
Abstract
Introduction:
Epilepsy is a well-known disease entity that is responsible for a significant amount of morbidity. The purpose of this research is to determine the frequency of calcium homeostasis abnormalities in patients who are taking chronic anticonvulsant medication and to analyze the levels of Vitamin D in the serum of patients who are taking chronic anticonvulsant medication.
Materials and Methods:
The SVRRGGH general medicine department in Tirupati conducted this cross-sectional single-centered prevalence study. The study included outpatients, inpatients, and acute medical care (AMC) patients. After applying the inclusion and exclusion criteria, the study randomly selected 100 seizure disorder patients from the SVRRGH in Tirupati. Epilepsy patients who participated in the study were asked about medication, compliance, and seizure control. Anticonvulsant usage and duration were recorded. Serum calcium, Vitamin D, alkaline phosphatase (ALP), and parathormone were measured. Hypoalbuminemia caused calcium adjustments. Liver and renal function tests ruled out other major causes of hypovitaminosis D.
Results:
In this study, 36% were hypocalcemic and 64% were normocalcemic. There was a significant association between a number of drugs, duration of up to 12 months, normal Vitamin D levels, and good seizure levels with hypocalcemia (P < 0.001). Around 25% had high ALP levels and 75% had normal ALP levels. High ALP levels were significantly associated with hypocalcemia (P < 0.001).
Conclusion:
Chronic anticonvulsant therapy is associated with significant hypocalcemia and hypovitaminemia D, and our findings suggest that calcium and Vitamin D supplementation might be beneficial for patients experiencing these conditions.
Introduction
Epilepsy causes significant morbidity and is well-known. India’s 5.35/1000 incidence and 49.5/100,000 prevalence rates make it a major public health issue.[1] Long-term use of epilepsy drugs with serious side effects. Since medicine is evidence based, the medical community must assess the side effects. Long-term anticonvulsant treatment is known to disrupt bone and mineral metabolism, resulting in bone mineral density changes. In several anticonvulsant drug-managed populations, 40%–60% have hypocalcemia, decreased serum 25-(OH) Vitamin D, reduced bone mass, elevated serum immunoreactive parathyroid hormone (PTH), and osteomalacia on histology.[2]
Thus, the medical complications of epilepsy treatment, which affect so many of us, cannot be ignored. The current investigation seeks to confirm the above complications and determine biochemically supported pathophysiology. Anticonvulsant drugs alter the liver’s metabolism of Vitamin D and its metabolites, both active and inactive.3,4] Hepatic microsomal enzymes catabolize Vitamin D faster, lowering 25-hydroxy Vitamin D levels. Most long-term anticonvulsant patients have bone mineralization changes. Hypocalciuria, hypocalcemia, decreased 25-hydroxy Vitamin D, increased alkaline phosphatase (ALP), and serum immunoreactive PTH are common laboratory abnormalities. Hypocalcemia and hypocalciuria are common. Clinical observations suggested that the severity of drug-induced calcium and bone metabolism disturbances depended on many factors, including anticonvulsant dose, susceptibility, and therapy duration. These included Vitamin D, exercise, sunlight, and physical activity.[5] Anticonvulsants can lower calcium levels, causing hypocalcemia and bone abnormalities. Hypocalcemia causes seizures. Hypocalcemic seizures are rare but increasingly recognized complications of long-term antiepileptic drug (AED) treatment. When AEDs fail to control seizures, calcium levels are often checked. Hypocalcemia may lower the seizure excitation threshold in epilepsy or subclinical seizure patients. Electroencephalographic patterns can change acutely or specifically. Electroencephalogram changes may occur without calcium deficiency symptoms (hypocalcemia). Hypocalcemia can cause confusion or disorientation in elderly people.[6-8] Phenytoin (PHT), phenobarbitone, sodium valproate, and carbamazepine have been proven to cause disturbances in calcium homeostasis.[7]
As a result, determining the significance of these anticonvulsant drug-induced complications in light of the fact that they are treatable is the rationale for undertaking this study. This significance can be determined through evaluation. The purpose of this research is to determine the frequency of calcium homeostasis abnormalities in patients who are taking chronic anticonvulsant medication and to analyze the levels of Vitamin D in the serum of patients who are taking chronic anticonvulsant medication.
Materials and Methods
After getting the institutional ethics committee (SVMC/March 16, 2021), a cross-sectional single-centered study was conducted at the Department of General Medicine SVRRGGH, Tirupati. Patients who were either outpatients or admitted to medical wards as well as those who received acute medical care, are included in the subjects of the study (AMC).
The study’s inclusion criteria encompass individuals on chronic anticonvulsant therapy to manage epilepsy or seizure disorders, with a specified age range, typically adults (18 years and above). Conversely, the exclusion criteria involve excluding individuals on acute anticonvulsant therapy or with no history of chronic therapy to concentrate on long-term effects. Patients with preexisting calcium-related disorders, pregnancy, lactation, severe comorbidities, or noncompliance with medication or study requirements also be excluded to maintain a more homogeneous study population. In addition, those using calcium supplements were excluded as this could independently affect calcium homeostasis.
Following the application of the inclusion and exclusion criteria, a random selection of one hundred patients with seizure disorders who were attending the SVRRGH in Tirupati was made for the study. Patients who agreed to take part in the research had extensive questions about their epilepsy treatment, including medication, compliance, and seizure control, answered. The information pertaining to the quantity of anticonvulsant usage and its duration, was gathered. It was determined how much calcium, Vitamin D, ALP, and parathormone were present in the serum. In the event that hypoalbuminemia was present, calcium levels were adjusted. To rule out the possibility of other significant causes of hypovitaminosis D, tests assessing liver and renal function were carried out.
Patients who participated in the research project gave their verbal and written consent after receiving appropriate information. The institutional ethical committee at SVRRGGH, Tirupati, gave their stamp of approval to the protocol for this research study. Patients who had been admitted to medical wards, the ambulatory medical center, the intensive care unit, and the emergency room were all part of this procedure. A comprehensive history was taken, and a clinical examination was carried out, as well as a check of the patient’s medical records to verify the presence of any comorbidities, such as coronary artery disease, hypertension, diabetes, and other diseases. There was serum calcium, serum phosphorus, ALP, Vitamin D, and PTH levels were measured in all patients.
Normocalcemia is total serum calcium concentration between 8.6 and 10.3 mg/dL. Hypocalcemia is defined as a total serum calcium concentration <8.8 mg/dL (<2.20 mmol/L) in the presence of normal plasma protein concentrations or as a serum ionized calcium concentration <4.7 mg/dL (<1.17 mmol/L). A range of <75 nmol/L (or 30 ng/mL) of serum/plasma 25(OH) D concentration is considered Vitamin D deficiency.
For the purpose of statistical analysis in this investigation, SPSS version 26.0, (IBM Corp., Chicago, Illinois) was utilized. For the purpose of summarizing patients’ baseline clinical characteristics, descriptive statistics such as percentages, frequencies, means, medians, and standard deviations were utilized. The mean and standard deviation were utilized for the analysis of continuous variables, whereas frequencies and proportions were utilized for the analysis of categorical data. Crosstabs were utilized for the analysis of the comparison of proportions among categorical variables. On the Chi-square test, statistical significance was determined to have been achieved when the P < 0.01.
Results
In this study, 36% were hypocalemic and 64% were normocalcemic. There was a significant association of a number of drugs, duration of up to 12 months, normal Vitamin D levels, and good seizure levels with hypocalcemia [Table 1. In total, there were 36 patients with hypocalcemia who participated in our research; 12 of these patients were younger than 20 years old, 12 patients were between the ages of 21 and 30 years old, 8 people were between the ages of 31 and 40 years old, and 4 patients were older than 40 years old. Eighteen people in the normocalcemia group were younger than 20 years old, 21 people were between the ages of 21 and 30 years old, 19 people were between the ages of 31 and 40 years old, and 6 people were older than 40 years old. It was statistically determined whether or not the patients had hypocalcemia in addition to the number of anticonvulsant medications they had been taking. The prevalence was 14.3% among patients who were only receiving one drug at a time for treatment. Patients who were using two different medications had a prevalence of 70.4%, whereas patients who were using three different medications had a value of 80%. Serum phosphate levels, in addition to serum calcium, were also evaluated. Thirty-one patients out of the studied people had decreased phosphorus levels. Among the 31 patients, 8 people were taking only one drug, 17 patients were consuming two drugs and 6 people were using three drugs. Sixty-nine patients had normal levels of serum phosphorus. After measuring the levels of Vitamin D in the serum of each of these patients, we discovered that out of the 36 patients who were diagnosed with hypocalcemia, 23 of the subjects also had low levels of Vitamin D. However, there were only two people who had hypovitaminemia D in the group that was considered to have normal calcium levels, and the difference in prevalence was statistically significant (P = 0.001).
Distribution of variables among the study participants (n=100)
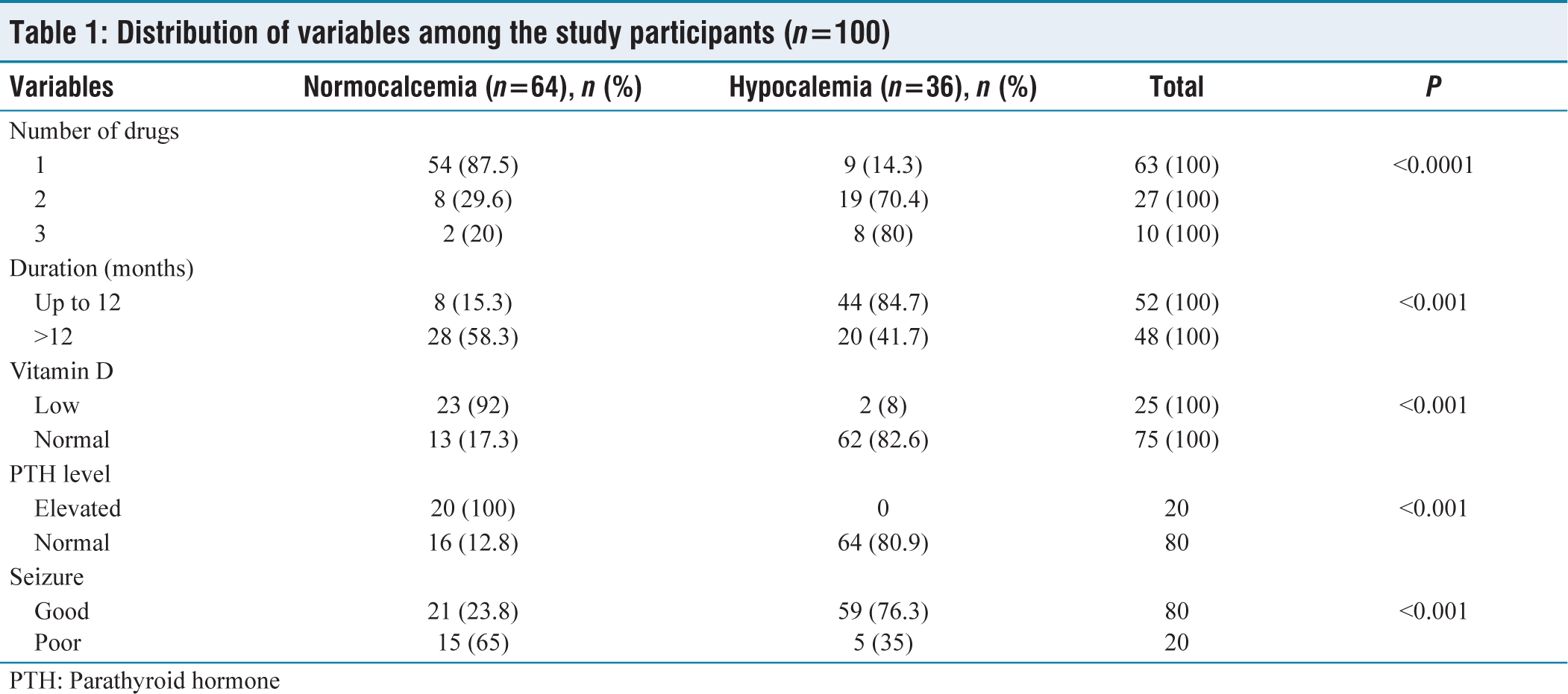
PTH: Parathyroid hormone
Furthermore, the correlation between decreased Vitamin D values and PTH levels was analyzed and it was found that, of the 23 patients with decreased Vitamin D, 13 had elevated PTH values and 10 had normal PTH levels; the number is significant on analysis with P value being < 0.001. Only three patients had normal Vitamin D values and high PTH levels. Seventy-four people had normal Vitamin D and normal PTH levels. The correlation between phosphorus levels in the serum and parathyroid levels was analyzed and was found statistically significant. Among 31 individuals with low phosphorus values, 17 patients had normal PTH levels and 14 patients had high PTH levels. Around 25% had high ALP levels and 75% had normal ALP levels. High ALP levels were significantly associated with hypocalcemia [Table 2.
Relationship of hypocalcemia and high alkaline phosphatase among the study participants (n=100)
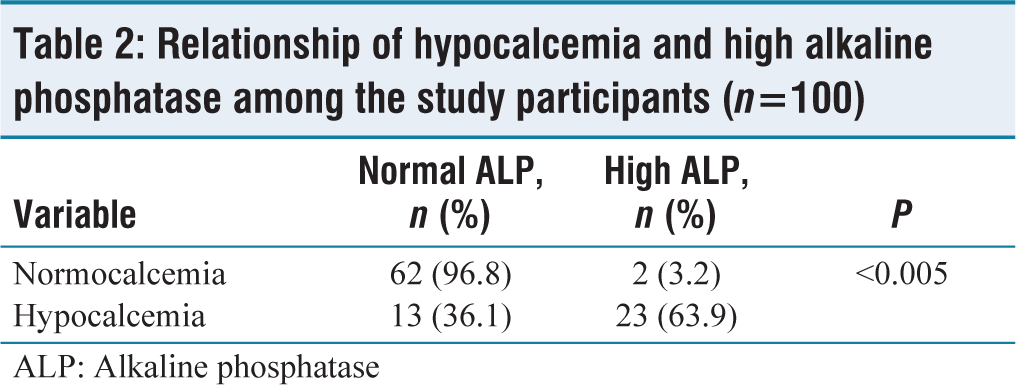
ALP: Alkaline phosphatase
Discussion
The primary purpose of this research project was to investigate and evaluate the prevalence of hypocalcemia in people who had been taking chronic anticonvulsant medication for 12 months. This research was conducted on a total of 100 epilepsy patients who were treated at the Sri Venkateswara Ramnarain Ruia Government general hospital in Tirupati. All of these patients had to meet the inclusion and exclusion criteria that were outlined in the methodology section. In the population that was investigated for this study, the prevalence of hypocalcemia was 36%. Our study was similar to one that had been conducted in the past by Schmitt et al.[9] on 56 patients who were taking chronic anticonvulsants. Out of those 56 patients, it was discovered that 29% (16 patients) had hypocalcemia. In a study conducted by Nandhini[10] and involving the same number of participants, the prevalence of hypocalcemia was found to be anywhere from 3% to 30% among patients who were taking phenobarbitone, PHT, carbamazepine, and sodium valproate.
The number of anticonvulsant medications used was directly associated with the risk of low calcium levels (also known as hypocalcemia), and the differences between the groups were statistically significant (P = 0.001). Our findings were comparable to those obtained in a study of a similar nature that had been conducted by Govindarajan.[11] Sixty-five individuals were taking only a single drug, whereas 27 patients were consuming two drugs, and the rest of the population was taking three drugs. Hypocalcemia was observed in 23 patients who were using two or more drugs, whereas only nine individuals had hypocalcemia while taking a single drug as treatment.
Various studies reported decreased calcium and phosphorus levels due to CYP-450 enzyme by PHT in the liver causing high Vitamin D catabolism. Several reports revealed decreased levels of serum 250HD in children as well as adults taking PHT. Information also prevails regarding the cellular retort to PTH, caused by the inhibitory consequence of PHT on hormone-sensitive adenylate cyclase activity. Hypocalcemia was related to high doses of anticonvulsant drugs, numerous drug therapy, and the usage of individual anticonvulsant drugs in the following order in a study conducted by Dent et al.[12] with increasing order of importance: phenobarbital, PHT, pyrimidine, pheneturide. Subnormal serum calcium levels existed more commonly in individuals with high liver ALP levels. Initial outcomes of medication with calciferol inferred that the disruption of calcium metabolism was the outcome of deficiency of Vitamin D. It is probable that anticonvulsant drugs hasten the Vitamin D breakdown by liver enzyme induction.
It was determined how long anticonvulsants had been used and whether or not the use of the drugs had any impact on the level of hypocalcemia that was present in the patient. About 15.3% of people who had been taking medications for less than a year were affected by hypocalcemia, whereas 58.3% of people who had been using drugs for more than a year were affected by the condition. With a P < 0.001, the difference was statistically significant. This study was limited to evaluating serum calcium levels in patients who were taking anticonvulsant medications. Although the period of duration of drug usage and serum phosphorus were also analyzed, the focus of this study was on serum calcium levels. Seven out of the 31 patients who had low phosphorus levels had been using medications for more than a year, whereas 24 patients had been using medications for a shorter period.
Serum calcium levels were found to have a correlation with serum Vitamin D levels in a separate study that was carried out on 56 patients who were taking chronic anticonvulsants. This study was carried out by Hahn and Halstead.[13] The levels of serum calcium and 250HC were found to have decreased in epileptic outpatients who were receiving chronic treatment with either diphenylhydantoin or phenobarbital, as was demonstrated by this study.
Patients with hypocalcemia were evaluated to determine whether or not they had decreased Vitamin D values. This finding that 21 of the 23 people with hypovitaminosis D had decreased calcium levels, also known as hypocalcemia, was statistically significant. These individuals all suffered from the condition known as hypovitaminosis D. Analyses were performed to determine whether or not there was a connection between the control of epilepsy and the presence of hypocalcemia. The difference in seizure control between patients with hypocalcemia and those with normal calcium levels was statistically significant, with a P < 0.001 indicating the significance of the difference. A patient with mental retardation was examined in a study by Ali et al.[14] to determine whether there were any changes in seizure control as a result of decreased values of serum calcium brought on by long-term treatment with phenobarbitone and PHT. The researchers came to the conclusion that there were no such changes. According to the findings of the investigation, the serum levels of the anti-convulsant medications were appropriate for treatment. In this study, it is imperative to rule out the possibility of subtherapeutic levels of anticonvulsant medication, but this step was not taken. This is one of the problems with the study that we conducted.
We also investigated whether or not there was a correlation between the levels of serum ALP and the administration of anticonvulsant medication. Twenty-five of the 100 patients who were investigated were found to have elevated levels of ALP. Twenty-one patients also had hypocalcemia, accounting for 76% of the total, while the other four, accounting for 24% of the total, had an isolated elevation in ALP values. In the study that was done by Schmitt et al., which was mentioned earlier, a finding that was related to this was reported, and it stated that 27% of the study group had increased levels of ALP.[9] A correlation between low serum vitamin D levels and osteomalacia in epileptic patients consuming long term antiepileptic medications. We also looked at the age breakdown of patients who had high ALP levels as well as those whose ALP levels were normal.
Among the 25 patients with high ALP, 10 patients were male, 15 were female, whereas 40 patients were male and 35 patients were female among the normocalcemia group. Among the patients with increased levels of ALP, 10 patients were below the age of 20 years, eight patients were in between 20 and 30 years, six patients were in between 30 and 40 age group, and only one patient was more than 40 years had elevated ALP.
The elevated serum ALP values were analyzed in relation to the length of time that the patient had been receiving drug treatment and using the medication. When only one drug was used, the prevalence was 15.4%, but when two or three drugs were used, the prevalence increased to 37% and 62.5%, respectively. Therefore, the greater the number of drugs used, the greater the likelihood of elevated levels of ALP. Also taken into consideration was the impact that the length of time on medication had on ALP levels. Those patients who had been taking their medications for less than a year had a prevalence of 15.4%, while those patients who had been taking their medications for more than a year had a prevalence of 35.4%. According to the statistical analysis, every one of the aforementioned values was statistically significant (P < 0.001).
The coincidence of the prevalence of hypocalcemia and raised ALP was analyzed. Of the 36 individuals with hypocalcemia, 19 (59.3%) also had elevated ALP. Raise of ALP alone was found in 6 (8.8%) individuals. There were 12 patients with raised ALP who were on a single drug, whereas nine patients were using two drugs and four patients were consuming about three drugs. Normal ALP values were found in 57 people who were taking only one drug and in 16 people who were using two drugs for seizures. Only two patients had normal ALP levels while consuming three drugs in this study. In our study, nine patients had raised ALP who had taken medication for 12 months and 16 patients had elevated ALP who had taken medication for more than 12 months. The existence of raised PTH in individuals with hypocalcemia was assessed and was seen in half of such patients, with statistical significance.
In our study, serum phosphorus and Vitamin D levels were also analyzed. However, this study has pertained only to the evaluation of serum calcium levels in patients taking seizure medications. Among 31 patients with low phosphorus, 12 patients had normal Vitamin D levels, 19 patients had decreased Vitamin D levels. Four patients had decreased Vitamin D levels and normal levels of serum phosphorus. Sixty-five patients had normal levels of phosphorus and normal levels of Vitamin D. The serum phosphate investigation was done for the patients and it was found that hypophosphatemia was observed along with either a greater number of, or longer period of anti-convulsant treatment and also with hypovitaminosis D and raised parathormone levels. The objective of the thesis was to study the prevalence of hypocalcemia among patients on chronic anticonvulsant therapy (>6 months).
Limitations
Participants in the study were those who were already taking conventional antiepileptic medication. Hence, newer drugs were not studied. Only total serum calcium was analyzed, not the ionized form of calcium, which is the component that plays a significant role in metabolism. To attribute poor seizure control entirely to hypocalcemia, the serum levels of anticonvulsants in patients were not measured. This was done to attribute poor seizure control to hypocalcemia. There was no investigation into the disease pathology that brought on the seizures or their influence on seizure control. When measuring levels of ALP, only the total levels were measured; bone isoenzyme levels were not taken into consideration. The effect of calcium and Vitamin D supplements on epileptic seizures.
Conclusion
Patients who are receiving chronic anticonvulsant treatment have a significantly increased risk of developing hypocalcemia. There is a significant relationship between the incidence of hypocalcemia and both the total number of anticonvulsant medications taken and the length of time that these medications are taken. When compared with normocalcemic patients, hypocalcemia in patients has a significant association with poor seizure control, even in the presence of good drug compliance. Normocalcemic patients have no such association. Either alone or in conjunction with hypocalcemia, elevated levels of ALP were discovered in patients who were undergoing chronic treatment with anticonvulsants. There was a significant correlation between increased ALP levels and the length of time and number of times anticonvulsant drugs were used. This study draws the conclusion that there is significant hypocalcemia and hypovitaminemia D in patients who are receiving chronic anticonvulsant therapy, and we suggest that supplementation with calcium and Vitamin D might be beneficial.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Ethical Committee Approval Number
Sri Venkateswara Medical College -SVMC/March 16, 2021.
CRediT Author Statement
Conceptualization-Rajasekhar G; Manuscript writing-Ketham Reddy Girish Reddy, Gudluru Pujith Kumar; Manuscript revision-D Padma, D Jennifar Evanjalin, Angel Jose; and Proof reading – Rajasekhar G.
Data Availability
All data is contained within the manuscript.
Use of Artificial Intelligence
Authors declare no use of AI in writing the manuscript.