
Abstract
Background:
Distal renal tubular acidosis (dRTA) is a condition characterized by the impaired ability to secrete hydrogen ions from the distal tubule. In pediatric patients, common clinical features of dRTA include excessive urine production (polyuria), frequent nighttime urination (nocturia), poor growth and weight gain (failure to thrive), difficulty with bowel movements (constipation), abnormal breathing, and the presence of kidney stones (nephrolithiasis). While urinary tract infections (UTIs) are frequently associated with dRTA, renal failure is uncommon and seldom reported in children.
Case Presentation:
A 10-year-old girl was referred for the evaluation due to a progressive loss of gross motor milestones over a period of 3 years. She also experienced an acute episode of paralysis and was found to have bilateral medullary nephrocalcinosis (right staghorn calculus) accompanied by moderate renal failure and a UTI. Her development in other areas was appropriate for her age. Importantly, there was a history suggestive of excessive urine production (polyuria), increased thirst (polydipsia), and frequent nighttime urination (nocturia). Physical examination revealed proximal myopathy, characterized by a waddling gait and a positive Gower’s sign, as well as diminished reflexes and muscle tone in the lower limbs. Laboratory tests indicated the presence of sepsis (total leukocyte count – 26,660, CRP-174.29) and elevated renal parameters (serum creatinine – 4.27) along with active urinary abnormalities. Urine culture and sensitivity testing showed significant growth of Escherichia coli (>100,000 CFU). A computed tomography scan of the kidneys, ureters, and bladder revealed a staghorn calculus on the right side, as well as bilateral medullary nephrocalcinosis and swollen kidneys. The patient was diagnosed with dRTA based on several factors, including hypokalemic hyperchloremic metabolic acidosis with a normal anion gap, high urine pH, borderline hypercalciuria, presence of medullary nephrocalcinosis, and after ruling out other potential differential diagnoses. Following treatment for the UTI and sepsis, as well as standard treatment for dRTA, the child exhibited symptomatic improvement. Her creatinine levels returned to 0.8 mg/dL, and the septic markers declined to normal levels. To further investigate the cause of the initial decline in renal function in addition to the UTI, a renal biopsy was performed.
Conclusion:
This case report emphasizes the significance of including medullary nephrocalcinosis and renal tubular acidosis in the list of potential diagnoses for patients presenting with progressive gross motor developmental regression, acute flaccid paralysis, and proximal myopathy. Timely identification of these conditions can help avoid unnecessary and expensive investigations, while also facilitating prompt clinical recovery in affected children. Early diagnosis plays a crucial role in guiding appropriate management strategies and improving patient outcomes.
Introduction
Renal tubular acidosis (RTA) is a group of disorders characterized by the development of hypokalemic metabolic acidosis with a normal anion gap. These conditions arise due to defects in the renal tubules’ ability to either reabsorb bicarbonate or excrete hydrogen ions in response to acidemia.[1,2] Common clinical manifestations of distal renal tubular acidosis (dRTA) in pediatric patients include failure to thrive, polyuria, constipation, rickets, and nephrocalcinosis. In this case report, we present the case of a 10-year-old child diagnosed with dRTA, who exhibited progressive gross motor developmental regression, medullary nephrocalcinosis, and acute renal failure.
Case Report
A 10-year-old child presented at Apollo Hospitals Guwahati with symptoms suggestive of urinary tract infection (UTI), renal failure, growth retardation, and progressive weakness of the extremity muscles. The child was delivered through normal vaginal delivery without any perinatal complications, and her birth weight was 2.9 kg. She was exclusively breastfed from birth and introduced to solid food at 6 months of age. The child received vaccinations as per the recommended schedule until 1.5 years of age. She is the fifth child in the family, and her growth and development were normal until the age of 4 years.
At the age of 4 years, the child began experiencing pain and weakness in both lower limbs. Her growth became stunted, and her activities became limited. Over time, her condition deteriorated, and she became bedridden. She also experienced loss of appetite and weight. When the child reached 10 years of age, she visited an outpatient clinic in Silchar, where she was diagnosed with multiple renal calculi. As a result, she was referred to a higher center for further interventions. The child’s father had been healthy until the age of 45 years when he suddenly experienced chest discomfort and passed away from cardiac arrest. Her mother, sister, and cousins are healthy and do not have any known medical conditions. A 10-year-old girl was referred for evaluation due to a progressive loss of gross motor milestones over a period of 3 years, bilateral medullary nephrocalcinosis (with a right staghorn calculus), moderate renal failure, and a UTI. Her other developmental domains were appropriate for her age. It is worth noting that there was a history suggestive of polyuria, polydipsia, and nocturia.
During the physical examination, the girl exhibited generalized growth retardation, with a weight of 11 kg and a height of 110 cm. Her BMI was 12.3, which falls below the 3rd standard deviation. Figure 1a and b showed the presence of painful joints. Proximal myopathy was observed, characterized by a waddling gait and a positive Gower’s sign. Additionally, diminished lower limb reflexes and muscle tone were noted. Laboratory parameters indicated the presence of sepsis, with a total leukocyte count of 26,660 and a CRP level of 174.29. The girl’s hemoglobin level was 9.5, indicating microcytic and hypochromic anemia. Renal parameters were elevated, with a serum creatinine level of 4.27. Other results included corrected serum calcium of 7.7, serum phosphorus of 7.1, parathyroid hormone level of 141.7, and serum albumin level of 1.9. Active urinary findings were also present. Venous blood gas analysis revealed metabolic acidosis with a pH of 6.9 and HCO3-level of 6 meq/L, accompanied by a normal anion gap of 14 meq/L. The urine pH was 6.5 and the urine anion gap was 30. The initial presentation of renal failure with severe acidosis, as indicated by increased serum creatinine and decreased urine output, was atypical for dRTA.
(a and b) Generalised growth retardation

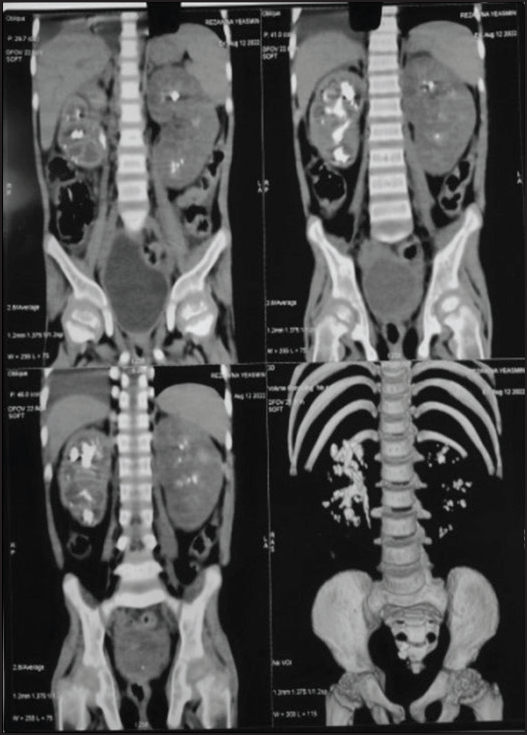
The patient received appropriate treatment, including NaHCO3 infusion, calcium gluconate infusion, intravenous antibiotics, intravenous fluids, and parenteral nutrition. Renal ultrasound revealed bilateral nephrocalcinosis with swollen kidneys. Over the course of 7 days, the patient gradually improved. Fluids were discontinued, and feeding was initiated via a Ryle’s tube. The serum creatinine level decreased to 2 mg/dL, and urine output reached 580 mL over 24 h. The urine culture showed the growth of Escherichia coli (>100,000 CFU), and antibiotics were adjusted based on sensitivity results. Computed tomography scan of the kidneys, ureters, and bladder scan revealed a staghorn calculus measuring 30 × 30 × 23 mm in the right PCS and right PUJ, along with fullness of the right PCS. Bilateral medullary nephrocalcinosis and swollen kidneys (left greater than right) were also observed. The scan also indicated urinary bladder calculi with mild bladder wall thickening and mild pleural effusion on the right [Figure 2]. X-ray of the hands displayed features of rickets, such as widened and frayed metaphysis of long bones [Figure 3].
Computed tomography scan of the kidneys, ureters, and bladder showed staghorn calculus measuring 30 mm × 30 mm × 23 mm in right PCS and right PUJ with fullness of right PCS. Medullary Nephrocalcinosis bilaterally, Bilateral kidneys are swollen (L > R) Urinary bladder calculi with mild bladder wall thickening, mild pleural effusion on right
X-ray of the hands showing features of rickets in the form of widening and fraying of metaphysis of long bones

The diagnosis of dRTA was confirmed based on hypokalemic hyperchloremic metabolic acidosis with a normal anion gap, high urine pH, borderline hypercalciuria, medullary nephrocalcinosis, and the exclusion of other differential diagnoses. The patient experienced symptomatic recovery following treatment for UTI, sepsis, and standard therapy for dRTA. Renal biopsy demonstrated features of acute tubulointerstitial nephritis, explaining the acute kidney injury (AKI) and mixed acidosis. The acidosis subsequently transitioned to hyperchloremic acidosis following the correction of AKI. The patient’s creatinine level returned to 0.8 mg/dL, and septic markers normalized.
Conclusion and Discussion
dRTA in children is primarily a hereditary condition, but it can also occur as a secondary condition due to obstructive uropathies, drug and toxin exposure, and autoimmune diseases. The depletion of potassium in dRTA can be a result of various genetic defects in cellular metabolism, presenting as autosomal dominant or recessive conditions. The common clinical presentations of dRTA in the pediatric age group include polyuria, constipation, failure to thrive, and nephrolithiasis.[3,4] Although acute renal failure is an uncommon presentation of dRTA, any precipitating cause for renal failure should be investigated. In our case, acute pyelonephritis was identified as the cause of AKI, which can sometimes mask the underlying disease and make diagnosis challenging, with limited data available in the literature. In children, dRTA is typically a primary condition with underlying genetic causes, and at least three genes (ATP6V1B1, ATP6V0A4, and SLC4A14) have been identified to be involved in primary dRTA.[5,6,7] However, most patients show catch-up growth after initiating alkaline treatment. In our case, supplementation therapy with alkali, Vitamin D, and potassium normalized the biochemical abnormalities and muscle weakness.
In conclusion, it is crucial to accurately diagnose and effectively manage dRTA in children. The disease has a favorable long-term prognosis when properly controlled. Mortality in cases of dRTA is often associated with complications such as respiratory failure and cardiac arrhythmias resulting from hypokalemic paralysis.[8,9]
Management of dRTA involves the replacement of alkali and potassium, along with treating the underlying disorder if present.[10] This case report emphasizes the significance of considering renal tubular acidosis as a potential cause in the differential diagnosis of acute renal failure accompanied by bilateral medullary nephrocalcinosis and normal anion gap metabolic acidosis. Early diagnosis of dRTA can help prevent unnecessary investigations and facilitate prompt clinical recovery in affected children.[11]
Footnotes
Acknowledgements
We would like to express our gratitude to the Biochemical Department for their valuable inputs and assistance in the biochemical analysis of the patient. Their expertise and contribution have greatly contributed to the understanding and management of the case. We sincerely appreciate their support and collaboration in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Patient Consent
The authors confirm that all necessary consent forms were obtained, which included the patient’s consent for the reporting of their clinical information in a scientific platform. The patient was fully informed that their name and personal details would not be disclosed or published, and reasonable measures would be taken to maintain their anonymity. However, it is important to note that complete anonymity cannot be guaranteed. The authors prioritize patient confidentiality and have taken appropriate measures to protect the patient’s privacy.
CRediT Author Statement
The authors of this manuscript have fulfilled the following criteria:
They have made significant contributions to the concept, design, data acquisition, analysis, or interpretation of the article They have either drafted the article or provided critical revisions that are important for its intellectual content They have given their approval for the publication of the final version They have agreed to take responsibility for the work by addressing any concerns related to its accuracy or integrity and ensuring appropriate investigation and resolution.
These criteria indicate that the authors have actively participated in the research process, manuscript preparation, and decision-making regarding its publication.
Data Availability
No.
Use of Artificial Intelligence
No.