15.29%) who were <150 cm in height. Other group comprised patients who were >150 cm in height, a total of 576 (84.71%). There was a higher incidence of induced labor in the study group (66.35%) and emergency lower-segment cesarean section done due to cephalopelvic disproportion (CPD) (60%) was also higher among the short-stature group. The incidence of normal labor (32.99%) was higher in the tall-stature group.
Conclusion:
Short height (<150 cm) is an independent risk factor for cesarean delivery due to CPD. Statistical correlation was found between mothers of short stature and babies being born with low birth weight. As labor is influenced by multiple factors, it is fair enough to give a trial of labor for short primigravidae except in uncommon circumstances.
Introduction
Pregnancy is a normal physiologic process that can be complicated by an interaction of several factors innate to the woman. Maternal height has been for long a contributory anthropometric factor that can determine the obstetric outcome. Medically, an adult height that is more than 2 standard deviations below the mean for gender and age is defined as short stature. Different studies, including meta-analysis conducted by the World Health Organization, mentions 145 cm as the constant value for the determination of short stature among women.[1-3]
Almost 800 women/day die due to preventable causes during pregnancy, 99% of these deaths are contributed by developing countries. Many adult females have a history of malnourishment in childhood, maybe because of which, they are short-statured in adulthood and thus may have unfavorable perinatal outcomes.[2] Numerous studies have stressed on the importance of the maternal height and its effect on the course of labor and subsequent perinatal outcome. There are studies in India that showed a birth weight variation of 216 g between tall (>162 cm) and short (<143 cm) antenatal women.[4,5] There are some data that maternal short stature is associated with low birth weight (LBW) in Caucasians, but there is limited information among the South Asian population. Maternal short stature in itself is recognized to increase the risk of obstetric complications such as cephalopelvic disproportion (CPD), arrest of labor, higher rates of cesarean sections, intrauterine asphyxia, intrauterine growth retardation, and low APGAR scores.[6,7]
It is important for the obstetrician to identify the women who are at a risk for increased pregnancy and delivery complications. Precautionary measures should be taken for those at high risk, and delivery should be planned at higher medical centers.[8,9] A specified height can be defined under which attention can be paid to the risk of CPD. Second-stage labor is very important in the clinical course of labor. Vigilant management of labor after considering factors such as age, body weight, and height, age of the patient can help achieve a successful outcome.[8-10]
Various studies have highlighted maternal stature as an independent measure, in which some articles have concluded that height below 150 cm is associated with higher perinatal mortality. Some investigators considered the fact that the use of maternal height as a screening tool has low sensitivity and specificity, so they doubted the practical value in assessing CPD.[11-13] Women who land up in CPD tend to undergo surgical interventions such as vacuum or forceps delivery or emergency cesarean deliveries, which can cause considerable maternal morbidity in addition to economic burden and stress on the family. To minimize this maternal-fetal trauma that accompanies this emergency, it is important for the obstetrician to identify who is at a risk of CPD. Working toward this, numerous investigators have tried to find indices to identify high-risk antenatal women.[14,15]
There is always a paucity of maternal medical services in India. Antenatal care is provided by a traditional dais in rural areas. To prevent unnecessary complications, there is a need of an indicator of risk, which has reliability and consistency as its main characteristics and it is easy to use. Maternal height is one such measurement that can be considered, as it is a nonmodifiable risk-causing factor, and it reflects the nutritional status of an individual during childhood and adolescence and there could be other genetic influences also, which can lead to altered perinatal outcomes.[16,17]
The objective of this study is to ascertain the relationship between maternal stature (height) and mode of delivery based on other intrapartum factors which influence labor and consequent maternal and neonatal outcome.
Materials and Methods
A prospective, observational study was undertaken at G Kuppuswamy Naidu Memorial Hospital in Coimbatore from December 2019 to August 2020. With a 95% confidence interval, a z = 1.96, and a 10% attrition rate, the sample size was computed, and 680 pregnant women were included in the study that were primigravidae at term gestation on admission to the labor suite and provided informed consent before enrolling in the study. The study included singleton pregnancies, term gestation >37 weeks, and cephalic presentations, whereas noncephalic presentations, intrauterine death, intrauterine growth restriction, malpresentations, malpositions, twin gestations, preterm labor, fetuses with congenital anomalies, mothers with other pregnancy-related complications such as preeclampsia and gestational diabetes mellitus, and cases of elective cesarean were excluded from the study. After applying the inclusion and exclusion criteria, 680 patients were selected and internally compared to study the association of maternal height status with mode of delivery and prenatal outcomes. All antenatal women with a height of <150 cm were included in the study group and those above 150 cm were included in the control group.
From the antenatal case records, prepregnancy height (in cm) and weight (in kg) were obtained. At the time of the booking visit to our hospital, the woman was measured for height using a stadiometer that was accurate to 0.1 cm. Accordingly, the body mass index (BMI) was determined. Additional information regarding the progress of the labor, whether it is spontaneous or induced, is noted. Several intrapartum observations were made, including changes in cardiotocography (CTG) and liquor color. The subsequent choice of method of delivery – whether vaginal, instrumental, or cesarean – was documented. CPD, lack of labor progress, unsuccessful induction, and fetal distress were the categories for the indications for cesarean delivery. Weight-, sex-, and other birth-related information like APGAR are documented. There are complications, including postpartum hemorrhage and perineal tears. Babies who required newborn intensive care admission for a variety of reasons were observed and recorded. Taking all of the above factors into account, the relationship between short stature (defined as 150 cm) and mode of delivery and maternal and fetal outcomes was derived. All data were coded and put in a master spreadsheet for statistical analysis using acceptable statistical procedures. SPSS Inc. Released 2007. SPSS for Windows, (Version 16.0. Chicago, SPSS Inc.) was used to analyze the data. All data were subjected to descriptive statistics, which were given in the form of mean values and percentages. Suitable statistical comparison tests were carried out. The unpaired t-test was used to examine continuous variables. The Chi-square and Fisher’s exact tests were used to examine categorical variables. The statistical significance level was set at P = 0.05. Microsoft Excel 2007 was used to generate charts.
Results
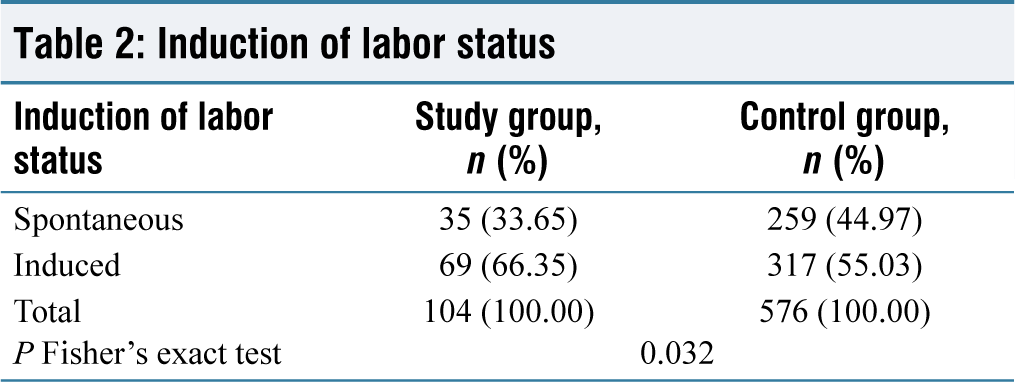
In our study of 680 people, the overall incidence of short stature (150 cm) (study group) was found to be 15.29% (n = 104), and the incidence of tall stature (>150 cm) (control group) was found to be 84.71% (n = 576). Patients in the study group had an average age of 26.11 years, while those in the control group had an average age of 26.01 years. In terms of age distribution, there was no statistically significant change. The prevalence of booked status was 82.69% (n = 86) in the study group and 87.50% (n = 504) in the control group. There was no statistically significant difference in the distribution of booked status between the two groups. The control group’s mean weight was 71.64 kg, compared to 61.98 kg for the study group. Regarding weight distribution, a statistically significant difference was observed. Between the maternal height research groups with an unpaired t-test P = 0.05 [Table 1]. Patients in the study group had a mean prepregnancy BMI of 26.97, while patients in the control group had a mean prepregnancy BMI of 26.93. There was no statistically significant difference between the two groups in terms of prepregnancy BMI distribution. Reactive CTG was more common in both the study group patients (n = 88, 84.62%) and the control group patients (n = 502, 87.15%), revealing no statistically significant difference. When comparing the status of the different groups’ liquor colors, the majority of study group patients had a greater incidence of clear liquor (n = 90, 86.54%) and Grade 2 meconium liquor (n = 7, 6.73%). Similarly, most of the patients had a higher incidence of clear liquor (n = 495; 85.94) in the control group, but there was no statistical difference. Induced labor occurred more frequently in the Study Group patients (n = 69, 66.35%) than spontaneous labor (n = 35, 33.65%). Furthermore, the control group’s patients tended to experience more induced labor (n = 317; 55.03%). According to Fisher’s exact test, there was a statistically significant difference between the maternal height study groups in terms of the status of induction of labor, with a P = 0.05 [Table 2].
Weight distribution among the two groups
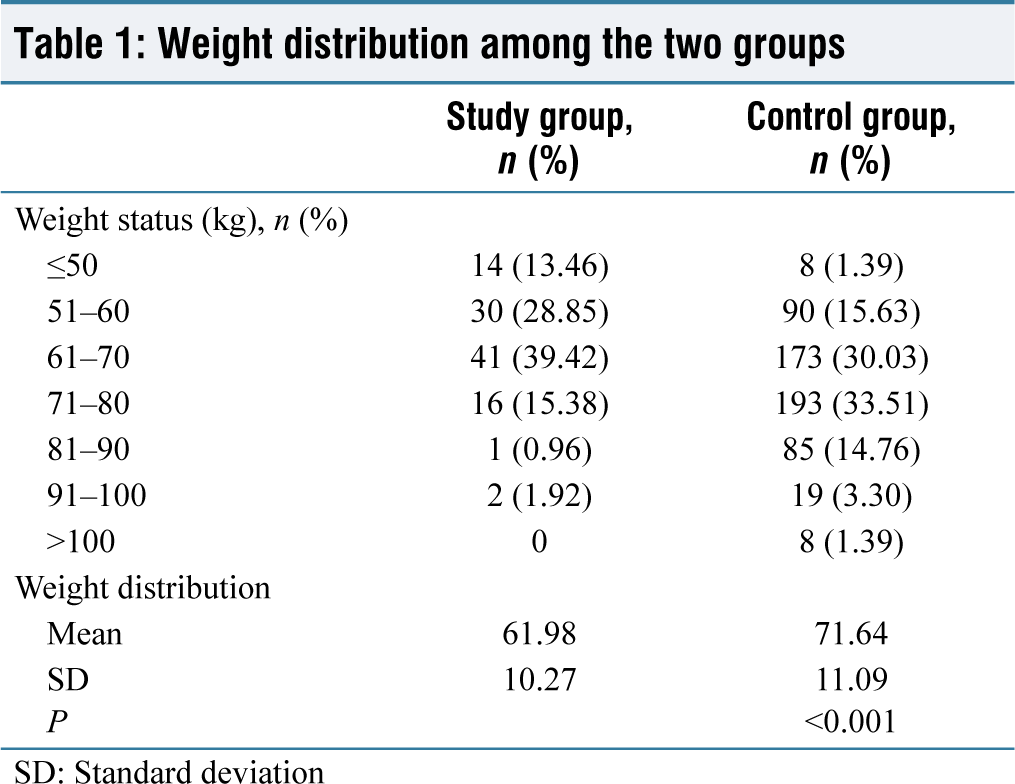
SD: Standard deviation
Induction of labor status
The mean gestational age of the study group and control group is 40.72 weeks and 40.77 weeks, respectively, showing no statistical difference between the groups in terms of gestational age at delivery. The majority of study group patients received emergency lower-segment cesarean section (LSCS) as the mode of delivery (n = 45, 43.27%), followed by vacuum extraction (n = 29, 27.88%). However, in the group acting as a control, regular labor was the most common mode of delivery (n = 190, 32.99%), followed by LSCS (n = 179, 31.08%). According to Fisher’s exact test, there was a statistically significant difference in the mode of delivery status between the maternal height study groups, with a P = 0.05 [Table 3]. Cepahlopelvic disproportion was the most common cesarean (LSCS) indication in the study group (n = 27, 60.00%), followed by fetal distress (n = 12, 26.67%). However, the incidence of cepahlopelvic disproportion as an indicator was (n = 67, 37.43%) and fetal distress was (n = 56, 31.28%) in the control group. According to Fisher’s exact test, there was a statistically significant difference in cesarean (LSCS) indication status between the maternal height study groups, with a P = 0.05 [Table 4]. Mild anemia was more common as a maternal complication in the study group patients (n = 22, 21.155%). Similarly, in the control group, the majority of patients had a greater frequency of mild anemia (n = 108, 18.75%). There was no statistically significant difference between the groups in terms of maternal complication status. Patients in the study group had a mean birth weight of 2.84 kg, while patients in the control group had a mean birth weight of 2.99 kg. According to the unpaired t-test, there was a statistically significant difference in birth weight distribution between the mother-height study groups, with a P = 0.05 [Table 5]. At 1 min, the study group patients had an APGAR score of 7.50, while the control group patients had an APGAR score of 7.69. According to the unpaired t-test, there was a statistically significant difference in birth weight distribution between the mother-height study groups, with a P = 0.05 [Table 5]. At 5 min, the study group patients had an APGAR score of 8.44, while the control group patients had an APGAR score of 8.56. There was no statistically significant difference between the two groups in terms of the APGAR score at 5 min. Patients in the study group had a higher rate of Neonatal Intensive Care Unit (NICU) admission for observation (n = 14, 13.46%). Similarly, in the control group, most patients (n = 98, 17.01%) were admitted to the Neonatal Intensive Care Unit (NICU) for observation. There was no statistically significant difference in NICU admission status between the groups.
Mode of delivery among the two groups
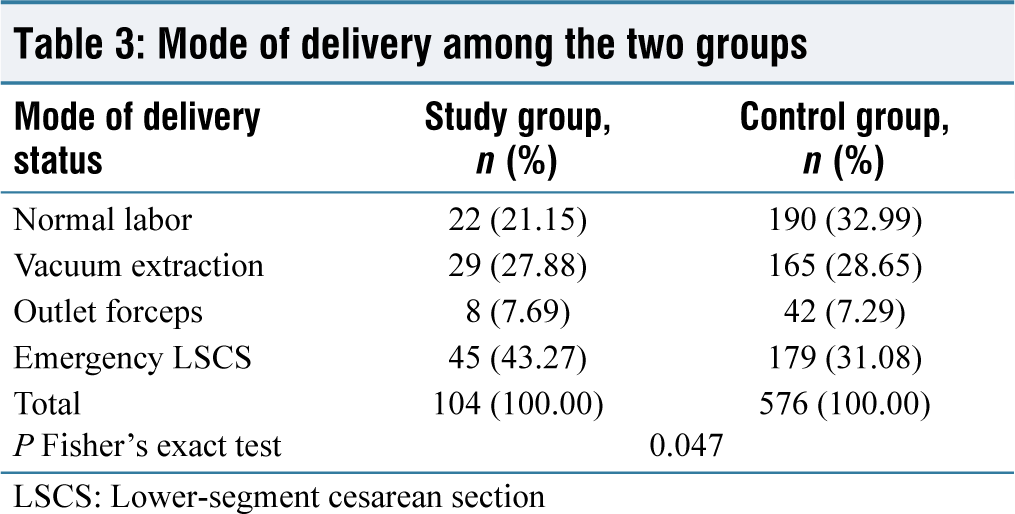
LSCS: Lower-segment cesarean section
Indication of lower-segment cesarean section
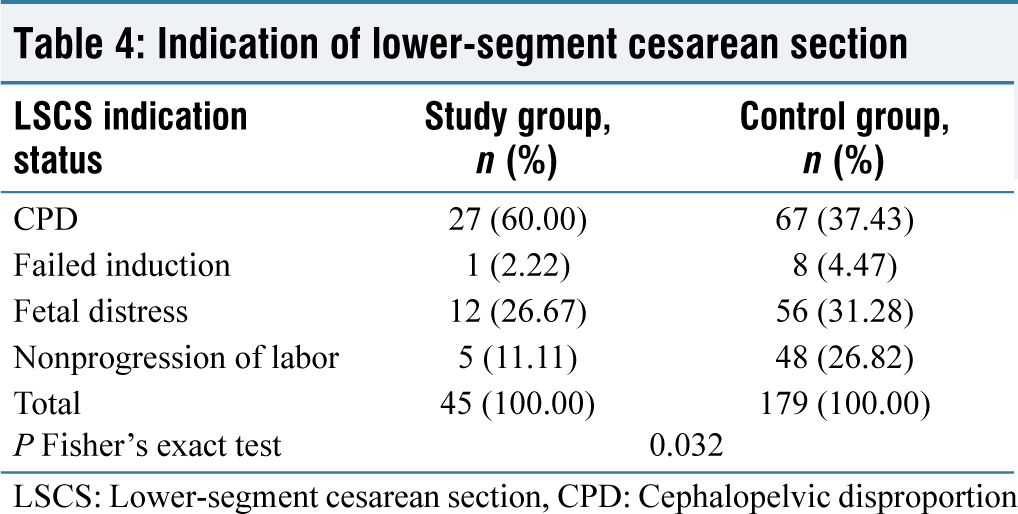
LSCS: Lower-segment cesarean section, CPD: Cephalopelvic disproportion
Maternal and offspring factors (birth weight, APGAR at 1 min and APGAR at 5 min)
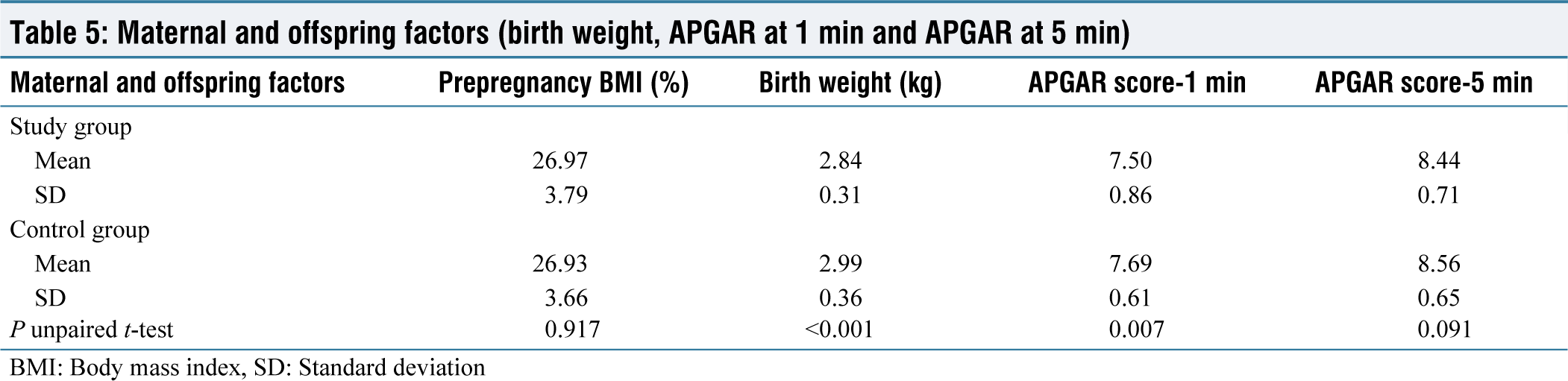
BMI: Body mass index, SD: Standard deviation
Discussion
A remarkable gynecological literature has shown short stature to influence labor outcomes and was related to cause obstetric complications and eventually increased incidence of cesarean delivery. Several authors over the past few decades have tried to establish an association. Nevertheless, in this study, after observing the results supported the theory that maternal short stature has a significant association with the mode of delivery.[18-20]
Age, booked status, CTG status, the color of liquor status, gestational age at delivery, maternal complications, prepregnancy BMI, APGAR score at 5 min, and NICU admission status study variables failed to show any significant difference and effects on outcomes when data gathered in our study was analyzed. The same view was echoed by Marshall et al.’s and Solomon et al.’s studies.[20,21]
In a study by Ratnasiri et al. stated that there were adverse perinatal outcomes at extremes of both BMI. They also stated that as BMI increases, there might be an increased risk of cesarean delivery. Pre pregnancy weight was shown to be higher in short-stature group, but BMI showed no much difference in both groups.[22]
Increase in prepregnancy weight could be a sampling error or might have occurred by chance. Since BMI is the most reliable measure, it is taken into consideration and as it did not differ much, it might not cause a striking difference in the outcomes. The study by Kalk et al. showed that there was an increased rate of neonatal admission in babies born to low-birth-weight mothers. In this study, though there was not much difference between these variables and also they were not related to NICU admissions.[23]
The incidence of emergency LSCS as mode of delivery (primary outcome variable) was significantly higher in short-stature group patients, in comparison to the tall-stature group patients by 28% (43.27% vs. 31.08%, respectively). Our findings are consistent with the ones of Arendt et al., suggesting an inverse relationship between the rate of cesarean section and maternal stature.[24]
The incidence of normal labor in comparison group participants (n = 190, 32.99%) was higher compared to short-stature group, where the incidence of normal labor was much lower (n = 22, 21.5%). Sheiner et al. reported a higher cesarean delivery, even after controlling dystocia in mothers <150 cm compared to their taller counterparts. The association between cesarean delivery and short stature can be explained by CPD and the same study pointed out that this may influence the obstetrician s decision regarding the mode of delivery. The authors further pointed out that the risks of cesarean delivery should not be forgotten, that it can be an impending obstetric hazard and might increase maternal morbidity.[25] Maternal height reflects the maternal pelvic size, which is directly related to dystocia; hence, it has been shown to be a predictive marker of obstructed labor. Hence, increased labor induction in a preventive mode, primarily not rather as a response to the standard indication, is more beneficial to both mother and the child.[25,26]
In a study done by Govind et al., similar conclusions were drawn regarding the incidence of LSCS due to CPD. 53% of mothers below the height of 145 cm landed up in CPD compared to my study in which 60% had CPD in mothers with height <150 cm who landed up in emergency LSCS.[25]
The mean birth weight was significantly less in short- stature group patients in comparison with the tall-stature group patients by 5% (2.84 kg vs. 2.99 kg, respectively). Our results were consistent with the findings of Britto et al., which highlighted that there was a difference of 125 g of weight between the children of short-heighted mothers and the children of tall heighted mothers (3.18 ± 0.56 kg vs. 3.30 ± 0.58 kg, respectively).[27] It can be assumed that mothers with short stature, had a higher risk of having babies of lower birth weight than the ones with tall height. In a study done by Rochow et al., average birthweight significantly varies based on the region of origin.[28] To simplify it more, the study staBrittoted that within a region of origin, the average birth weight differs among different maternal heights. However within the same height group and women of different regions of origin, average birth weight did not show a significant difference.
In this study, the comparative LBW might be due to the babies being constitutionally or genetically small. Bisai et al. identified newborn size was heavily impacted by maternal stature.[29] The relation to LBW and short stature had been described in various studies decades ago. Kader et al., in their study, tried to identify the significant nutritional and socioeconomic determinants associated with LBW and found that short stature in mothers, especially <145 cm are associated with LBW infants.[30]
The mean 1-min APGAR score was significantly less in short-stature group patients in comparison with the tall-stature group patients by 2% (7.50 vs. 7.69, respectively). The 5-min APGAR score, when compared amongt two groups, the short-stature group participants’ mean APGAR score was 8.56 and the other group participants’ mean value was 8.44. No significant difference in relation to the 5 min APGAR score was established. There was no significant evidence of the difference among NICU admission status and the 5 min APGAR score between the two groups, the statistically significant values at 1 min APGAR are of least importance and can be ignored. In comparison to the study by Syed et al., intra-uterine asphyxia, intrauterine growth retardation, and low APGAR scores were more prevalent among the babies of short-heighted mothers rather than the normal-statured ones.[31] It can be assumed that short-statured mothers showed a higher risk of CPD, leading to a prolonged second stage of labor with increased chances of low Apgar score at 1 min.
Conclusion
Based on the results obtained, our study highlighted that short stature is independently related to the risk of induction of labor. Furthermore, we determined a significant correlation between short stature and babies being born with a lower weight. As labor is influenced by multiple variables, it might be reasonable to give all primigravidae, regardless of their height, a fair trial of labor except in uncommon circumstances. Selecting a cutoff height as a screening tool for categorizing patients and identification of the patients who have a greater probability of landing up in obstetrical complications could be useful, as height is one of the many factors which affects the mode of delivery and outcome of labor.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Ethical Committee Approval Number
GKNMH/Admin/DNB/2019TP dated December 04, 2019.
CRediT Author Statement
Dr. Apoorva Anil Gummadi – Concept of Study, Data Collection, Manuscript Writing and Editing; Dr Sandhya Sunkaraneni-Data Collection, Manuscript Writing and Editing; Sai Kiran Kuchana-Data Collection, Manuscript Writing and Editing Kode Rohith-Manuscript Writing and Editing; Muhammad Riyyan-Manuscript Writing, Editing, Submission.
Data Availability
All data underlying the results are available as a part of this article and no additional source data are required.
Use of Artificial Intelligence
There was no use of Artifical Intelligence.